Jonathan S. Black, MD
Objectives
After completing this chapter, you’ll be able to:
- explain the intrinsic and extrinsic causes of surgical wounds that have failed to heal
- describe the reconstructive ladder
- describe how the reconstructive ladder is used to achieve wound closure
- explain the surgical principles that guide care of patients who require skin, tissue, or bone transplantation for wound closure.
Surgical wounds are common in hospitalized patients; however, due to the body’s amazing ability to heal acute wounds, hospitalized patients are seldom seen by wound care specialists unless their wounds have failed to heal. This chapter addresses common surgical wounds, complex wounds healed via surgical procedures, and surgical wounds that have failed to heal in a timely manner.
Extrinsic and Intrinsic Causes of Nonhealing Wounds
Causes of nonhealing wounds can be grouped into two large categories: extrinsic and intrinsic. Extrinsic causes are those factors that exist outside of the wound itself, such as pressure, ischemia, smoking, and malnutrition. Intrinsic factors exist within the wound, such as infection, tension, and arterial insufficiency. Determining which of these factors is present in a wound is an important initial step in wound care. Removing any obstacles to healing is also important; local treatments won’t be effective in healing the wound if the underlying cause of the disruption in healing is not addressed.
Wound care focuses on removing the obstacles to healing. Although wound care has seen technological advances, the great 16th-century surgeon Ambrose Paré is still correct in that we as healthcare providers don’t heal wounds, we create them and nature heals them.1 Indeed, our role is to support the body so that the wound can heal. Wound care practitioners must exercise caution when moving too quickly into treatments for wounds until the underlying causes of the delay in wound healing are fully understood.
Wound History
There are four major questions that need to be addressed by the clinician:
1. How and when did the wound occur?
2. When did the wound’s healing trajectory change from normal to abnormal and why?
3. What known factors are obstructing the wound from healing?
4. What therapies have been attempted?
When examining a patient with a nonhealing surgical wound, it’s imperative that the initial reason for surgery and the operation performed be fully understood. The answers to the following questions must be clear in the examiner’s mind: What was the preoperative condition that required surgery? For example, did the patient have gastric bypass or repair of ruptured abdominal viscera? What was the patient’s condition before surgery? Was the patient healthy or was the patient chronically ill due to diabetes or cancer? What was the intended operation? Were organs or tissue removed? Was the operation clean or contaminated (e.g., penetrating trauma, perforated diverticulum)? Were foreign materials implanted? Was the operation carried out as planned? For example, has the wound been closed with permanent sutures or mesh? Has healing been occurring along a normal trajectory until now? If so, what has happened to alter the course of healing? What medications is the patient taking that might impact healing? Has the nutritional status of the patient been normal since surgery? Was it normal prior to surgery?
From this initial assessment, a comprehensive understanding of the patient who has the wound, not just the wound itself, will be obtained. And, although treating the wound is of utmost importance, treating the patient, whose body will heal the wound, is equally imperative.
Goals of Care
For acute wounds, wound closure with the return of form and function is the usual goal of care. Left alone to close via contraction and scar formation, wounds seldom have either form or function and will often recur and look unpleasant. The ability to reach ideal and complete healing without scarring, such as seen in fetal wounds, is currently impossible. All full-thickness skin injuries heal with a scar. Therefore, the return of acceptable healing with sustained function and anatomic continuity becomes the ideal end point. The surgeon is constantly mindful of the consequences to leaving the wound open, balanced against the consequences of surgical closure and undergoing anesthesia.
Reconstructive Ladder and Planning Reconstruction
A decision-making process in choosing the appropriate method to achieve wound closure is based on the following information and the “rungs” of the reconstructive ladder (Fig. 18-1). Following are some important questions to consider.
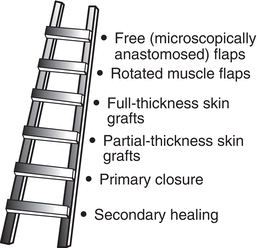
Figure 18-1. Reconstructive ladder. The reconstructive ladder is used to determine the method to replace missing tissue from a wound bed. The ladder shows the simplest method—simply allowing the wound to heal on its own—at the bottom of the ladder.
Is the Wound Missing Tissue?
If the wound hasn’t lost any tissue, it may be possible to close it primarily. Wounds are capable of healing by primary intention, which occurs when the wound edges are approximated (pulled together) and retained by sutures, staples, or glue. The dynamics of healing begin, and new tissue is synthesized. A healing ridge (an induration beneath the skin, extending to approximately 1 cm) forms directly under the suture line between 5 and 9 days after surgery. All forms of wound healing lead to scar, and primary wound closure is no different. If the scar is under tension, it is prone to exaggerated scar formation, such as hypertrophic scar.
What Kind of Tissue, If Any, Is Missing?
Wounds that only lack portions of skin may be allowed to granulate closed if they’re small, or skin may be grafted to speed the healing process. Wounds that have lost tendon, muscle, or bone may require transplantation of this tissue to provide form and function. Such operations require flaps of skin, muscle, fascia, or bone. Such flaps are named for their composition, such as an osteocutaneous flap, which is a bone and skin flap.
Flaps (as opposed to grafts) bring their blood supply with them and either are locally transported to the wound or are from a distant site (free flap). The free flap employs the surgical technique of freely removing tissue from one area, detaching the nutrient artery and vein from their supply vessels, and moving the tissue to the recipient site where these vessels are reattached to new supply vessels. For example, a free radial forearm flap contains radius bone, overlying muscle, and skin. It is commonly used to reconstruct the face and jaw after wide excision of cancer of the mandible and floor of the mouth.
What Donor Site Morbidity May Occur?
Donor sites have some form of scarring and may exhibit some loss of function, depending on the tissue removed. Split skin graft donor sites should heal with minimal effort; there is no loss of function but a scar remains. When the breast is reconstructed using the latissimus dorsi muscle from the back, the woman may lose some functions of the shoulder. Although some patients perceive the loss of function as tolerable, other patients—for example, a tennis player—may undoubtedly perceive it differently. If a thumb is lost, a patient may opt to transplant the great toe to provide opposition for hand function; however, most people wouldn’t want to sacrifice a thumb to replace the great toe. Some cultures (e.g., Japan) place great importance on the toes and prefer to use the second toe rather than the great toe for thumb reconstruction. In other words, the degree of loss a patient is willing to experience is proportional to his or her need for the sacrificed tissue.
What’s the Simplest Method to Achieve Wound Closure?
The easiest method available to close the wound is often used first. Wounds that can heal quickly on their own via granulation and epithelialization are allowed to do so. However, when large wounds or wounds over thin skin (e.g., sacrum) are allowed to granulate closed, the resultant scar is often unstable and prone to injury and ulceration. Skin grafting is the next simplest method and is used to treat wounds that are missing only skin. Skin grafting can be full or partial thickness, depending on the kinds of tissue missing in the recipient site and the condition of the site. Grafting of any tissue type relies on that tissue to revascularize at its recipient site. Wounds that could close on their own, but with accompanying contracture and loss of function, may also be grafted. If muscle is missing, muscle flaps may be used to fill the wound defect or cavity, but the muscle isn’t typically made functional (i.e., an insertion, origin, and nerve aren’t restored to create a functional muscle). One notable exception is the gracilis free flap to restore the function of the zygomaticus major after facial nerve injury. The blood supply to the muscle is restored so that it remains viable. The ample blood flow into the muscle is commonly used to treat complex wound problems such as osteomyelitis. Restored blood flow may also transport antibiotics and immune cells to the wound.
Muscle has been shown to supply overlying islands of skin through a series of vessels that perforate the muscle body. Surgeons can simultaneously transplant a muscle and the island of skin to both fill a wound cavity and provide skin coverage. Such a flap is called a musculocutaneous flap. These flaps are typically named after the muscle, as in the case of the tensor fascia lata flap, which is used to close a trochanteric pressure ulcer. If a large amount of skin is missing, the muscle may be transplanted and then covered with skin grafting to achieve the same effect. Such an operation is called a muscle flap and split-thickness skin graft, with the specific muscle being grafted added to the name.
Muscle is brought to the recipient site in one of two ways:
- It’s rotated along the arc of its original blood supply left intact.
- It’s freed from its blood supply and the artery and vein are reattached via a microscope at the recipient site.
Freeing the muscle, skin, and other parts of a flap allows the flap to be used for reconstruction in areas that the muscle normally couldn’t reach, such as the lower third of the leg. It’s important to note that, as often as possible, tissue should be replaced with similar tissue. Similar hair bearing, appearance, and thickness improve aesthetic appearance on the reconstructed wound.
Wounds Without Missing Tissue
Some wounds don’t require grafts because they aren’t missing tissue, or local tissue can be undermined and lifted to close the original wound.
Simple Lacerations
Traumatic wounds are often missing little or no tissue and can be closed primarily; however, the full extent of the injury must be known before any closure is attempted. Laceration of arteries and veins is usually obvious by the amount of bleeding present. Facial lacerations are especially bloody due to the robust blood supply in the face. The patient with a facial laceration is assessed for function of motor and sensory nerves, muscle, and parotid and other salivary glands in the area prior to injection with lidocaine, which would obscure the findings. Repair of vessels, tendons, ligaments, and nerves is commonly completed in the operating room because it is a sterile environment and sometimes has the added benefit of an operating microscope. Wounds are irrigated copiously to remove any debris. Skin closure is accomplished by undermining surrounding tissue to facilitate its movement and suturing layers of tissue with minimal tension. Drains may be placed in wounds with contamination or large amounts of dead space. The appearance of the wound should ideally mimic the ipsilateral appearance. However, traumatic amputation or extensive debridement may leave an appearance that’s less than acceptable.
Removing all forms of tension on the wound reduces the scar. Wounds that must be mobilized to gain function, such as incisions over joints, heal with wider scars, and this may be disturbing to the patient’s self-image. Stented dressings, immobility (e.g., limited chewing or talking with facial lacerations), and thin applications of topical antibiotics may help to minimize scars. Moist wound healing techniques, used throughout the healing process, will minimize healing time and potentially the amount of scarring. However, it’s important for the patient, the patient’s family, and members of the healthcare team to realize that scarring is inevitable and only after the scar has matured, which can take more than 1 year, will scar revision be attempted. Silicone-based dressings may be used over some healed wounds to help minimize scar buildup during the maturation phase. This has only been shown helpful with hypertrophic scarring. The reader is referred to an excellent evidence-based review of emergency wound management.2
Extensive Lacerations
Extensive lacerations, while unsightly, are seldom life threatening. Lifesaving care of the heart, lungs, and brain precedes definitive wound care. Initial wound care includes debridement of obvious dirt, glass, grass, or other foreign bodies. Massive lacerations are packed with moist dressings to prevent tissue desiccation, and, when the patient is stable, the wounds are debrided and surgically closed, if possible. Extensive wounds may require multiple debridements until viable tissue is present; these wounds may also require more complex forms of delayed closure, such as flaps.
Wounds that are not closed within the first 6 hours after injury are considered contaminated and cannot be closed primarily after that time. Some clean facial wounds are an exception to this rule, and their closure may be delayed longer in healthy patients who are on antibiotics.
Penetrating Abdominal Wounds
Penetrating abdominal wounds include stab wounds, impalements, gun shots, and so forth. These are serious wounds due to direct tissue injury, risk of contamination and sepsis, and the potential for excessive bleeding. Depending on the degree of contamination from environmental agents (e.g., dirt) or penetration of the bowel or bladder, the wound may not be closed completely. Frequently in traumatic injuries, these wounds are not closed external to the fascia. If the fascia cannot be closed, leaving the abdomen open is also a challenge. These patients require multiple re-explorations while simultaneously reducing or controlling abdominal fluid secretion and preserving the fascia for closure. Currently, no protocols exist for the management of the open abdomen, and care is based on clinical judgment.
Abdominal Compartment Syndrome
Abdominal compartment syndrome (ACS) is similar to compartment syndrome of the extremity. ACS can occur during elective abdominal operations, following abdominal trauma or pelvic fracture, and with pancreatitis. Normal intra-abdominal pressure in surgical patients is 2 to 10 mm Hg; a value above 12 mm Hg indicates intra-abdominal hypertension, and a value above 20 mm Hg is considered an indicator of abdominal compartment syndrome. Intra-abdominal pressure can be determined using simple water column manometry with a bladder catheter. When pressure is mildly increased to 10 to 15 mm Hg, the cardiac index rises due to compression of the vena cava. With further elevations, there is progressive organ dysfunction due to intra-abdominal pressure on the abdominal organs and vena cava. Direct compression on the hollow intestine and portocaval system causes these structures to collapse. When the bowel is compressed, it becomes ischemic, allowing bacteria to thrive. Vasoactive substances such as histamine and serotonin increase endothelial permeability, further capillary leakage impairs red blood cell transport, and ischemia worsens. As pressure rises, ACS not only impairs visceral organs but also damages the cardiovascular and the pulmonary systems; it may also cause a decrease in cerebral perfusion pressure. Therefore, ACS should be recognized as a possible cause of decompensation in any critically injured patient.3,4
It is important to include ACS in a wound healing chapter because the treatment of ACS is not closure of the abdomen. If the abdomen is at all difficult to close, this procedure should be abandoned and alternative techniques applied. A good rule of thumb is as follows: when looking at the abdomen horizontally, if you can see the gut above the level of the wound, consider leaving the abdomen open and using temporary closure.
The easiest way to control the open abdomen is to use a silo-bag closure. This short-term therapy has increasingly been replaced by negative pressure wound therapy (NPWT). The use of NPWT has been shown to allow successful fascial closure in patients who in the past would have required mesh grafting for closure. While NPWT increases the use of primary closure, it also shortens time to recovery.5,6
Abdominal Wound Dehiscence and Evisceration
Wound dehiscence is the separation of the edges of a surgical wound. The strength of a wound lies in the musculoaponeurotic layer of the abdomen. In the early postoperative period, wounds stay closed as a result of the strength of the sutures used or through normal healing processes as muscles regain their strength. However, some wounds are susceptible to dehiscence, thus requiring tissue transplantation.
Risk factors for wound dehiscence may be technical or related to patient factors. Technical factors are due to the type of closure used. Indeed, wound dehiscence may occur because sutures break, sutures stretch or cut through the tissue, knots slip, the suture is too thin, or an insufficient number of sutures are used. Closure is best achieved when long-lasting, absorbable, or permanent sutures are used, with secure knots that do not slip or invite bacteria to harbor in them. Sutures should be placed about 1 cm from the abdominal wound and 1 cm apart from each other. This closure places the suture in healthy fascia that will not be cut by suture material. In wounds that are healing securely, a healing ridge of palpable thick tissue about 0.5 cm appears along the incision. This ridge is almost always absent in wounds that rupture.
Risk factors for abdominal wound dehiscence were reported in a large retrospective study.7 The most significant patient-related factors for dehiscence were age over 50 years, male gender, emergency operation, longer operative times, postoperative coughing, hypertension, steroid use, cancers, ascites, chronic pulmonary disease, jaundice, anemia, and wound infection. A risk score was computed with the highest risk factors being age over 70 years; ascites; vascular surgery; surgery on the esophagus, stomach, or large bowel; coughing; and wound infection.7
Obesity, heavy coughing or retching, and ascites, all of which strain the wound during healing, predispose to dehiscence. However, many surgeons believe that if a wound is closed securely, these complications will not occur. Usually, the first sign of an impending problem is the sudden discharge of serosanguineous fluid from the wound, but some patients present with sudden evisceration following an episode of coughing or retching. When the edges of the wound separate and internal organs such as the gut are protruding from the wound, this is known as evisceration.
Evisceration is a frightening experience for the patient. Immediate treatment includes helping the patient to remain calm, medicating for pain, and holding the abdominal contents in the abdomen by keeping the viscera moist with a sterile moist towel. Exposed intestines should not be forced back into the abdomen. The patient should be kept NPO and prepared for immediate surgery. Lower the head of the bed so it is flat or no more than 20 degrees. Monitor the patient’s vital signs and assess for signs and symptoms of shock.8 The wound is explored urgently in surgery, devitalized tissue is excised, and the abdomen is closed with nonabsorbable interrupted suture taking secure bites into healthy tissue. Hernia formation is relatively common, reaching 30% in wounds that eviscerated and reclosed. If the wound has dehisced and the patient cannot tolerate another anesthetic, the wound can be packed with dressings, an abdominal binder used, or a vacuum-assisted closure applied to obtain secondary healing. These wounds will inevitably develop a hernia.
Wounds Requiring Tissue Transplantation for Closure
Tissue transplantation is a phrase used to describe closure techniques for a group of wounds that have missing tissue. In order to achieve closure, various tissues (skin, muscle, fascia, bone) can be grafted or flapped into the wound. These wounds can be quite complex to manage.
Burns
Surgical management of burn wounds includes escharotomy, excision of eschar, skin grafting, and scar revision. Because many burned patients must undergo multiple operations, it is beneficial to have a dedicated team for these patients to reduce some of the anxiety associated with surgery, anesthesia, and pain management. It is wise to have burned patients go directly from their inpatient room to surgery, not stopping in preoperative areas.
Escharotomy
Escharotomy is a decompressive operation to reduce compartment syndrome in the extremities, respiratory compromise, abdominal compartment syndrome, and even orbital compression. Full-thickness burned skin cannot stretch; therefore, during fluid resuscitation, the fluid that moves into the interstitial spaces places pressure on vessels and nerves. Indications for escharotomy include compartment syndrome of the extremities (pallor, pain, pulselessness, paresthesia, and paralysis), falling oximetry with respiratory difficulty, increased abdominal pressure, and changes in vision (with increased periorbital pressures). Escharotomy is completed by incising the burned tissue along the longitudinal axis of the extremities or across the chest and/or abdomen. The surgical site is left open to allow for both edema and chest wall movement with respiration. Once the capillary bed has stabilized and fluid leaves the interstitial spaces, the escharotomy incisions will approximate. The incisions are not closed, but rather are allowed to heal secondarily; therefore, they should be packed with saline-moistened gauze.
Excision of Eschar
Years ago, eschar was removed slowly with weeks of daily submersion in tanks and debridement with scissors. This process is still used for some burns, but many burns today are debrided with pressurized water knives, and some burns are completely excised and grafted early to promote rehabilitation. Burns of the hand are typically managed in this fashion in order to quickly mobilize the hand and restore function.
Skin Grafting
The most accepted way to permanently heal a full-thickness burn wound is to graft the wound. Skin grafts are portions of the patient’s skin removed from a donor site of unburned skin or healed burned skin that are moved to cover an open burn wound. They are often referred to as split-thickness skin grafts. Skin grafts are harvested in the operating room and placed on the freshly debrided burn wound. The skin graft lives off of the serum in the wound bed; it does not have a blood supply (unlike a flap). As the capillary beds in the wound bed grow into the skin graft, it becomes pink in color. This pink color is called a “take” and often expressed as a percentage (e.g., 50% take of the split-thickness skin graft).
A crucial aspect of skin graft healing is immobilization of the graft onto the wound bed. Most surgeons use fibrin glue, splint the graft in place, or suture it to the edges of the wound. Because edema in the space between the wound bed and the skin graft can separate the graft from capillary ingrowth, NPWT is often used to promote attachment. If NPWT is used, the suction should be continuous and not interrupted.
The dressings are usually removed at 72 hours to inspect the graft. Dressings after that point vary, but many surgeons continue to dress the newly grafted site with an antimicrobial dressing.
Skin grafts fail for several reasons. The primary reason is edema in the wound bed that lifts the grafted skin off the bed. It is imperative that all precautions to keep the grafted area elevated be followed. Too many well-meaning patients have convinced nurses that during a quick trip to the bathroom, rather than the bedside commode, the leg will remain elevated. Unfortunately, those short periods of time with the leg down may be all that is required to allow edema to lift the graft off of the wound bed!
 Patient Teaching
Patient Teaching
Instruct patients to use the commode rather than the bathroom after a skin graft to the leg.
Skin grafts can also fail due to infection in the wound. If infection is suspected, it should be ruled out with quantitative cultures of the wound bed prior to grafting.
Pruritus is a common and distressing problem in healed burn wounds. Skin grafts do not carry sweat or oil glands with them, making the transplanted skin prone to dryness and pruritus from heat retention. In addition, burn scars are not elastic, making them prone to injury. Persistent pruritus is estimated to occur in about 87% of burned patients.9 Methods to treat pruritus have not been compared systematically, and the use of histamine receptor agonists is commonly based on the belief that pruritus is mediated by mast cells. Newer thoughts on the etiology of pruritus following skin grafting are that it is a variant of pain, and newer treatments for pruritus have examined eutectic mixture of local anesthetic (EMLA) cream, transcutaneous electrical nerve stimulation (TENS), colloidal oatmeal, massage, and sedatives. The problem of pruritus is in great need of ongoing study.
Scar Revision
Scars continue to mature over 6 to 12 months following a burn. Burned areas that were allowed to heal without grafting have the most robust scars. When the scars reach across joints, the joints can be pulled into contracture. Z-plasty is a procedure that can be performed if there is adequate tissue in one dimension and not the other, for example, adequate tissue in length but not width. Z-plasty transfers the excess tissue to the area in need of tissue, thereby releasing the contracture. Many times, however, there is not enough tissue in either direction, and so skin grafting is needed.
Nonhealing Surgical Wounds
Surgical wounds can be slow to heal because of underlying disease states, such as infection, poorly controlled diabetes, impaired arterial blood flow, protein–calorie malnutrition, and compromised immunity. By convention, any surgical wound of 3 to 4 weeks’ duration that is not responding to conventional therapy is considered nonhealing. From the surgical perspective, only debridement can be offered as treatment.
Infection, including the development of biofilms, is a common culprit of nonhealing. Biofilms promote inflammation, and inflammation delays healing. Common bacterial causes include Staphylococcus, Pseudomonas, and Enterobacter. Debridement, performed either traditionally or using low-frequency ultrasound, destroys the biofilm and is an important component of wound care.10
Median Sternotomy Wounds
Median sternotomy incisions are extremely complex wounds to close following surgery. Bone stabilization is usually done by rigid fixation and immobilization, but the sternum is often closed with wire and subjected to constant movement with respiration.
Infected medial sternotomy wounds following cardiac surgery are a dreaded complication. High-risk patients include those who are obese (body mass index over 30) and those with diabetes, heart failure, previous myocardial infarction, urgent operative status, hypertension, and/or have large breasts. Perfusion time over 200 minutes, use of an intra-aortic balloon pump, and three or more distal anastomoses are risk factors for very serious infections, but these conditions rarely occur.11,12 Control of blood glucose and improvement of heart failure prior to surgery are helpful interventions.
Early wound infection, such as the aforementioned suppurative mediastinitis, appears as cellulitis, purulent wound drainage, and obvious tracking between the skin, sternum, and mediastinum. Left untreated, these infections smolder down into the mediastinum and may even extend into aortic suture lines, prosthetic grafts, and intracardiac prostheses. Local wound care is based on the condition of the wound and the condition of the patient. Wound bed preparation may include packing, debridement, or the use of NPWT, which may be used as a first line of treatment to drain the superficial infection down to the sternum because it splints the chest wall. NPWT can be used as a bridge to allow the patient to recover or stabilize. A systematic review with meta-analysis found that the use of NPWT was associated with reduced length of stay and NPWT may be more effective than standard therapy to manage surgical site infections.13,14
Caution is required when treating deep wounds that are packed. One continuous piece of rolled gauze is the preferred method for packing to avoid losing single dressings in the chest cavity. If foam is used for packing, write the number of pieces of foam used on the outermost dressing so that they can be removed with future dressing changes. Further, if wounds require topical application of solutions, the large amount of open tissue will quickly absorb the fluids. Use of such products as povidone–iodine solution in these large wounds has resulted in iodine toxicity due to the large absorptive surface. Wounds that extend to or around the myocardium should be gently packed between heartbeats. Packing the wound tightly can constrict myocardial filling during relaxation; therefore, the wound must be tucked loosely with gauze.
Chest Wall Reconstruction
Reconstruction of the chest wall can range from skin closure to chest wall stabilization. Defects following excision of a tumor, tissue loss from infection of the pleural space, and dehiscence of sternal wounds after coronary bypass grafting are examples of chest wall wounds that usually require reconstruction. Failure to stabilize the chest wall can lead to paradoxical chest motion with breathing, which results in compromised respiratory function. Prior to surgery, the patient’s cardiac and pulmonary function, nutritional status, and wound bed should be maximized.
When a defect is limited to skin and subcutaneous tissue, local skin flaps can frequently be used to close the wound. A skin flap can be rotated or advanced to cover the wound. The deltopectoral skin flap can also be used to cover chest wounds, although its blood supply is stretched to do so. The principal blood supply to the flap is from two large perforating arteries arising from the second or third intercostal space lateral to the sternal border. Therefore, any tension of the flap or chest can interfere with blood supply to the flap. The weight and torsion of the breast tissue or an obese chest can place tension on the flap, so a loose-fitting bra or binder should be used to support the tissue.
Loss of the sternum is especially complex because without the sternum, ribs are pulled inward with inspiration (e.g., flail chest). Patients can usually tolerate the loss of four ribs if the wound is closed with a muscle flap, such as the latissimus dorsi flap. Massive chest injuries or defects will require bony reconstruction; if bone is not used, acrylics or synthetic mesh can be used. However, the risks of infection and rejection are ever present when synthetic materials are used.15
 Practice Point
Practice Point
Immediately report to the surgeon any signs of flap ischemia, such as pale, dusky, mottled, or cool tissue.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


