Antiinflammatory Drugs
Objectives
• Explain the pathophysiologic basis of five cardinal signs of inflammation.
• Compare the action of various nonsteroidal antiinflammatory drugs (NSAIDs).
• Explain the use of disease-modifying antirheumatic drugs (DMARDs).
• Differentiate between the side effects and adverse reactions of NSAIDs and DMARDs.
• Apply the nursing process to the patient taking DMARDs.
Key Terms
cyclooxygenase, p. 337
COX-2 inhibitors, p. 340
disease-modifying antirheumatic drugs, p. 345
gout, p. 348
immunomodulators, p. 345
immunosuppressives, p. 345
infection, p. 337
inflammation, p. 337
nonsteroidal antiinflammatory drugs, p. 337
prostaglandins, p. 337
uricosurics, p. 348
 http://evolve.elsevier.com/KeeHayes/pharmacology/
http://evolve.elsevier.com/KeeHayes/pharmacology/
Inflammation is a response to tissue injury and infection. When the inflammatory process occurs, a vascular reaction takes place in which fluid, elements of blood, leukocytes (white blood cells [WBCs]), and chemical mediators accumulate at the injured tissue or infection site. The process of inflammation is a protective mechanism in which the body attempts to neutralize and destroy harmful agents at the site of injury and to establish conditions for tissue repair.
Although there is a relationship between inflammation and infection, these terms should not be used interchangeably. Infection is caused by microorganisms and results in inflammation, but not all inflammations are caused by infections.
Pathophysiology
The five characteristics of inflammation, called the cardinal signs of inflammation, are redness, swelling (edema), heat, pain, and loss of function. Table 25-1 gives the description and explanation of the cardinal signs of inflammation. The two phases of inflammation are the vascular phase, which occurs 10 to 15 minutes after an injury, and the delayed phase. The vascular phase is associated with vasodilation and increased capillary permeability, during which blood substances and fluid leave the plasma and go to the injured site. The delayed phase occurs when leukocytes infiltrate the inflamed tissue.
TABLE 25-1
CARDINAL SIGNS OF INFLAMMATION
| SIGNS | DESCRIPTION AND EXPLANATION |
| Erythema (redness) | Redness occurs in the first phase of inflammation. Blood accumulates in the area of tissue injury because of the release of the body’s chemical mediators (kinins, prostaglandins, and histamine). Histamine dilates the arterioles. |
| Edema (swelling) | Swelling is the second phase of inflammation. Plasma leaks into the interstitial tissue at the injury site. Kinins dilate the arterioles, increasing capillary permeability. |
| Heat | Heat at the inflammatory site can be caused by increased blood accumulation and may result from pyrogens (substances that produce fever) that interfere with the temperature-regulating center in the hypothalamus. |
| Pain | Pain is caused by tissue swelling and the release of chemical mediators. |
| Loss of function | Function is lost because of the accumulation of fluid at the tissue injury site and because of pain, which decreases mobility at the affected area. |
Various chemical mediators are released during the inflammation process. Prostaglandins that have been isolated from the exudate at inflammatory sites are among them. Prostaglandins (chemical mediators) have many effects: vasodilation, relaxation of smooth muscle, increased capillary permeability, and sensitization of nerve cells to pain.
Cyclooxygenase (COX) is the enzyme responsible for converting arachidonic acid into prostaglandins and their products. This synthesis of prostaglandins causes inflammation and pain at a tissue injury site. There are two enzyme forms of cyclooxygenase: COX-1 and COX-2. COX-1 protects the stomach lining and regulates blood platelets, and COX-2 triggers inflammation and pain.
Antiinflammatory Agents
Drugs such as aspirin inhibit the biosynthesis of prostaglandin and are therefore called prostaglandin inhibitors. Because prostaglandin inhibitors affect the inflammatory process, they are more commonly called antiinflammatory agents.
Antiinflammatory agents also relieve pain (analgesic), reduce elevated body temperature (antipyretic), and inhibit platelet aggregation (anticoagulant). Aspirin is the oldest antiinflammatory drug, but it was first used for its analgesic and antipyretic properties. As a result of searching for a more effective drug with fewer side effects, many other antiinflammatory agents, or prostaglandin inhibitors, have been discovered. Although these drugs have potent antiinflammatory effects that mimic the effects of corticosteroids (cortisone), they are not chemically related to corticosteroids and therefore are called nonsteroidal antiinflammatory drugs (NSAIDs). Most NSAIDs are used to decrease inflammation and pain for patients who have some type of arthritic condition.
Nonsteroidal Antiinflammatory Drugs
NSAIDs are aspirin and aspirin-like drugs that inhibit the enzyme COX, which is needed for the biosynthesis of prostaglandins. Chapters 26 and 45 present expanded discussions of NSAIDs in their roles as analgesics and anticoagulants, respectively. These drugs may be called prostaglandin inhibitors with varying degrees of analgesic and antipyretic effects, but they are used primarily as antiinflammatory agents to relieve inflammation and pain. Their antipyretic effect is less than their antiinflammatory effect. With several exceptions, NSAID preparations are not suggested for use in alleviating mild headaches and mildly elevated temperature. Preferred drugs for headaches and fever are aspirin, acetaminophen, and ibuprofen (given to children and adults with high fever). NSAIDs are more appropriate for reducing swelling, pain, and stiffness in joints.
NSAIDs cost more than aspirin. Other than aspirin, the only NSAIDs that can be purchased over-the-counter (OTC) are ibuprofen (Motrin, Advil) and naproxen (Aleve). Ibuprofen is also available in generic form in 200-mg tablets or capsules. All other NSAIDs require a prescription. Examples of prescription products on the market that contain NSAID contents alone or in combination include Anaprox, Celebrex, Clinoril, Daypro, Equagesic, Naprosyn, Percodan, Relafen, Soma Compound, Talwin, and Toradol. If a patient can take aspirin for the inflammatory process without gastrointestinal (GI) upset, salicylate products are usually recommended.
There are seven groups of NSAIDs:
The first six NSAID groups on the list are known as first-generation NSAIDs, and the COX-2 inhibitors are called second-generation NSAIDs.
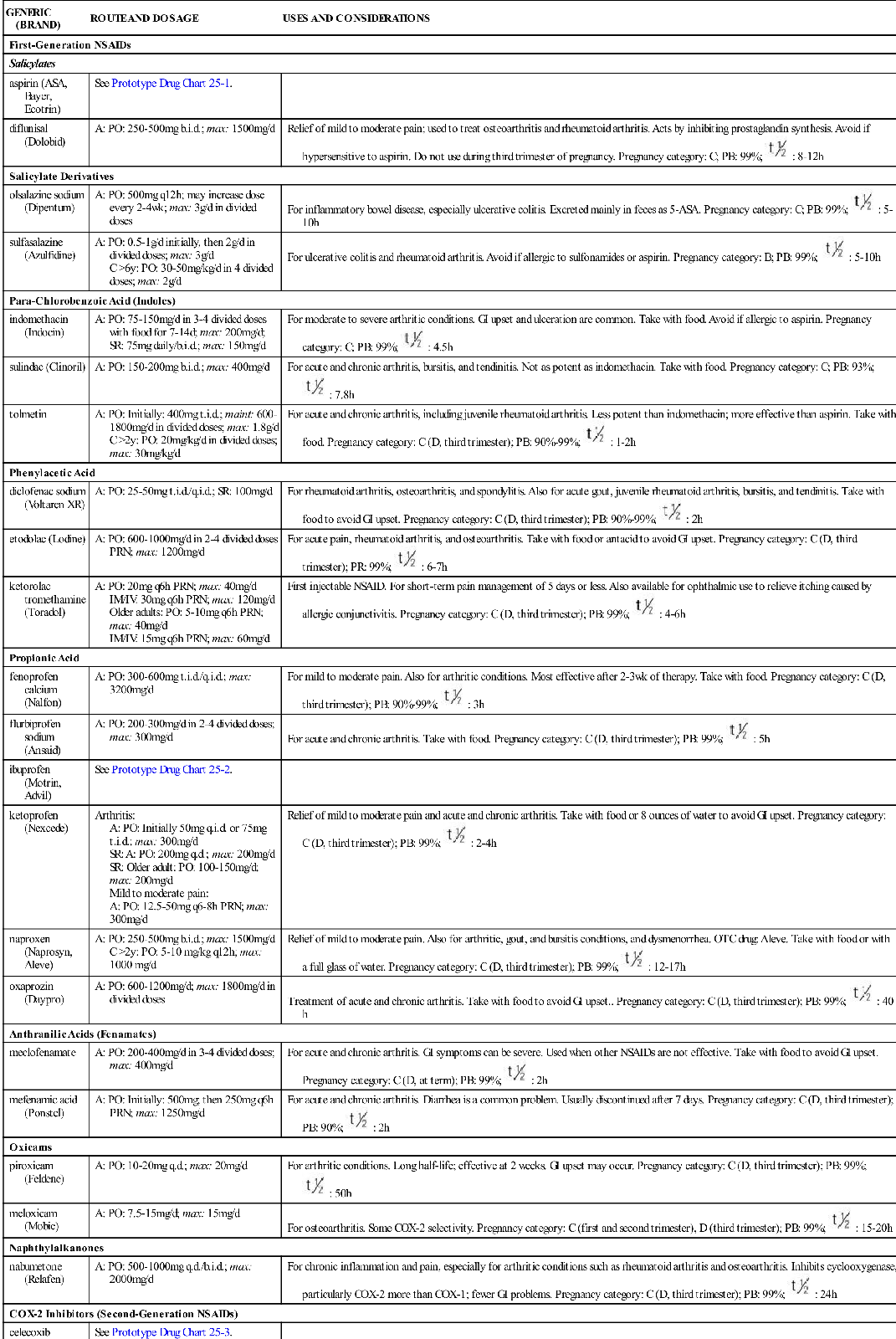
Table 25-2 provides dosage information and considerations for use for the most commonly used NSAIDs. The half-lives of NSAIDs differ greatly—some have a short half-life, and others have a moderate to long half-life with a general range of 8 to 24 hours. Aspirin should not be taken with an NSAID because of the side effects. In addition, combined therapy does not increase effectiveness.
TABLE 25-2
ANTIINFLAMMATORY AGENTS: NONSTEROIDAL
| GENERIC (BRAND) | ROUTE AND DOSAGE | USES AND CONSIDERATIONS |
| First-Generation NSAIDs | ||
| Salicylates | ||
| aspirin (ASA, Bayer, Ecotrin) | See Prototype Drug Chart 25-1. | |
| diflunisal (Dolobid) | A: PO: 250-500 mg b.i.d.; max: 1500 mg/d | Relief of mild to moderate pain; used to treat osteoarthritis and rheumatoid arthritis. Acts by inhibiting prostaglandin synthesis. Avoid if hypersensitive to aspirin. Do not use during third trimester of pregnancy. Pregnancy category: C; PB: 99%;  : 8-12 h : 8-12 h |
| Salicylate Derivatives | ||
| olsalazine sodium (Dipentum) | A: PO: 500 mg q12h; may increase dose every 2-4 wk; max: 3 g/d in divided doses | For inflammatory bowel disease, especially ulcerative colitis. Excreted mainly in feces as 5-ASA. Pregnancy category: C; PB: 99%;  : 5-10 h : 5-10 h |
| sulfasalazine (Azulfidine) | A: PO: 0.5-1 g/d initially, then 2 g/d in divided doses; max: 3 g/d C >6 y: PO: 30-50 mg/kg/d in 4 divided doses; max: 2 g/d | For ulcerative colitis and rheumatoid arthritis. Avoid if allergic to sulfonamides or aspirin. Pregnancy category: B; PB: 99%;  : 5-10 h : 5-10 h |
| Para-Chlorobenzoic Acid (Indoles) | ||
| indomethacin (Indocin) | A: PO: 75-150 mg/d in 3-4 divided doses with food for 7-14 d; max: 200 mg/d; SR: 75 mg daily/b.i.d.; max: 150 mg/d | For moderate to severe arthritic conditions. GI upset and ulceration are common. Take with food. Avoid if allergic to aspirin. Pregnancy category: C; PB: 99%;  : 4.5 h : 4.5 h |
| sulindac (Clinoril) | A: PO: 150-200 mg b.i.d.; max: 400 mg/d | For acute and chronic arthritis, bursitis, and tendinitis. Not as potent as indomethacin. Take with food. Pregnancy category: C; PB: 93%;  : 7.8 h : 7.8 h |
| tolmetin | A: PO: Initially: 400 mg t.i.d.; maint: 600-1800 mg/d in divided doses; max: 1.8 g/d C >2 y: PO: 20 mg/kg/d in divided doses; max: 30 mg/kg/d | For acute and chronic arthritis, including juvenile rheumatoid arthritis. Less potent than indomethacin; more effective than aspirin. Take with food. Pregnancy category: C (D, third trimester); PB: 90%-99%;  : 1-2 h : 1-2 h |
| Phenylacetic Acid | ||
| diclofenac sodium (Voltaren XR) | A: PO: 25-50 mg t.i.d./q.i.d.; SR: 100 mg/d | For rheumatoid arthritis, osteoarthritis, and spondylitis. Also for acute gout, juvenile rheumatoid arthritis, bursitis, and tendinitis. Take with food to avoid GI upset. Pregnancy category: C (D, third trimester); PB: 90%-99%;  : 2 h : 2 h |
| etodolac (Lodine) | A: PO: 600-1000 mg/d in 2-4 divided doses PRN; max: 1200 mg/d | For acute pain, rheumatoid arthritis, and osteoarthritis. Take with food or antacid to avoid GI upset. Pregnancy category: C (D, third trimester); PR: 99%;  : 6-7 h : 6-7 h |
| ketorolac tromethamine (Toradol) | A: PO: 20 mg q6h PRN; max: 40 mg/d IM/IV: 30 mg q6h PRN; max: 120 mg/d Older adults: PO: 5-10 mg q6h PRN; max: 40 mg/d IM/IV: 15 mg q6h PRN; max: 60 mg/d | First injectable NSAID. For short-term pain management of 5 days or less. Also available for ophthalmic use to relieve itching caused by allergic conjunctivitis. Pregnancy category: C (D, third trimester); PB: 99%;  : 4-6 h : 4-6 h |
| Propionic Acid | ||
| fenoprofen calcium (Nalfon) | A: PO: 300-600 mg t.i.d./q.i.d.; max: 3200 mg/d | For mild to moderate pain. Also for arthritic conditions. Most effective after 2-3 wk of therapy. Take with food. Pregnancy category: C (D, third trimester); PB: 90%-99%;  : 3 h : 3 h |
| flurbiprofen sodium (Ansaid) | A: PO: 200-300 mg/d in 2-4 divided doses; max: 300 mg/d | For acute and chronic arthritis. Take with food. Pregnancy category: C (D, third trimester); PB: 99%;  : 5 h : 5 h |
| ibuprofen (Motrin, Advil) | See Prototype Drug Chart 25-2. | |
| ketoprofen (Nexcede) | Arthritis: A: PO: Initially 50 mg q.i.d. or 75 mg t.i.d.; max: 300 mg/d SR: A: PO: 200 mg q.d.; max: 200 mg/d SR: Older adult: PO: 100-150 mg/d; max: 200 mg/d Mild to moderate pain: A: PO: 12.5-50 mg q6-8h PRN; max: 300 mg/d | Relief of mild to moderate pain and acute and chronic arthritis. Take with food or 8 ounces of water to avoid GI upset. Pregnancy category: C (D, third trimester); PB: 99%;  : 2-4 h : 2-4 h |
| naproxen (Naprosyn, Aleve) | A: PO: 250-500 mg b.i.d.; max: 1500 mg/d C >2y: PO: 5-10 mg/kg q12h; max: 1000 mg/d | Relief of mild to moderate pain. Also for arthritic, gout, and bursitis conditions, and dysmenorrhea. OTC drug: Aleve. Take with food or with a full glass of water. Pregnancy category: C (D, third trimester); PB: 99%;  : 12-17 h : 12-17 h |
| oxaprozin (Daypro) | A: PO: 600-1200 mg/d; max: 1800 mg/d in divided doses | Treatment of acute and chronic arthritis. Take with food to avoid GI upset.. Pregnancy category: C (D, third trimester); PB: 99%;  : 40 h : 40 h |
| Anthranilic Acids (Fenamates) | ||
| meclofenamate | A: PO: 200-400 mg/d in 3-4 divided doses; max: 400 mg/d | For acute and chronic arthritis. GI symptoms can be severe. Used when other NSAIDs are not effective. Take with food to avoid GI upset. Pregnancy category: C (D, at term); PB: 99%;  : 2 h : 2 h |
| mefenamic acid (Ponstel) | A: PO: Initially: 500 mg; then 250 mg q6h PRN; max: 1250 mg/d | For acute and chronic arthritis. Diarrhea is a common problem. Usually discontinued after 7 days. Pregnancy category: C (D, third trimester); PB: 90%;  : 2 h : 2 h |
| Oxicams | ||
| piroxicam (Feldene) | A: PO: 10-20 mg q.d.; max: 20 mg/d | For arthritic conditions. Long half-life; effective at 2 weeks. GI upset may occur. Pregnancy category: C (D, third trimester); PB: 99%;  : 50 h : 50 h |
| meloxicam (Mobic) | A: PO: 7.5-15 mg/d; max: 15 mg/d | For osteoarthritis. Some COX-2 selectivity. Pregnancy category: C (first and second trimester), D (third trimester); PB: 99%;  : 15-20 h : 15-20 h |
| Naphthylalkanones | ||
| nabumetone (Relafen) | A: PO: 500-1000 mg q.d./b.i.d.; max: 2000 mg/d | For chronic inflammation and pain, especially for arthritic conditions such as rheumatoid arthritis and osteoarthritis. Inhibits cyclooxygenase, particularly COX-2 more than COX-1; fewer GI problems. Pregnancy category: C (D, third trimester); PB: 99%;  : 24 h : 24 h |
| COX-2 Inhibitors (Second-Generation NSAIDs) | ||
| celecoxib (Celebrex) | See Prototype Drug Chart 25-3. | |

 , half-life; t.i.d., three times a day; UK, unknown; wk, week; y, year; >, greater than; <, less than.
, half-life; t.i.d., three times a day; UK, unknown; wk, week; y, year; >, greater than; <, less than.Salicylates
Aspirin comes from the family of salicylates derived from salicylic acid. Aspirin is also called acetylsalicylic acid (ASA) after the acetyl group used in the composition of aspirin. The abbreviation frequently used for aspirin is ASA.
Aspirin was developed in 1899 by Adolph Bayer, making it the oldest antiinflammatory agent. It was the most frequently used antiinflammatory agent before the introduction of ibuprofen. Aspirin is a prostaglandin inhibitor that decreases the inflammatory process. It is also considered an antiplatelet drug for patients with cardiac or cerebrovascular disorders; aspirin decreases platelet aggregation, and thus blood clotting is decreased. Because high doses of aspirin are usually needed to relieve inflammation, gastric distress is a common problem. In such cases, enteric-coated (EC) tablets may be used. Aspirin should not be taken with other NSAIDs because it decreases the blood level and effectiveness of NSAIDs.
Aspirin and other NSAIDs relieve pain by inhibiting the enzyme COX, which is needed for the biosynthesis of prostaglandins. There are two enzyme forms of cyclooxygenase, symbolized as COX-1 and COX-2 (Figure 25-1). COX-1 protects the stomach lining and regulates blood platelets, promoting blood clotting. COX-2 triggers pain and inflammation at the injured site. Usually NSAIDs inhibit or block both COX-1 and COX-2. Inhibition of COX-1 produces the desirable effect of decreasing platelet aggregation, but the undesirable effect of decreasing protection to the stomach lining. Stomach bleeding and ulcers may occur with aspirin and NSAID agents. When COX-2 is inhibited, pain and fever are reduced and inflammation is suppressed, but COX-2 inhibitors do not cause gastric ulceration and have no effect on platelet function.
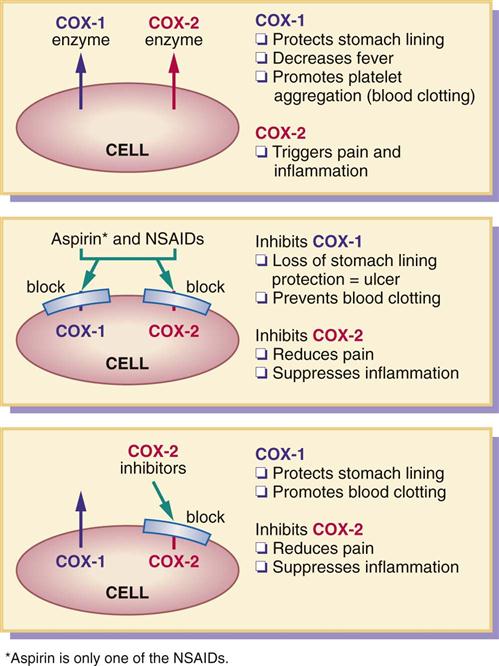
New NSAIDs, called COX-2 inhibitors, block only COX-2 and not COX-1. These drugs leave protection for the stomach lining intact (no gastric bleeding and ulcers), but still deliver relief for pain and inflammation.
A COX-2 inhibitor approved by the U.S. Food and Drug Administration (FDA) is celecoxib (Celebrex). Drugs similar to COX-2 inhibitors include meloxicam (Mobic) and nabumetone (Relafen), which allow some stomach protection. Patients at risk for stroke or heart attack who take aspirin to prevent blood clotting (decrease platelet aggregation) would not benefit from COX-2 inhibitors. If the COX-1 enzyme was not blocked, increased blood clotting would remain even though the stomach lining is protected.
Many researchers believe that COX-2 inhibitors may prevent some types of cancer (e.g., colon cancer). Fruits and vegetables block COX-2 enzyme naturally, protecting the colon from malignant growths.
Pharmacokinetics
Aspirin is well absorbed from the GI tract (Prototype Drug Chart 25-1). It can cause GI upset, so it should be taken with water, milk, or food. The EC or buffered form can decrease gastric distress. EC tablets should not be crushed or broken.
 Prototype Drug Chart 25-1
Prototype Drug Chart 25-1 Astrin
Astrin : 2-3 h (low dose); 15-20 h (high dose)
: 2-3 h (low dose); 15-20 h (high dose)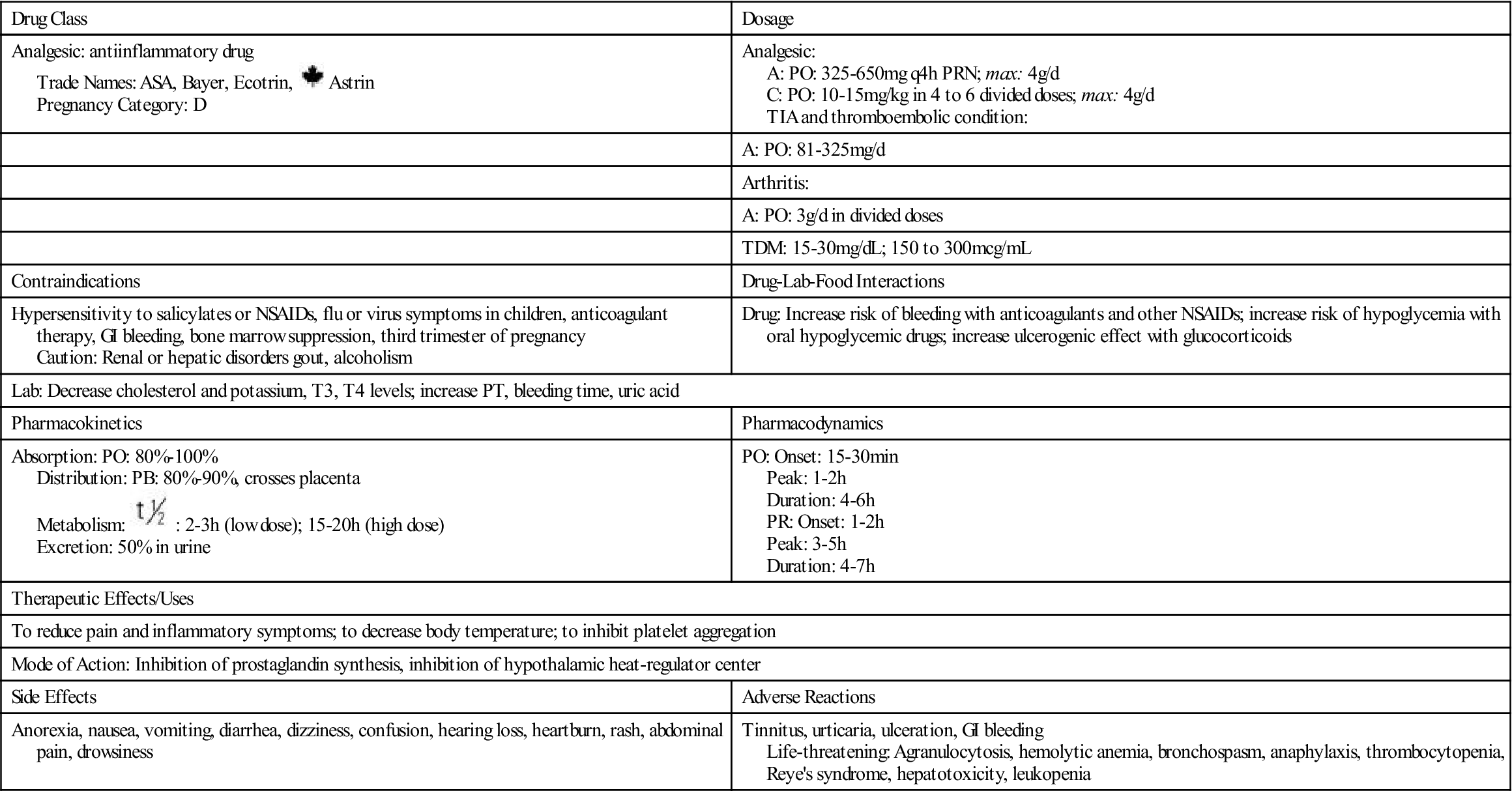
 , half-life; TDM, therapeutic drug monitoring; TIA, transient ischemic attack;
, half-life; TDM, therapeutic drug monitoring; TIA, transient ischemic attack;  , Canadian drug name.
, Canadian drug name.Aspirin has a short half-life. It should not be taken during the last trimester of pregnancy, because it could cause premature closure of the ductus arteriosus in the fetus. Aspirin should not be taken by children with flu symptoms, because it may cause the potentially fatal Reye syndrome.
Pharmacodynamics
Aspirin, like other NSAIDs, inhibits prostaglandin synthesis by inhibiting COX-1 and COX-2; thus it decreases inflammation and pain. The onset of action for aspirin is within 30 minutes. It peaks in 1 to 2 hours, and the duration of action is an average of 4 to 6 hours. The action for the rectal preparation of aspirin can be erratic because of blood supply and fecal material in the rectum; it may take a week or longer for a therapeutic antiinflammatory effect.
Hypersensitivity to Salicylate Products
Patients may be hypersensitive to aspirin. Tinnitus (ringing in the ears), vertigo (dizziness), and bronchospasm—especially in asthmatic patients—are symptoms of aspirin overdose or hypersensitivity to aspirin. Patients should not take diflunisal if they are hypersensitive to aspirin. Diflunisal is a derivative of salicylic acid, although it is not converted to salicylic acid in the body.
Salicylates are present in numerous foods (e.g., prunes, raisins, licorice) and in spices (e.g., curry powder, paprika).
 Nursing Process
Nursing Process






 Monitor serum salicylate (aspirin) level when patient takes high doses of aspirin for chronic conditions such as arthritis. Normal therapeutic range is 15 to 30 mg/dL. Mild toxicity occurs at serum level of >30 mg/dL, and severe toxicity occurs at >50 mg/dL.
Monitor serum salicylate (aspirin) level when patient takes high doses of aspirin for chronic conditions such as arthritis. Normal therapeutic range is 15 to 30 mg/dL. Mild toxicity occurs at serum level of >30 mg/dL, and severe toxicity occurs at >50 mg/dL.



