Chapter 13 Women’s Health Care Plans Breast Cancer/Surgical Management with Breast Reconstruction Option For additional care plans, go to http://evolve.elsevier.com/Gulanick/. Breast cancer is the most commonly occurring cancer in American women (except skin cancer). It is the second leading cause of cancer death in women; lung cancer remains the most fatal of all cancers for both men and women. A woman has a 1-in-8 lifetime risk for developing this highly treatable disease. Despite its common occurrence, most women with breast cancer will not succumb to the disease; the 10-year survival rate is approximately 90%, with about 2.5 million breast cancer survivors in the United States. Complete sequencing of the human genome has led to the identification of two genes associated with the development of breast cancer and ovarian cancer. Women who carry a mutation in the BRCA1 or BRCA2 gene are known to be at increased risk for the development of breast cancer, and these cancers often develop at a much younger age than usual (age 45 or younger). The lifetime breast cancer risk for women with hereditary cancer (defined as having an inherited mutation in the BRCA1 or BRCA2 gene) is 56% to 85%. Hereditary breast cancer, however, accounts for only 5% to 10% of all breast cancer cases. The remainder of all breast cancers do not have an identified hereditary component. In other words, most women who get breast cancer have a noninherited form. In these women the incidence of the disease increases with age, with most occurring in women over 50 years of age. Two other risk factors are associated with an increased risk for breast cancer: exposure to radiation (e.g., women who have received chest irradiation as prior treatment for other malignancies such as Hodgkin lymphoma) and the period of time that the body makes estrogen. The earlier a woman begins to menstruate and the later she has her first pregnancy, or after prolonged hormone replacement therapy, the higher is her risk for breast cancer. The later menopause occurs in a woman, the higher her postmenopausal risk for breast cancer. Another significant risk factor is cigarette smoking. Research suggests that some women have a slow-acting form of a liver enzyme that normally detoxifies carcinogens, permitting the carcinogens present in tobacco to remain in the body longer. With the use of breast self-examination and screening mammography, most breast cancer is successfully diagnosed at an early stage. Treatment recommendations are made according to the disease stage and may include surgery, radiation, chemotherapy, or a combination of these. Prognosis is related to the stage and type of tumor. Adjuvant chemohormonal therapy has decreased recurrence and has improved survival rates in most subgroups of patients. Even though the treatment modalities have lengthened the survival time for metastatic breast cancer, stage IV or metastatic disease is not curable. Surgical management of breast cancer includes two major approaches: (1) breast conservation therapy, often referred to as a lumpectomy, and (2) removal of the entire breast, which is called a modified radical or radical mastectomy. Both of these surgical approaches may include examination of the axillary lymph nodes for evidence of micrometastatic disease, usually through sentinel lymph node biopsy. The presence or absence of disease in the lymph nodes determines prognosis (and subsequent treatment) and is referred to as nodal status. Women with node-negative disease generally have a better prognosis than women with node-positive disease. Women undergoing mastectomy have several options for breast reconstruction, including immediate or delayed reconstruction. The timing depends on several factors, including cancer treatment protocol, other medical problems, and the woman’s preference. Breast-conserving therapy (lumpectomy) with adjuvant chemotherapy, radiation therapy, or both is considered a treatment that is medically equivalent to mastectomy. Specialized breast cancer treatment centers are available, providing a multidisciplinary treatment approach (e.g., medical and surgical oncologists, gynecologists, radiation oncologists, clinical nurse specialists, nurses, and social workers). This care plan addresses the surgical management of breast cancer. Follow-up care and adjunct treatment would be performed in the ambulatory care setting. Deficient Knowledge: Preoperative Acute Pain Risk for Situational Low Self-Esteem/Disturbed Body Image Anxiety Deficient Knowledge: Postoperative Related Care Plans Cancer chemotherapy, p. 691 Cancer radiation therapy, p. 702 Ineffective peripheral tissue perfusion, p. 197 Ineffective sexuality pattern, p. 176 Cervical Cancer Cancer of the cervix is one of the most common cancers affecting women’s reproductive organs, occurring between 35 and 55 years of age. It is more commonly seen in the African-American and Hispanic American populations. Although the number of cases and deaths have significantly declined during the past 20 years, it remains a serious health risk. Several factors increase one’s risk for cervical cancer, including human papillomavirus (HPV) infection, lack of regular Papanicolaou (Pap) smear screening, many sexual partners, early sexual activity, history of sexually transmitted infections, long-term use of birth control pills, having many children, weakened immune systems, and smoking habit. At least 95% of the cases are reported to be related to sexual exposure to HPV. A vaccine approved by the U.S. Food and Drug Administration (FDA) for HPV is recommended for girls as young as 9 to 12 years of age and for women 13 to 26 years of age. The death rate from cervical cancer has significantly dropped as a result of Pap tests. When diagnosed at an early, preinvasive stage, the survival rate is nearly 100%. According to the American Cancer Society, invasive cancer that is diagnosed while still confined to the cervix has a 5-year survival rate of around 91%. Treatment options depend on the tumor stage at diagnosis. Treatment may consist of conization, loop electrosurgical excision procedure, cryosurgery, cauterization, laser surgery, hysterectomy, radiation, chemotherapy, or biological therapy. Deficient Knowledge Risk for Ineffective Coping Related Care Plans Acute pain, p. 144 Cancer chemotherapy, p. 691 Cancer radiation therapy, p. 702 Disturbed body image, p. 29 Hysterectomy, p. 876 Ineffective sexuality pattern, p. 176 Hysterectomy Salpingectomy; Oophorectomy; Total Abdominal Hysterectomy; Cervical Cancer Hysterectomy is a surgical procedure that involves the removal of the uterus with or without removal of the cervix. The surgery may also include removal of the ovaries (oophorectomy) and the fallopian tubes (salpingectomy). Indications for the surgery include endometriosis, uterine fibroids, cancer, uterine prolapse or bleeding, and ectopic pregnancy. Although other, less-invasive treatments can be considered for most of these problems, hysterectomy might be the only option for cancer. Hysterectomy is the second most common surgical procedure in women, with approximately 600,000 hysterectomies performed each year in the United States. Hysterectomy with oophorectomy results in surgically induced menopause. The woman may experience symptoms of menopause more severely than normal menopause because of the sudden loss of hormones. Every attempt is usually undertaken to retain the reproductive function of women who are still of childbearing age; however, certain clinical situations, such as aggressive forms of cancer, may require aggressive surgery. A hysterectomy can be performed using an abdominal, vaginal, or laparoscopic approach. The surgical approach used depends on the surgeon and patient, as well as on the amount of visualization and area of manipulation required. The bulk of recovery takes place at home, with patients gaining full function within 2 weeks if the vaginal approach was used for the procedure and 4 to 6 weeks if the abdominal approach was used. Deficient Knowledge: Surgical Treatment Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Integumentary Care Plans Renal and Urinary Tract Care Plans Cardiac and Vascular Care Plans Nursing Diagnosis Care Plans Stay updated, free articles. Join our Telegram channel Join Tags: Nursing Care Plans Nursing Diagnosis and Intervention Dec 3, 2016 | Posted by admin in NURSING | Comments Off on Women’s Health Care Plans Full access? Get Clinical Tree
Chapter 13 Women’s Health Care Plans Breast Cancer/Surgical Management with Breast Reconstruction Option For additional care plans, go to http://evolve.elsevier.com/Gulanick/. Breast cancer is the most commonly occurring cancer in American women (except skin cancer). It is the second leading cause of cancer death in women; lung cancer remains the most fatal of all cancers for both men and women. A woman has a 1-in-8 lifetime risk for developing this highly treatable disease. Despite its common occurrence, most women with breast cancer will not succumb to the disease; the 10-year survival rate is approximately 90%, with about 2.5 million breast cancer survivors in the United States. Complete sequencing of the human genome has led to the identification of two genes associated with the development of breast cancer and ovarian cancer. Women who carry a mutation in the BRCA1 or BRCA2 gene are known to be at increased risk for the development of breast cancer, and these cancers often develop at a much younger age than usual (age 45 or younger). The lifetime breast cancer risk for women with hereditary cancer (defined as having an inherited mutation in the BRCA1 or BRCA2 gene) is 56% to 85%. Hereditary breast cancer, however, accounts for only 5% to 10% of all breast cancer cases. The remainder of all breast cancers do not have an identified hereditary component. In other words, most women who get breast cancer have a noninherited form. In these women the incidence of the disease increases with age, with most occurring in women over 50 years of age. Two other risk factors are associated with an increased risk for breast cancer: exposure to radiation (e.g., women who have received chest irradiation as prior treatment for other malignancies such as Hodgkin lymphoma) and the period of time that the body makes estrogen. The earlier a woman begins to menstruate and the later she has her first pregnancy, or after prolonged hormone replacement therapy, the higher is her risk for breast cancer. The later menopause occurs in a woman, the higher her postmenopausal risk for breast cancer. Another significant risk factor is cigarette smoking. Research suggests that some women have a slow-acting form of a liver enzyme that normally detoxifies carcinogens, permitting the carcinogens present in tobacco to remain in the body longer. With the use of breast self-examination and screening mammography, most breast cancer is successfully diagnosed at an early stage. Treatment recommendations are made according to the disease stage and may include surgery, radiation, chemotherapy, or a combination of these. Prognosis is related to the stage and type of tumor. Adjuvant chemohormonal therapy has decreased recurrence and has improved survival rates in most subgroups of patients. Even though the treatment modalities have lengthened the survival time for metastatic breast cancer, stage IV or metastatic disease is not curable. Surgical management of breast cancer includes two major approaches: (1) breast conservation therapy, often referred to as a lumpectomy, and (2) removal of the entire breast, which is called a modified radical or radical mastectomy. Both of these surgical approaches may include examination of the axillary lymph nodes for evidence of micrometastatic disease, usually through sentinel lymph node biopsy. The presence or absence of disease in the lymph nodes determines prognosis (and subsequent treatment) and is referred to as nodal status. Women with node-negative disease generally have a better prognosis than women with node-positive disease. Women undergoing mastectomy have several options for breast reconstruction, including immediate or delayed reconstruction. The timing depends on several factors, including cancer treatment protocol, other medical problems, and the woman’s preference. Breast-conserving therapy (lumpectomy) with adjuvant chemotherapy, radiation therapy, or both is considered a treatment that is medically equivalent to mastectomy. Specialized breast cancer treatment centers are available, providing a multidisciplinary treatment approach (e.g., medical and surgical oncologists, gynecologists, radiation oncologists, clinical nurse specialists, nurses, and social workers). This care plan addresses the surgical management of breast cancer. Follow-up care and adjunct treatment would be performed in the ambulatory care setting. Deficient Knowledge: Preoperative Acute Pain Risk for Situational Low Self-Esteem/Disturbed Body Image Anxiety Deficient Knowledge: Postoperative Related Care Plans Cancer chemotherapy, p. 691 Cancer radiation therapy, p. 702 Ineffective peripheral tissue perfusion, p. 197 Ineffective sexuality pattern, p. 176 Cervical Cancer Cancer of the cervix is one of the most common cancers affecting women’s reproductive organs, occurring between 35 and 55 years of age. It is more commonly seen in the African-American and Hispanic American populations. Although the number of cases and deaths have significantly declined during the past 20 years, it remains a serious health risk. Several factors increase one’s risk for cervical cancer, including human papillomavirus (HPV) infection, lack of regular Papanicolaou (Pap) smear screening, many sexual partners, early sexual activity, history of sexually transmitted infections, long-term use of birth control pills, having many children, weakened immune systems, and smoking habit. At least 95% of the cases are reported to be related to sexual exposure to HPV. A vaccine approved by the U.S. Food and Drug Administration (FDA) for HPV is recommended for girls as young as 9 to 12 years of age and for women 13 to 26 years of age. The death rate from cervical cancer has significantly dropped as a result of Pap tests. When diagnosed at an early, preinvasive stage, the survival rate is nearly 100%. According to the American Cancer Society, invasive cancer that is diagnosed while still confined to the cervix has a 5-year survival rate of around 91%. Treatment options depend on the tumor stage at diagnosis. Treatment may consist of conization, loop electrosurgical excision procedure, cryosurgery, cauterization, laser surgery, hysterectomy, radiation, chemotherapy, or biological therapy. Deficient Knowledge Risk for Ineffective Coping Related Care Plans Acute pain, p. 144 Cancer chemotherapy, p. 691 Cancer radiation therapy, p. 702 Disturbed body image, p. 29 Hysterectomy, p. 876 Ineffective sexuality pattern, p. 176 Hysterectomy Salpingectomy; Oophorectomy; Total Abdominal Hysterectomy; Cervical Cancer Hysterectomy is a surgical procedure that involves the removal of the uterus with or without removal of the cervix. The surgery may also include removal of the ovaries (oophorectomy) and the fallopian tubes (salpingectomy). Indications for the surgery include endometriosis, uterine fibroids, cancer, uterine prolapse or bleeding, and ectopic pregnancy. Although other, less-invasive treatments can be considered for most of these problems, hysterectomy might be the only option for cancer. Hysterectomy is the second most common surgical procedure in women, with approximately 600,000 hysterectomies performed each year in the United States. Hysterectomy with oophorectomy results in surgically induced menopause. The woman may experience symptoms of menopause more severely than normal menopause because of the sudden loss of hormones. Every attempt is usually undertaken to retain the reproductive function of women who are still of childbearing age; however, certain clinical situations, such as aggressive forms of cancer, may require aggressive surgery. A hysterectomy can be performed using an abdominal, vaginal, or laparoscopic approach. The surgical approach used depends on the surgeon and patient, as well as on the amount of visualization and area of manipulation required. The bulk of recovery takes place at home, with patients gaining full function within 2 weeks if the vaginal approach was used for the procedure and 4 to 6 weeks if the abdominal approach was used. Deficient Knowledge: Surgical Treatment Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Integumentary Care Plans Renal and Urinary Tract Care Plans Cardiac and Vascular Care Plans Nursing Diagnosis Care Plans Stay updated, free articles. Join our Telegram channel Join Tags: Nursing Care Plans Nursing Diagnosis and Intervention Dec 3, 2016 | Posted by admin in NURSING | Comments Off on Women’s Health Care Plans Full access? Get Clinical Tree
 For additional care plans, go to
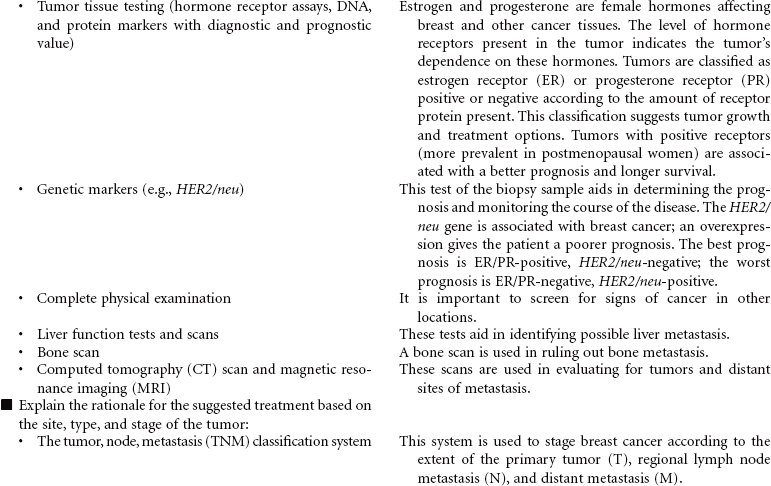
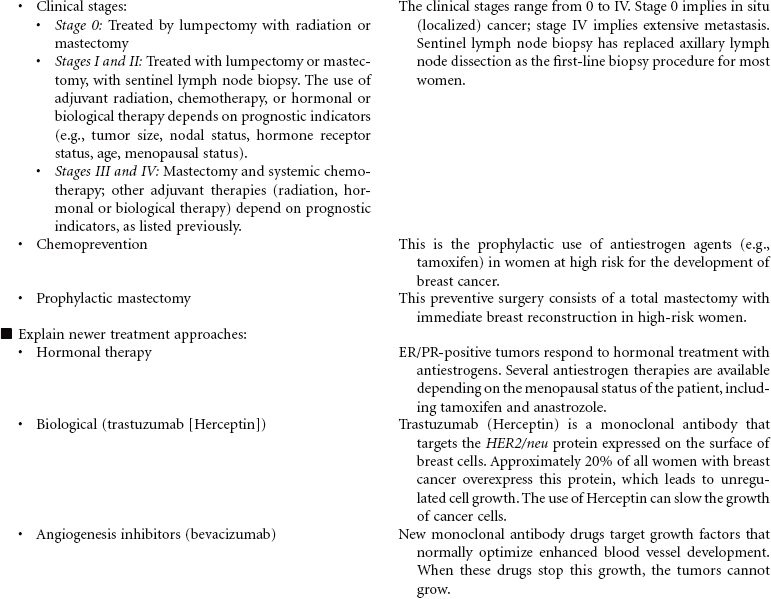
For additional care plans, go to  Deficient Knowledge: Preoperative
Deficient Knowledge: Preoperative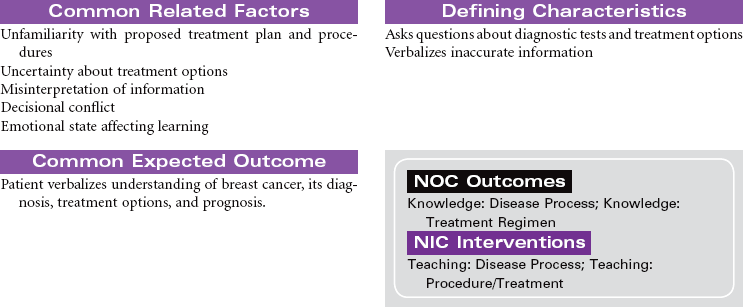

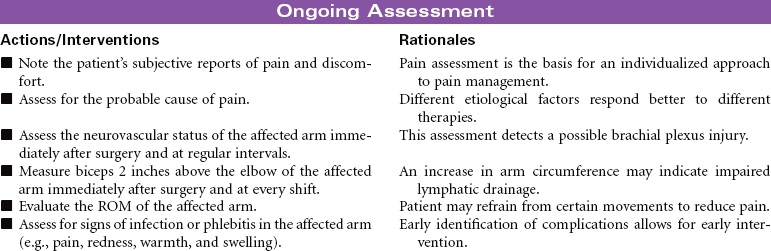
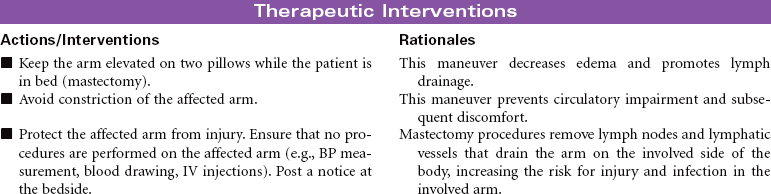
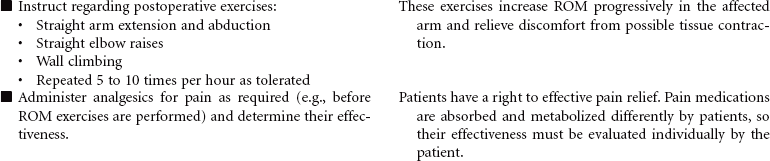
 Acute Pain
Acute Pain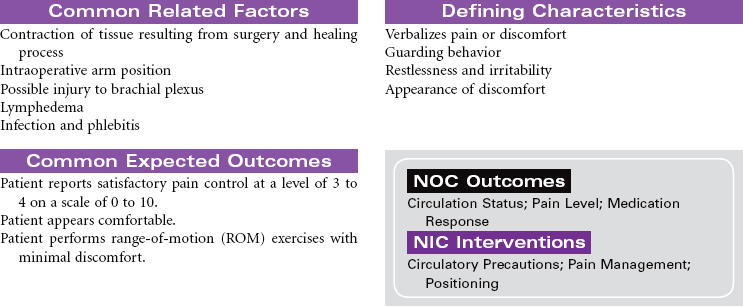
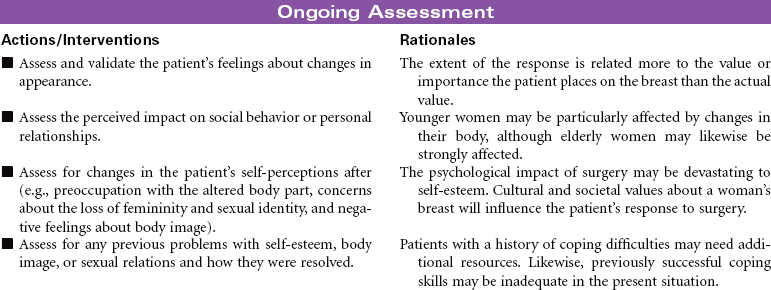
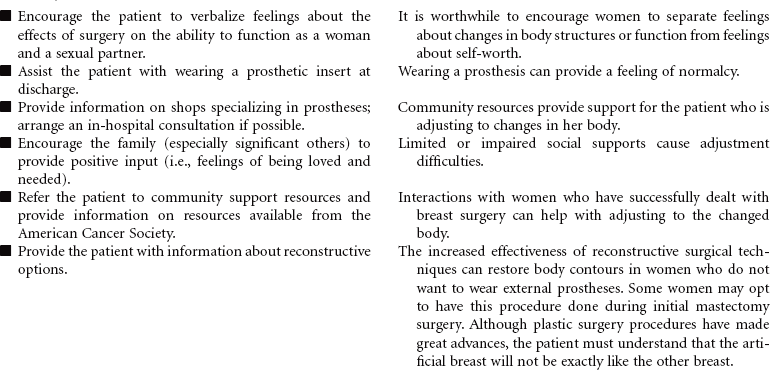
 Risk for Situational Low Self-Esteem/Disturbed Body Image
Risk for Situational Low Self-Esteem/Disturbed Body Image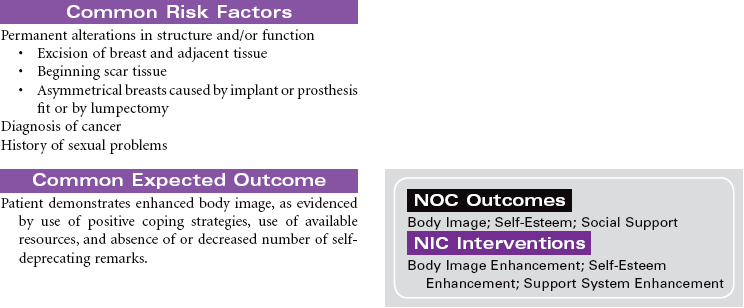

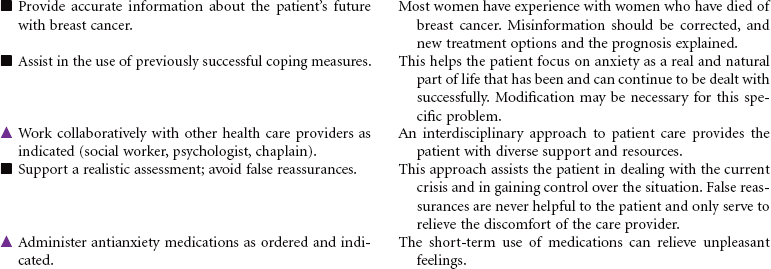
 Anxiety
Anxiety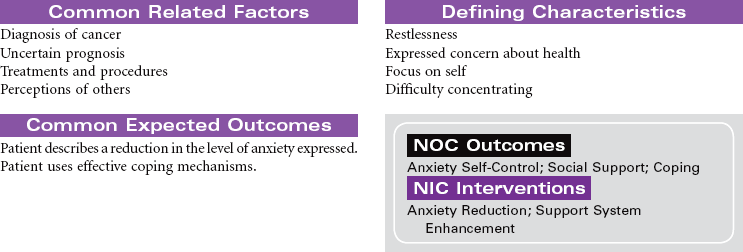


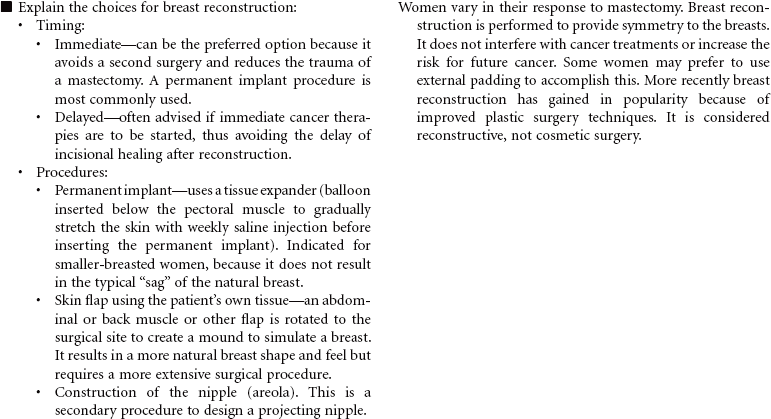
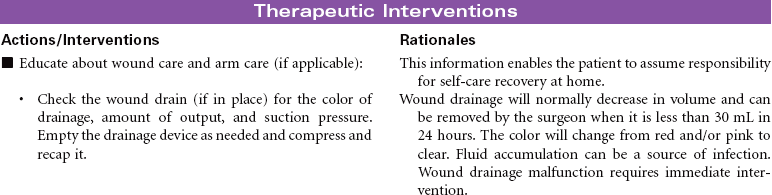
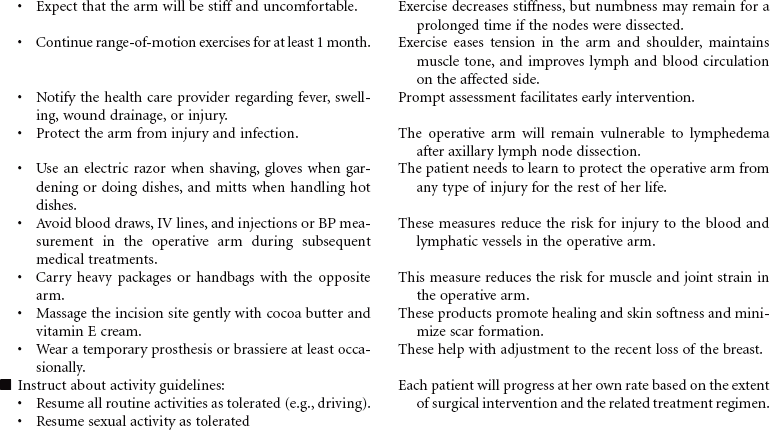
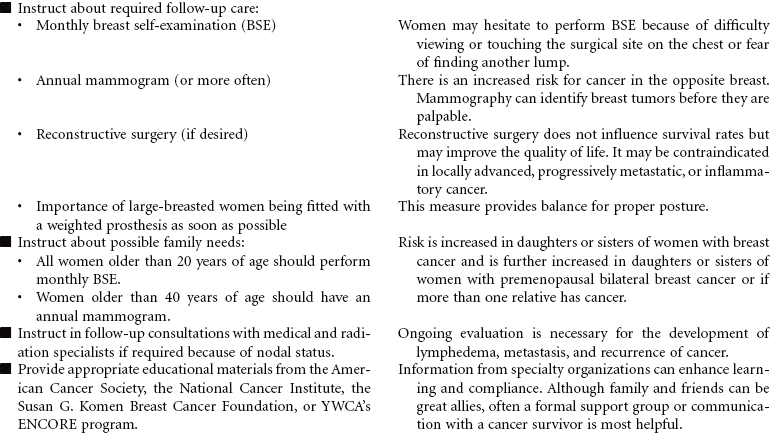
 Deficient Knowledge: Postoperative
Deficient Knowledge: Postoperative

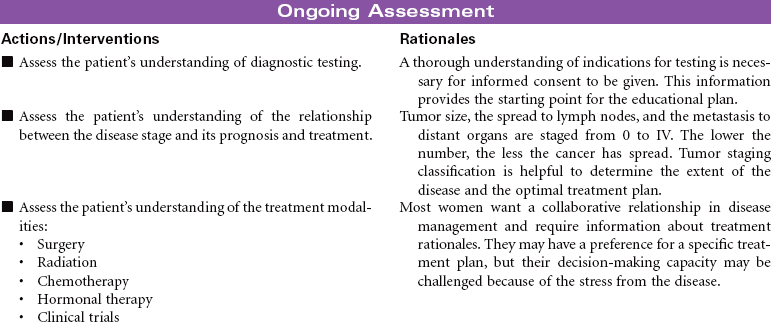
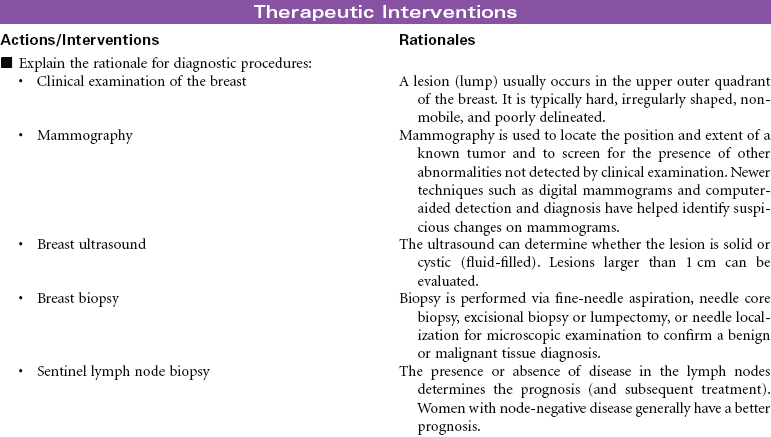
 Deficient Knowledge
Deficient Knowledge

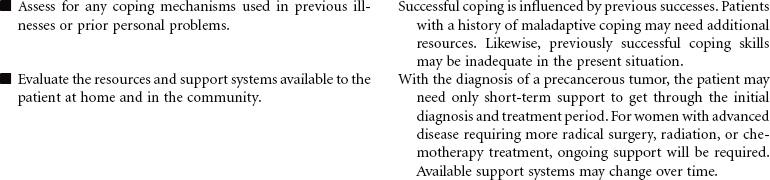
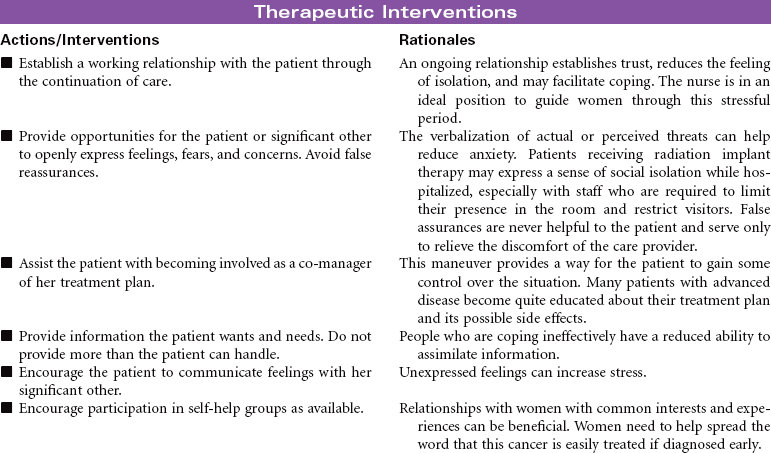
 Risk for Ineffective Coping
Risk for Ineffective Coping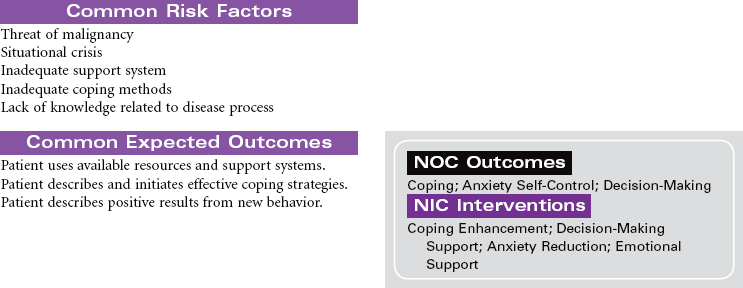

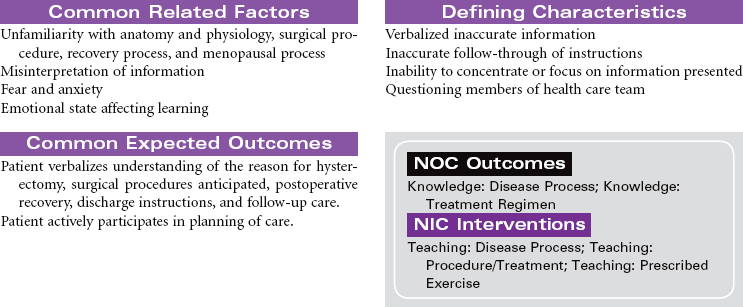
 Deficient Knowledge: Surgical Treatment
Deficient Knowledge: Surgical Treatment