Chapter 11 Acute Tubular Necrosis (ATN); Renal Insufficiency; Acute Kidney Injury Internal Arteriovenous Fistula; Graft; Central Venous Catheter; Renal Replacement Therapy
Renal and Urinary Tract Care Plans
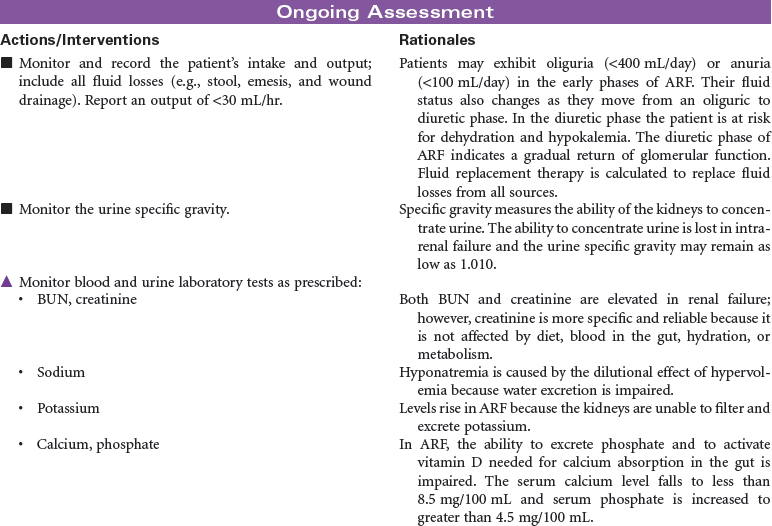
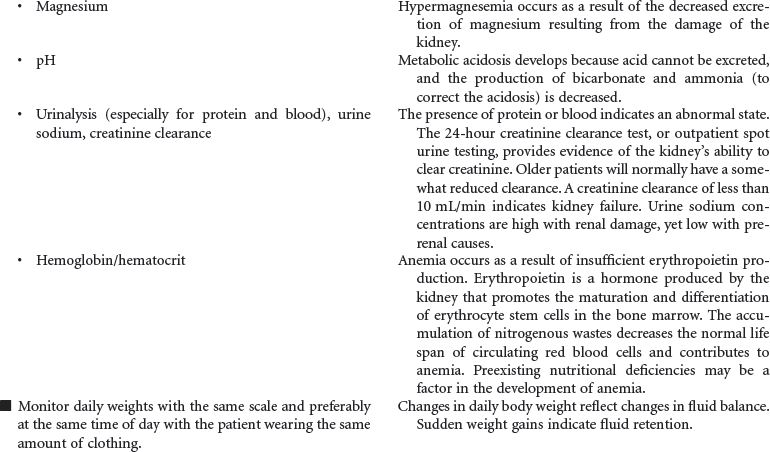
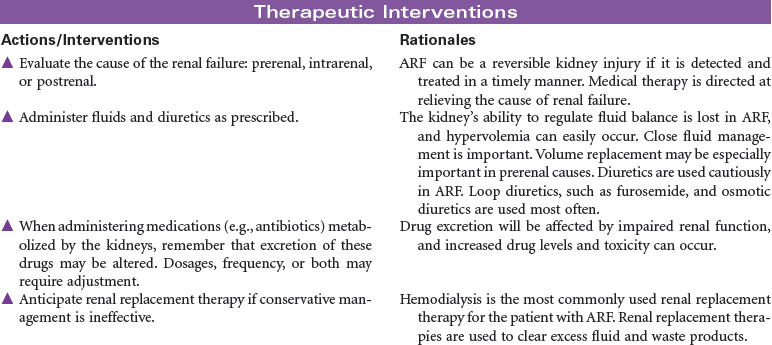
Acute Renal Failure
 For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
Hemodialysis
Renal and Urinary Tract Care Plans
 = Independent
= Independent  = Collaborative
= Collaborative Impaired Renal Function
Impaired Renal Function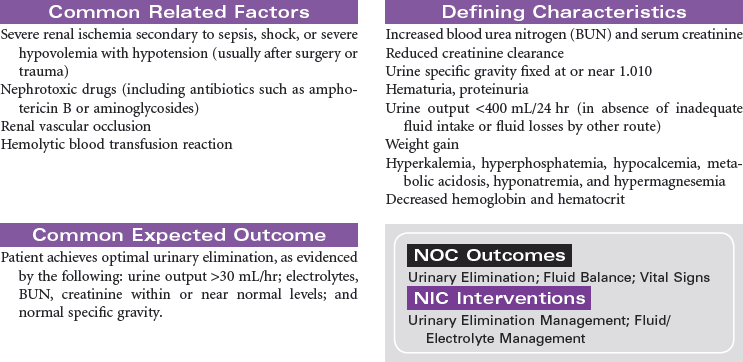
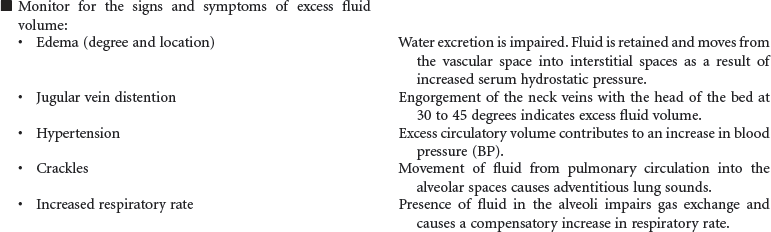
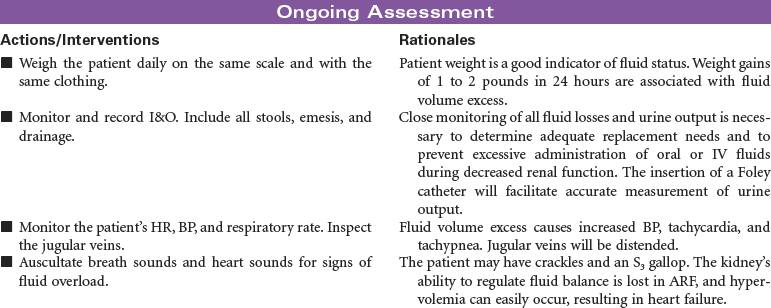
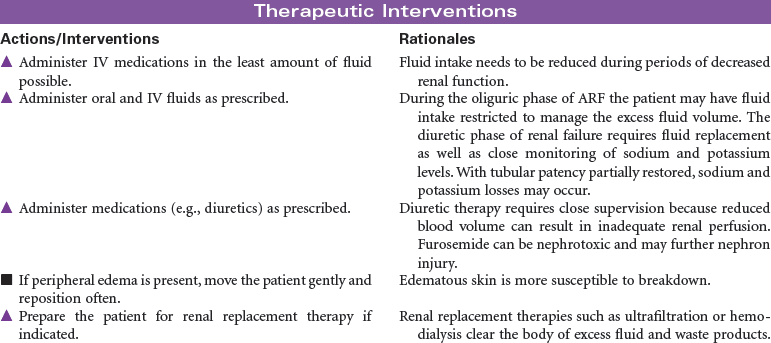
 Excess Fluid Volume
Excess Fluid Volume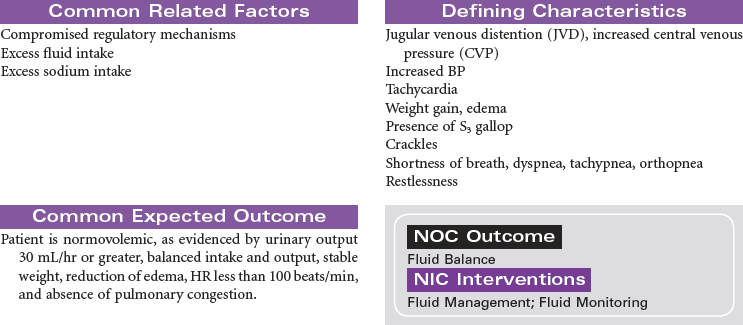
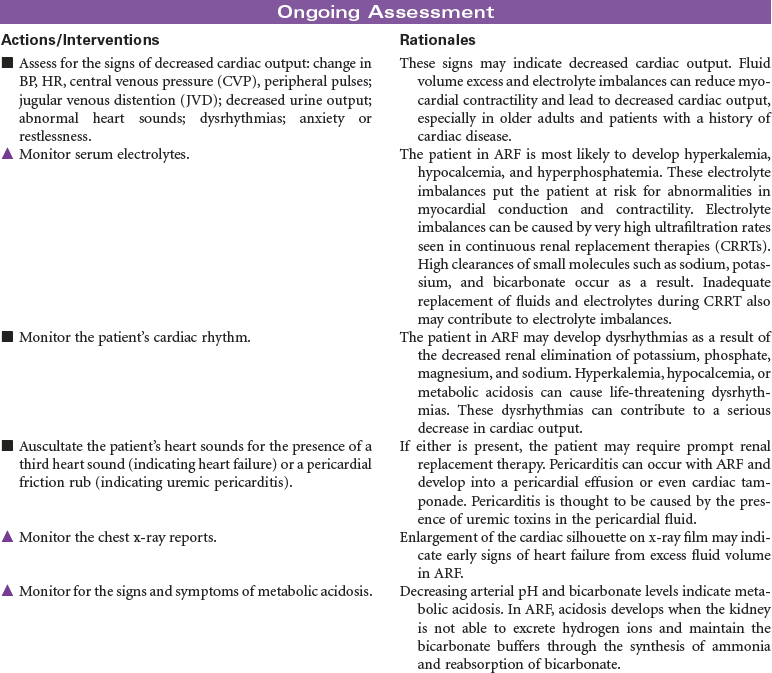
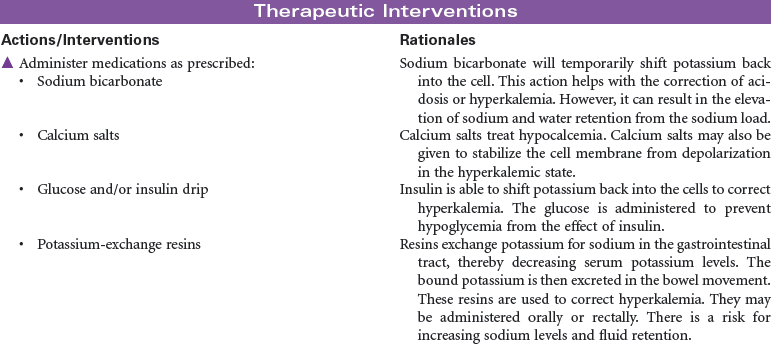
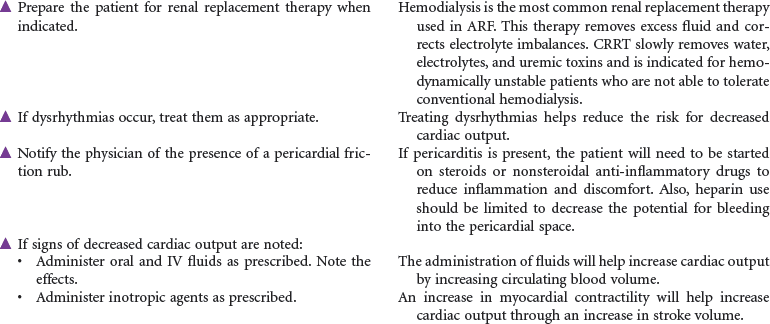
 Risk for Decreased Cardiac Output
Risk for Decreased Cardiac Output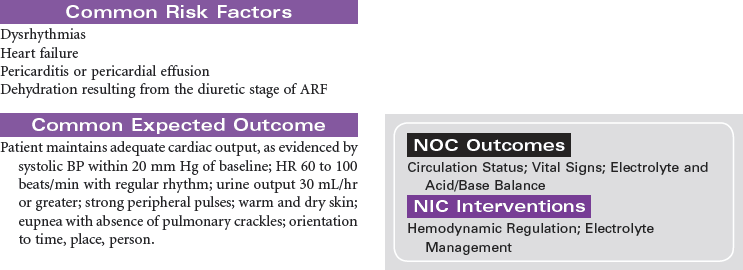
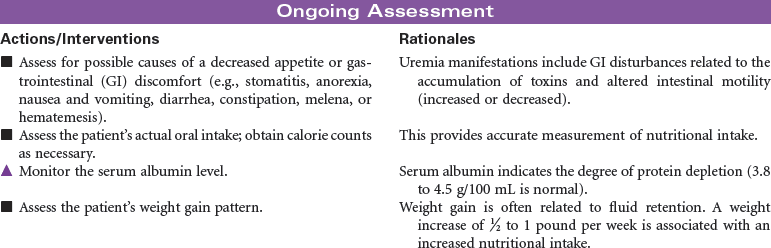
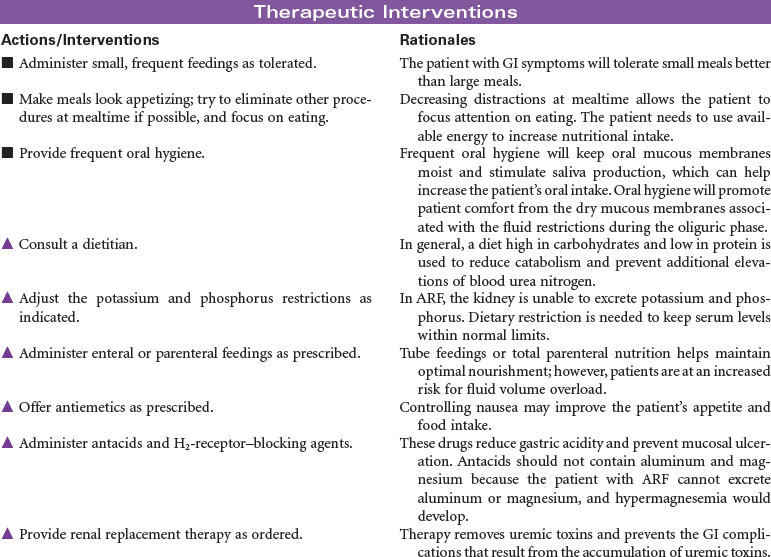
 Imbalanced Nutrition: Less Than Body Requirements
Imbalanced Nutrition: Less Than Body Requirements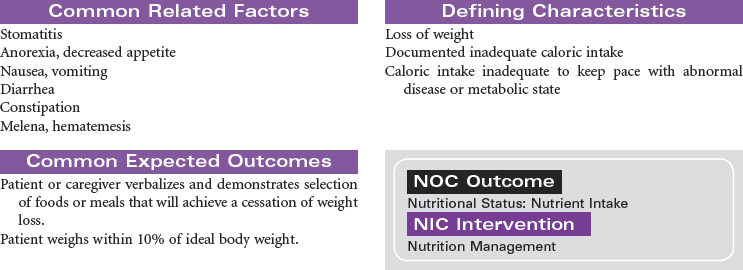
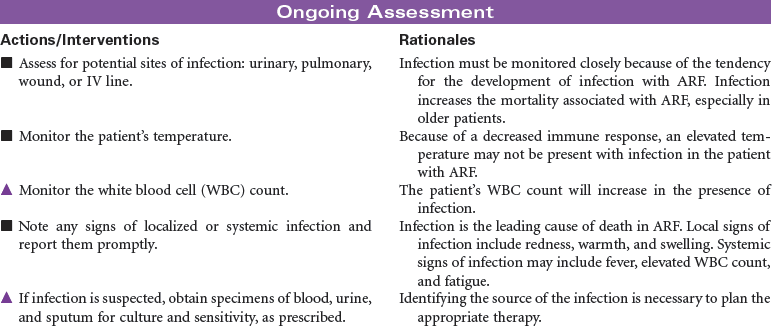
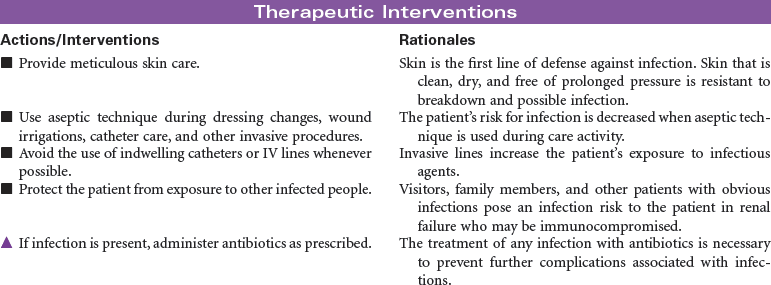
 Risk for Infection
Risk for Infection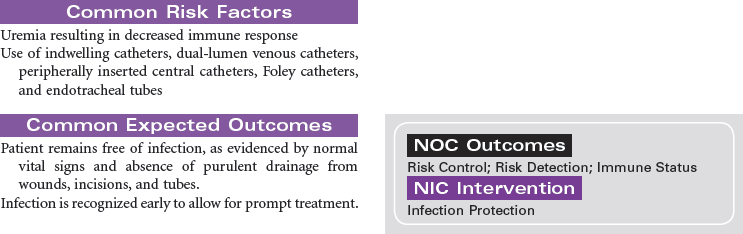
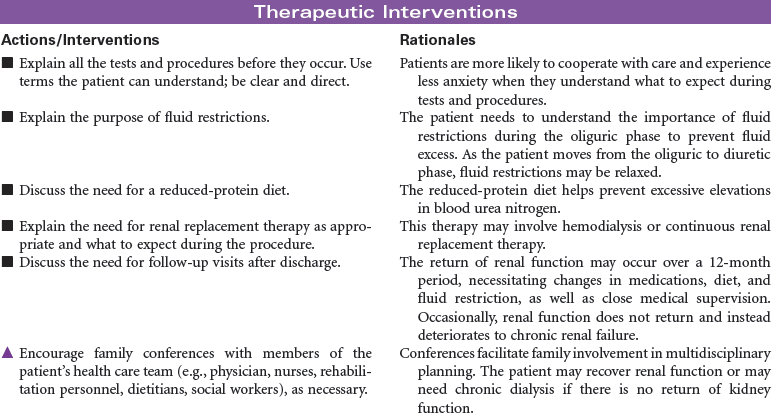
 Deficient Knowledge
Deficient Knowledge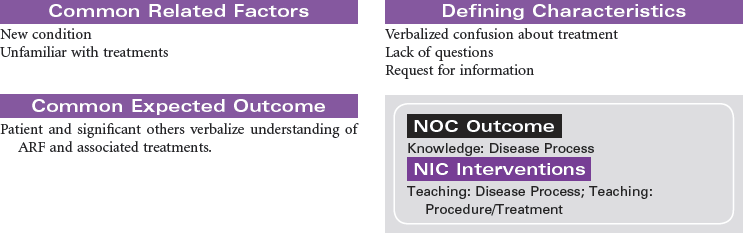

 Risk for Decreased Cardiac Output
Risk for Decreased Cardiac Output
 Risk for Infection
Risk for Infection
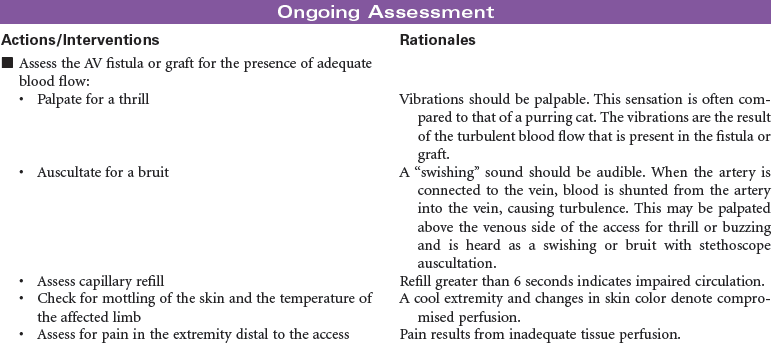
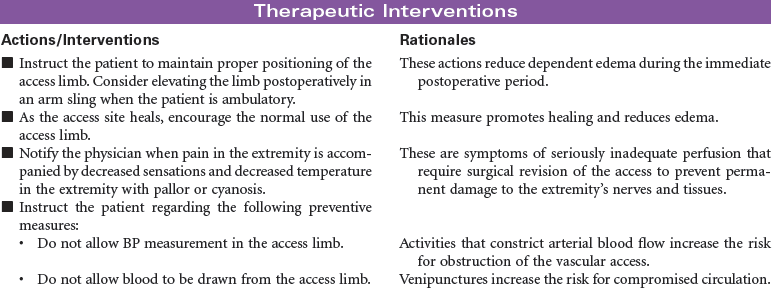
 Risk for Ineffective Peripheral Tissue Perfusion
Risk for Ineffective Peripheral Tissue Perfusion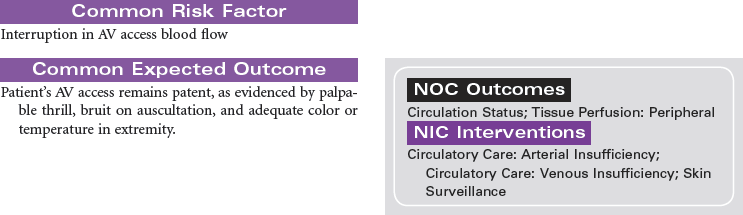

 Deficient Knowledge
Deficient Knowledge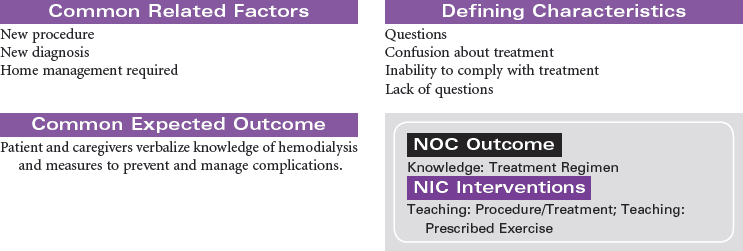
 Excess Fluid Volume
Excess Fluid Volume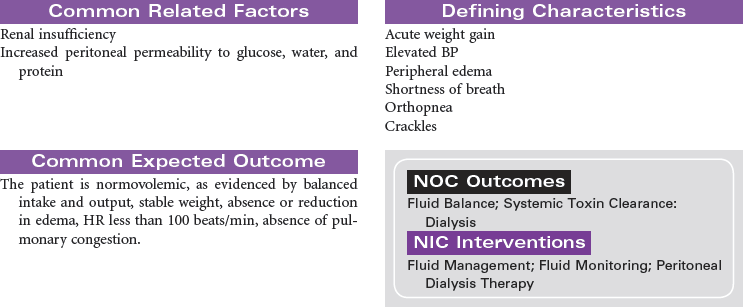



Get Clinical Tree app for offline access
