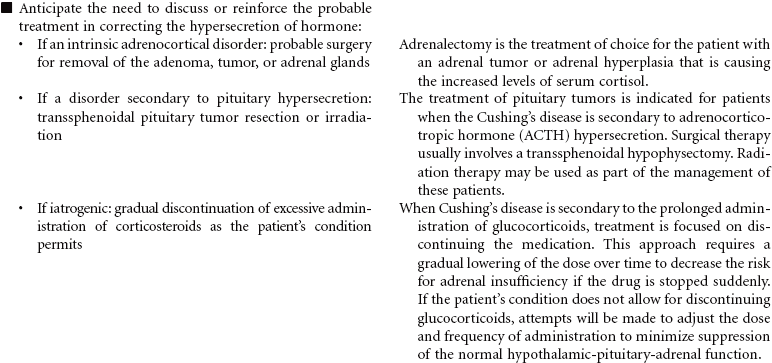
Chapter 14 Endocrine and Metabolic Care Plans For additional care plans, go to http://evolve.elsevier.com/Gulanick/. Cushing’s Disease Hypercortisolism; Cushing’s Syndrome; Adrenocortical Hyperfunction Cushing’s disease reflects an excess of cortisol. Depending on the cause of the disease, mineralocorticoids and androgens also may be secreted in increased amounts. The disorder may be primary (an intrinsic adrenocortical disorder [e.g., neoplasm]), secondary (from pituitary or hypothalamic dysfunction with increased adrenocorticotrophic hormone secretion resulting in glucocorticoid excess), or iatrogenic (from prolonged or excessive administration of corticosteroids). The disease results in fluid and electrolyte disturbances, suppressed immune response, altered fat distribution, and disturbances in protein metabolism. Changes in physical appearance that occur with Cushing’s disease can have significant influence on the patient’s body image and emotional well-being. The focus of this care plan is on the ambulatory patient with Cushing’s disease. Deficient Knowledge Disturbed Body Image Risk for Injury Risk for Excess Fluid Volume Related Care Plans Activity intolerance, p. 8 Diabetes mellitus, p. 912 Ineffective coping, p. 53 Risk for impaired skin integrity, p. 178 Diabetes Mellitus Type 1; Type 2 Diabetes mellitus is a disorder of metabolism in which carbohydrates, fats, and proteins cannot be used for energy. Insulin, a hormone secreted by islet cells of the pancreas, is required to facilitate movement of glucose across cell membranes. Once inside the cell, glucose is the primary metabolic fuel. Type 1 diabetes occurs when the pancreas is no longer able to secrete insulin. This condition occurs as a result of an autoimmune process with destruction of pancreatic beta cells and has its onset between ages 1 and 24 years. The autoimmune process is triggered by a combination of genetic predisposition and environmental stimuli such as a virus. The result of the insulin deficiency is hyperglycemia. It represents 5% to 10% of the cases of diabetes. Type 2 diabetes results because of resistance of peripheral tissue receptors to the effects of insulin. This type of diabetes also has a genetic predisposition for insulin resistance in skeletal muscles, fat cells, and liver cells. Type 2 diabetes is characterized by hyperinsulinemia and hyperglycemia. Over time the beta cells of the pancreas fail to produce sufficient insulin. Its onset is slow and gradual, with many individuals having had the disease 10 years before diagnosis. It represents 90% to 95% of the cases of diabetes. This is usually a condition of middle-aged to older individuals, although a recent increase in the incidence of type 2 diabetes has occurred in children. Obesity is a major factor in the development of type 2 diabetes in both children and adults. Current studies relate waist circumference of 40 inches for men and 35 inches for women to increased risk for this form of diabetes. Diabetes is a major public health problem; more than 16 million individuals, or 6.5% of the population, have the disease. Diabetes causes significant morbidity and mortality. Seventy percent of diabetes-related deaths are from cardiovascular disease. The severity of dyslipidemia and hypertension is higher in the person with type 2 diabetes. Diabetes is the most common single cause of end-stage renal disease in the United States. Diabetic retinopathy is the most frequent cause of new cases of blindness among adults 20 to 74 years of age. Diabetes is the leading cause of nontraumatic lower extremity amputations in the United States. This care plan concentrates on the care of individuals with type 2 diabetes. Risk for Unstable Blood Glucose Level Risk for Ineffective Therapeutic Regimen Management Risk for Injury: Feet Related Care Plans Chronic pain, p. 148 Deficient knowledge, p. 115 Diabetic ketoacidosis and hyperglycemic hyperosmolar nonketotic syndrome, Ineffective sexuality pattern, p. 176 Risk for infection, p. 106 Risk for impaired skin integrity, p. 178 Hyperthyroidism Graves’ Disease Hyperthyroidism occurs as a result of increased circulating levels of thyroid hormones. Women are affected more often than men. The peak age for diagnosis of the disorder is 20 to 40 years. The most common cause is Graves’ disease. This form of hyperthyroidism is an autoimmune disorder that contributes to a failure of the normal regulation of thyroid hormone secretion. Other causes of hyperthyroidism include toxic multinodular goiter, thyroid gland tumors, and pituitary gland tumors. The clinical manifestations of hyperthyroidism develop as a result of the hypermetabolic effects of increased thyroid hormones on all body systems. These manifestations include heat intolerance, irritability, restlessness, goiter, tachycardia, palpitations, increased blood pressure, diaphoresis, weight loss, increased appetite, diarrhea, visual changes, menstrual irregularities, and changes in libido. Thyrotoxic crisis or thyroid storm is a rare but severe form of hyperthyroidism that develops suddenly in response to excessive stress or poorly controlled hormone levels. The management of hyperthyroidism includes drug therapy, radioactive iodine therapy, and surgical removal of all or part of the thyroid gland. Deficient Knowledge Imbalanced Nutrition: Less Than Body Requirements Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Integumentary Care Plans Renal and Urinary Tract Care Plans Cardiac and Vascular Care Plans Nursing Diagnosis Care Plans Stay updated, free articles. Join our Telegram channel Join Tags: Nursing Care Plans Nursing Diagnosis and Intervention Dec 3, 2016 | Posted by admin in NURSING | Comments Off on Endocrine and Metabolic Care Plans Full access? Get Clinical Tree
Chapter 14 Endocrine and Metabolic Care Plans For additional care plans, go to http://evolve.elsevier.com/Gulanick/. Cushing’s Disease Hypercortisolism; Cushing’s Syndrome; Adrenocortical Hyperfunction Cushing’s disease reflects an excess of cortisol. Depending on the cause of the disease, mineralocorticoids and androgens also may be secreted in increased amounts. The disorder may be primary (an intrinsic adrenocortical disorder [e.g., neoplasm]), secondary (from pituitary or hypothalamic dysfunction with increased adrenocorticotrophic hormone secretion resulting in glucocorticoid excess), or iatrogenic (from prolonged or excessive administration of corticosteroids). The disease results in fluid and electrolyte disturbances, suppressed immune response, altered fat distribution, and disturbances in protein metabolism. Changes in physical appearance that occur with Cushing’s disease can have significant influence on the patient’s body image and emotional well-being. The focus of this care plan is on the ambulatory patient with Cushing’s disease. Deficient Knowledge Disturbed Body Image Risk for Injury Risk for Excess Fluid Volume Related Care Plans Activity intolerance, p. 8 Diabetes mellitus, p. 912 Ineffective coping, p. 53 Risk for impaired skin integrity, p. 178 Diabetes Mellitus Type 1; Type 2 Diabetes mellitus is a disorder of metabolism in which carbohydrates, fats, and proteins cannot be used for energy. Insulin, a hormone secreted by islet cells of the pancreas, is required to facilitate movement of glucose across cell membranes. Once inside the cell, glucose is the primary metabolic fuel. Type 1 diabetes occurs when the pancreas is no longer able to secrete insulin. This condition occurs as a result of an autoimmune process with destruction of pancreatic beta cells and has its onset between ages 1 and 24 years. The autoimmune process is triggered by a combination of genetic predisposition and environmental stimuli such as a virus. The result of the insulin deficiency is hyperglycemia. It represents 5% to 10% of the cases of diabetes. Type 2 diabetes results because of resistance of peripheral tissue receptors to the effects of insulin. This type of diabetes also has a genetic predisposition for insulin resistance in skeletal muscles, fat cells, and liver cells. Type 2 diabetes is characterized by hyperinsulinemia and hyperglycemia. Over time the beta cells of the pancreas fail to produce sufficient insulin. Its onset is slow and gradual, with many individuals having had the disease 10 years before diagnosis. It represents 90% to 95% of the cases of diabetes. This is usually a condition of middle-aged to older individuals, although a recent increase in the incidence of type 2 diabetes has occurred in children. Obesity is a major factor in the development of type 2 diabetes in both children and adults. Current studies relate waist circumference of 40 inches for men and 35 inches for women to increased risk for this form of diabetes. Diabetes is a major public health problem; more than 16 million individuals, or 6.5% of the population, have the disease. Diabetes causes significant morbidity and mortality. Seventy percent of diabetes-related deaths are from cardiovascular disease. The severity of dyslipidemia and hypertension is higher in the person with type 2 diabetes. Diabetes is the most common single cause of end-stage renal disease in the United States. Diabetic retinopathy is the most frequent cause of new cases of blindness among adults 20 to 74 years of age. Diabetes is the leading cause of nontraumatic lower extremity amputations in the United States. This care plan concentrates on the care of individuals with type 2 diabetes. Risk for Unstable Blood Glucose Level Risk for Ineffective Therapeutic Regimen Management Risk for Injury: Feet Related Care Plans Chronic pain, p. 148 Deficient knowledge, p. 115 Diabetic ketoacidosis and hyperglycemic hyperosmolar nonketotic syndrome, Ineffective sexuality pattern, p. 176 Risk for infection, p. 106 Risk for impaired skin integrity, p. 178 Hyperthyroidism Graves’ Disease Hyperthyroidism occurs as a result of increased circulating levels of thyroid hormones. Women are affected more often than men. The peak age for diagnosis of the disorder is 20 to 40 years. The most common cause is Graves’ disease. This form of hyperthyroidism is an autoimmune disorder that contributes to a failure of the normal regulation of thyroid hormone secretion. Other causes of hyperthyroidism include toxic multinodular goiter, thyroid gland tumors, and pituitary gland tumors. The clinical manifestations of hyperthyroidism develop as a result of the hypermetabolic effects of increased thyroid hormones on all body systems. These manifestations include heat intolerance, irritability, restlessness, goiter, tachycardia, palpitations, increased blood pressure, diaphoresis, weight loss, increased appetite, diarrhea, visual changes, menstrual irregularities, and changes in libido. Thyrotoxic crisis or thyroid storm is a rare but severe form of hyperthyroidism that develops suddenly in response to excessive stress or poorly controlled hormone levels. The management of hyperthyroidism includes drug therapy, radioactive iodine therapy, and surgical removal of all or part of the thyroid gland. Deficient Knowledge Imbalanced Nutrition: Less Than Body Requirements Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Integumentary Care Plans Renal and Urinary Tract Care Plans Cardiac and Vascular Care Plans Nursing Diagnosis Care Plans Stay updated, free articles. Join our Telegram channel Join Tags: Nursing Care Plans Nursing Diagnosis and Intervention Dec 3, 2016 | Posted by admin in NURSING | Comments Off on Endocrine and Metabolic Care Plans Full access? Get Clinical Tree
 For additional care plans, go to
For additional care plans, go to  Deficient Knowledge
Deficient Knowledge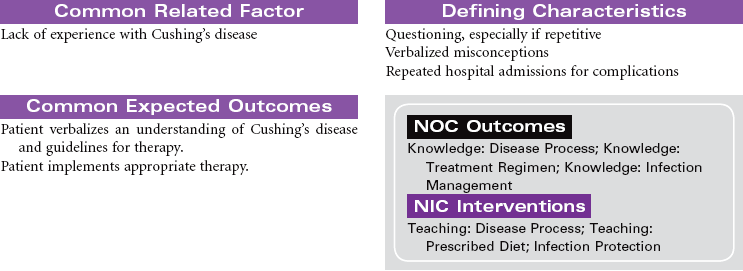
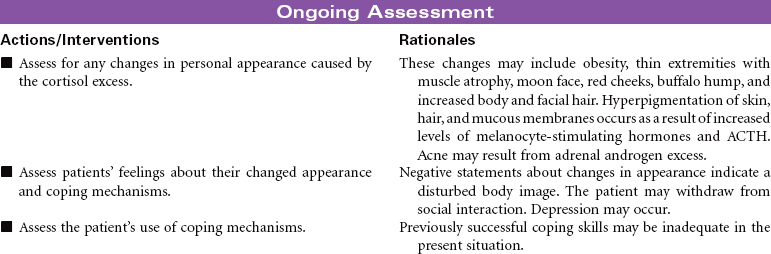
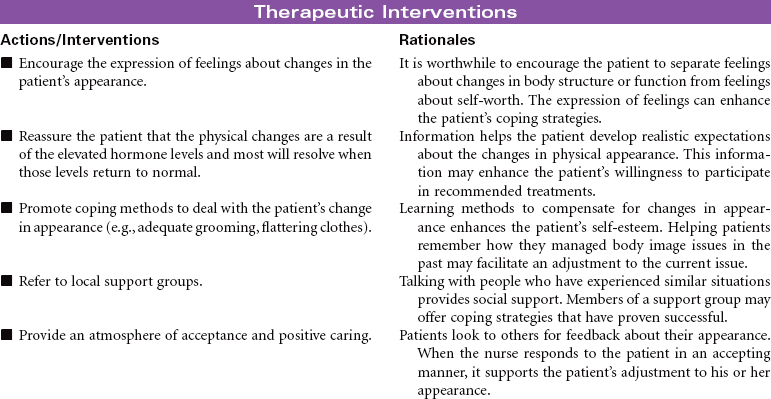
 Disturbed Body Image
Disturbed Body Image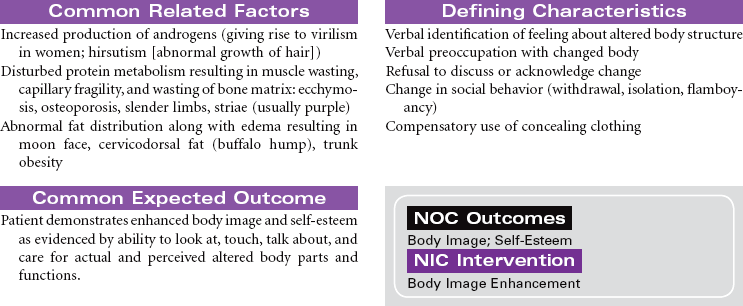
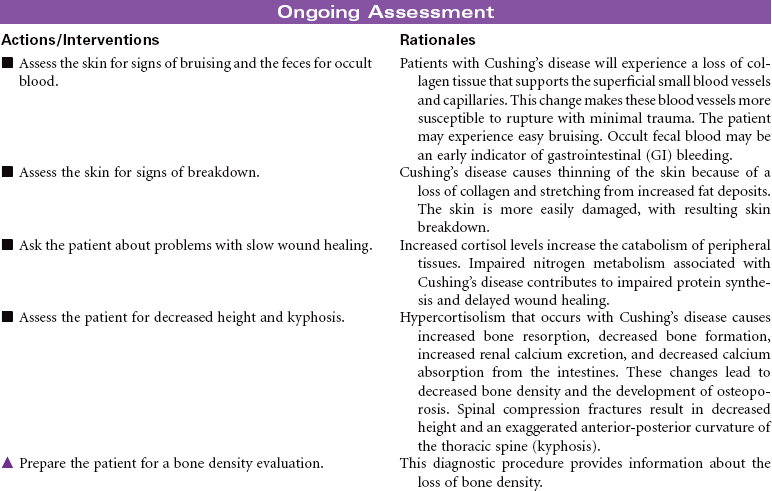
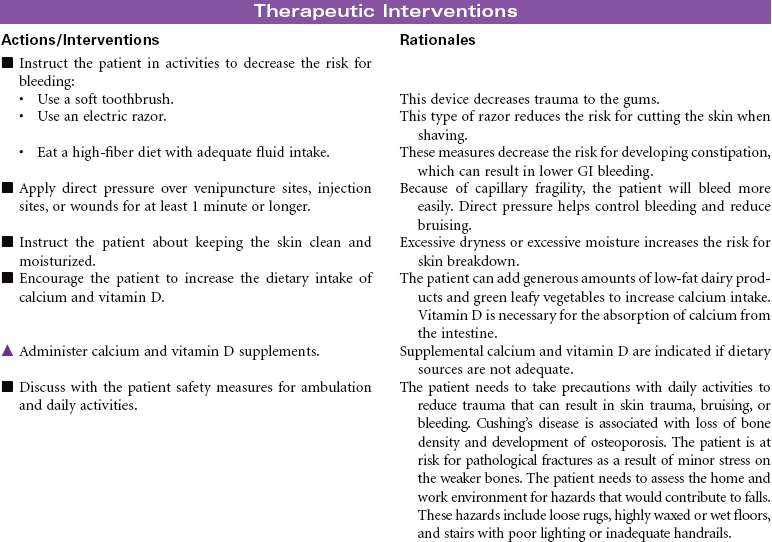
 Risk for Injury
Risk for Injury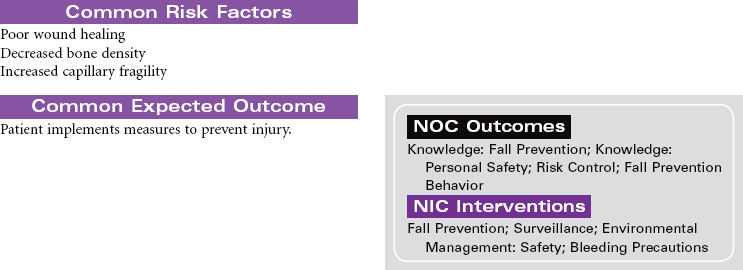
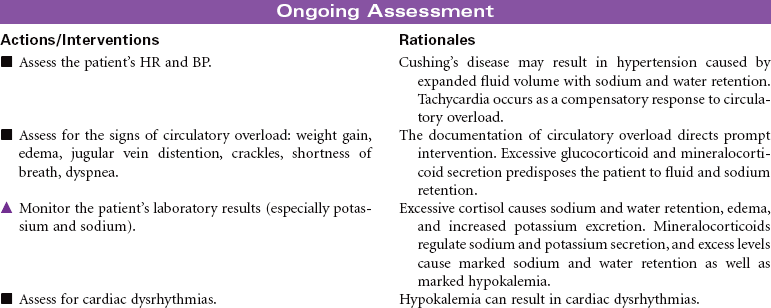
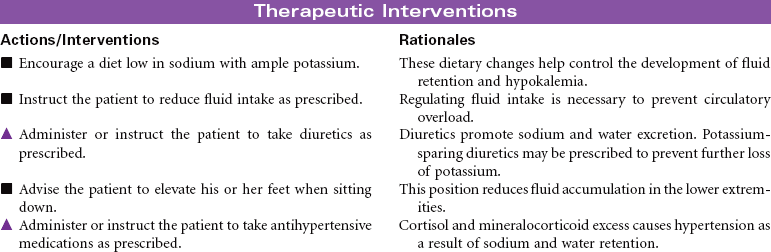
 Risk for Excess Fluid Volume
Risk for Excess Fluid Volume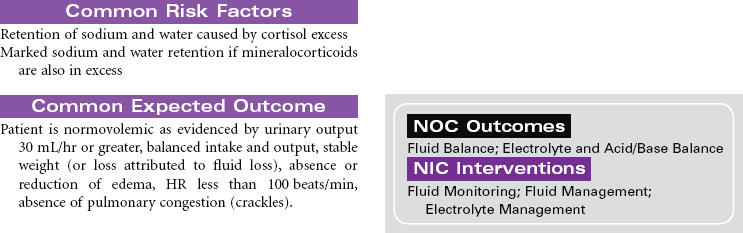
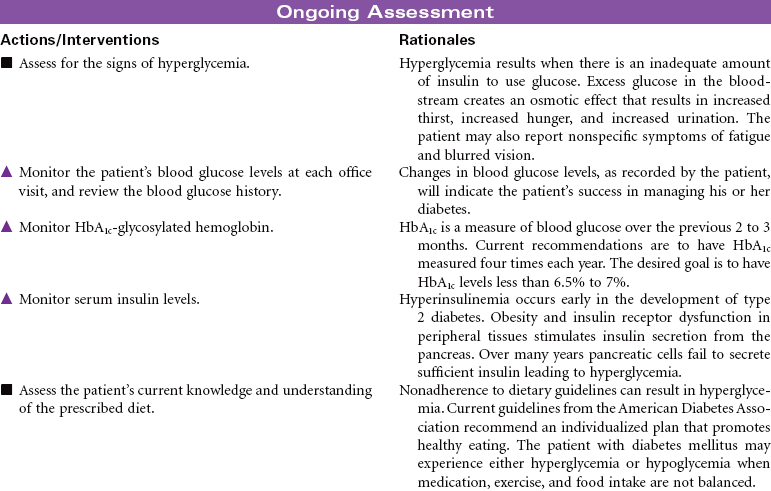
 Risk for Unstable Blood Glucose Level
Risk for Unstable Blood Glucose Level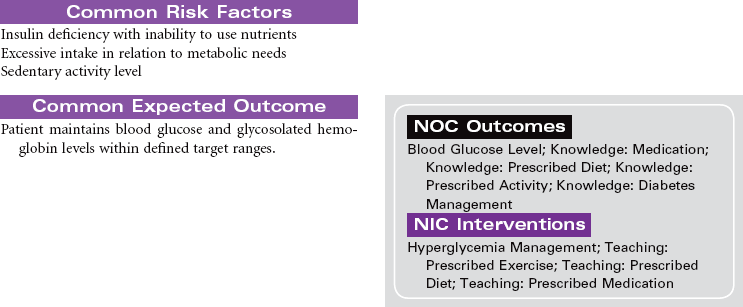
 Risk for Ineffective Therapeutic Regimen Management
Risk for Ineffective Therapeutic Regimen Management
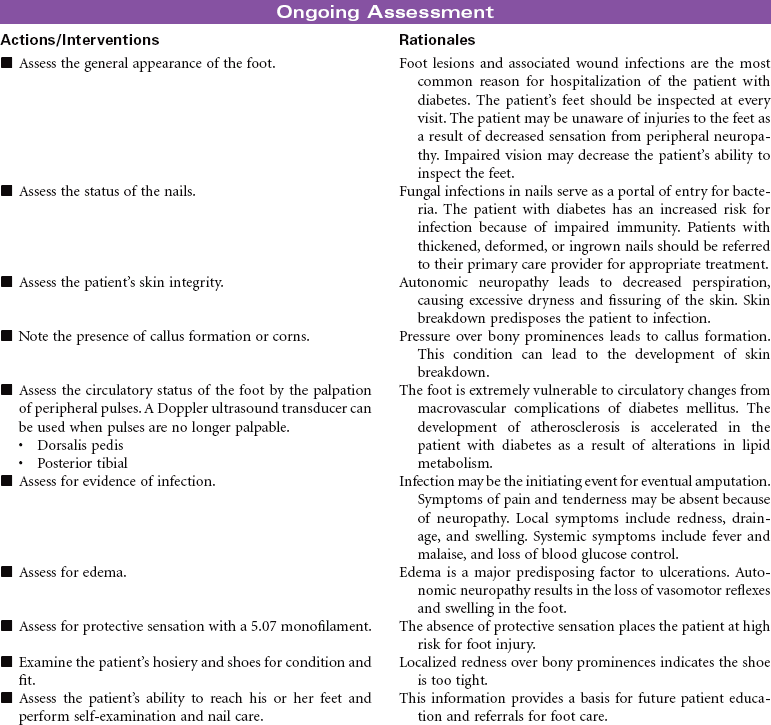
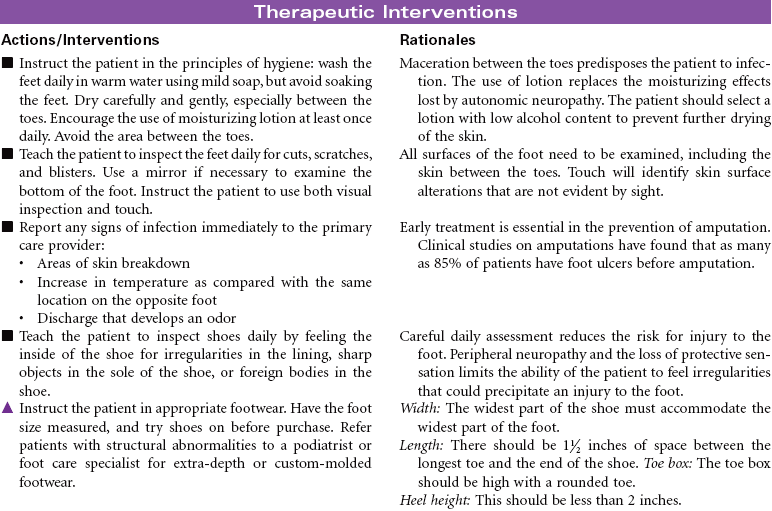
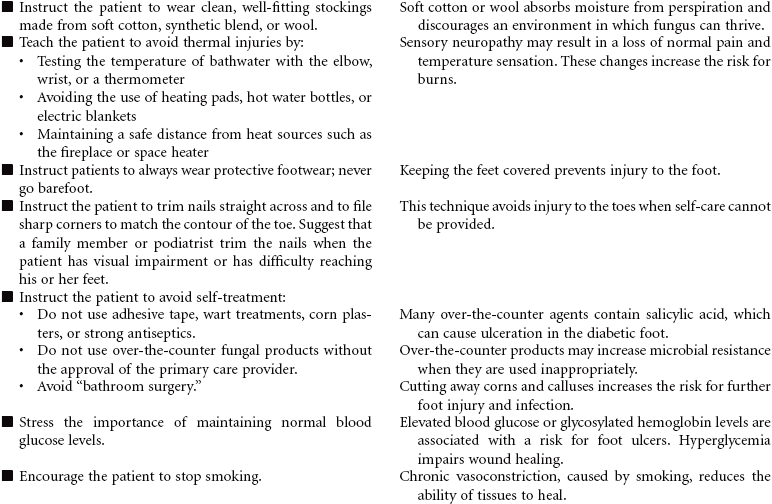
 Risk for Injury: Feet
Risk for Injury: Feet

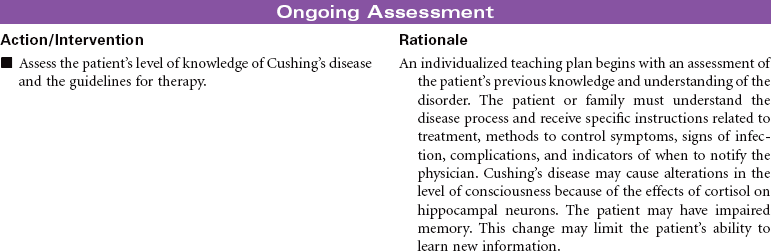
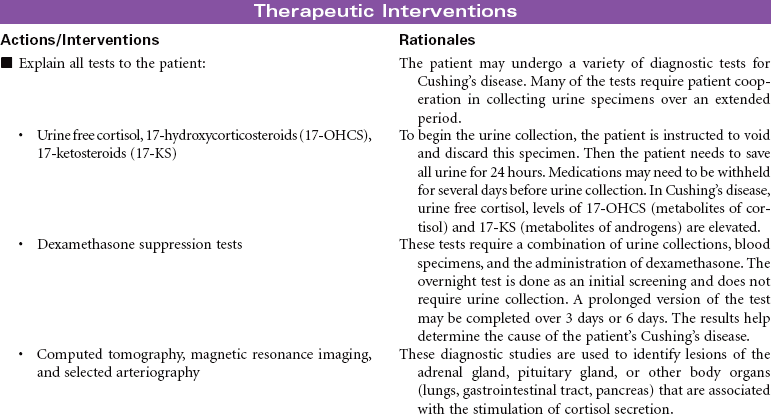
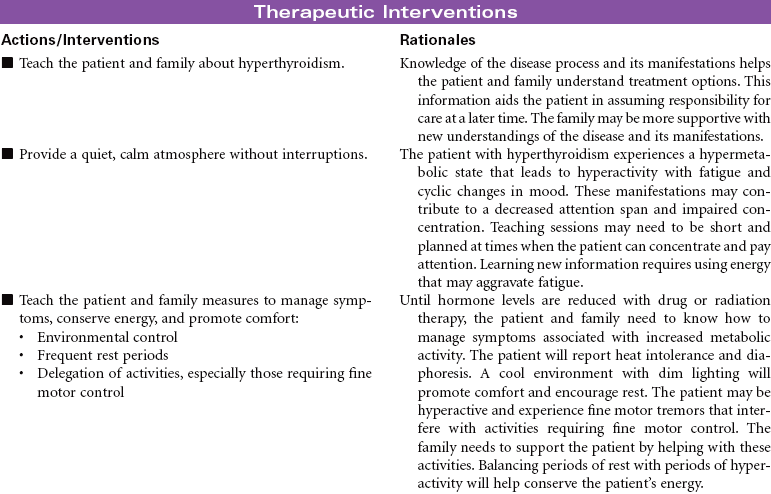
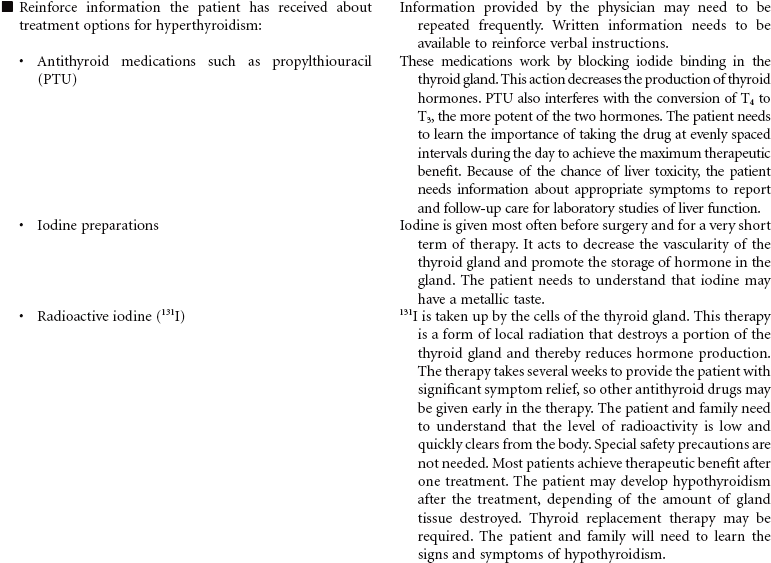
 Deficient Knowledge
Deficient Knowledge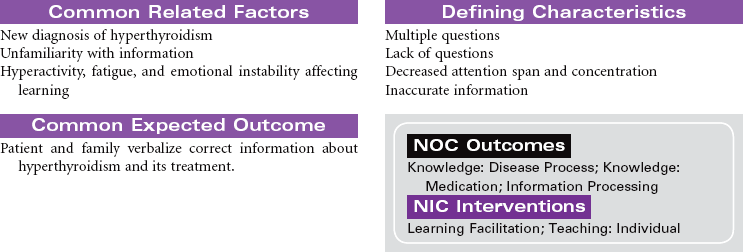


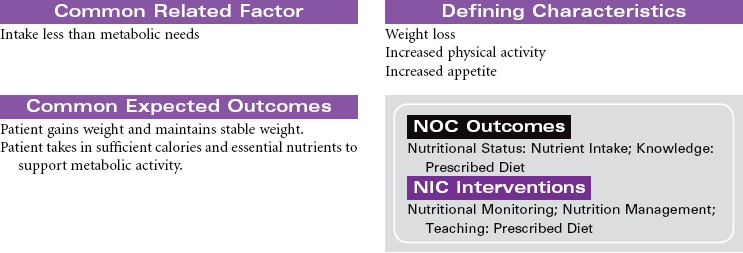
 Imbalanced Nutrition: Less Than Body Requirements
Imbalanced Nutrition: Less Than Body Requirements