Chapter 2 Pulmonology
Basic concepts—mechanics of breathing
2 What are the forces of resistance for the following:


Tissue resistance is generated as the pleural surfaces slide over each other during respiration. This resistance is normally minimal because of the presence of pleural fluid. Note that tissue resistance can increase markedly in conditions in which the pleural surfaces become adherent to each other, as may occur with an empyema (Fig. 2-1).
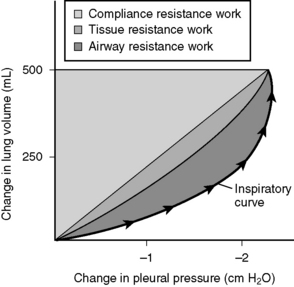
Figure 2-1 Relative contributions of the three types of resistance to the total work of breathing.
(From Brown TA: Rapid Review Physiology. Philadelphia, Mosby, 2007.)

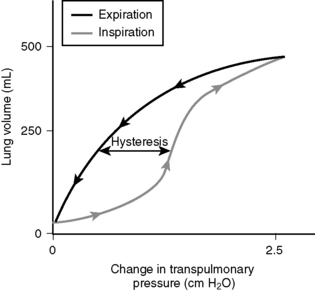
4 With respect to the compliance curve of the lungs, how might breathing at an elevated functional residual capacity in chronic obstructive pulmonary disease result in less “efficient” breathing?
Figure 2-2 shows a compliance curve of the lungs. Note that the lungs are most compliant in the midportion of the inspiratory curve (steepest slope). Breathing at an elevated functional residual capacity (as patients with chronic obstructive pulmonary disease [COPD] are prone to do for a variety of reasons) is less efficient and requires more work.
5 What does pulmonary elastance measure? How is pulmonary elastance altered in restrictive and obstructive lung diseases and why?

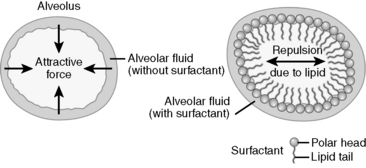
6 How does surfactant affect alveolar surface tension?
Water molecules lining the surface of alveoli are attracted to each other and are repelled by the hydrophobic air molecules. The attractive force between water molecules generates surface tension, which in turn produces a collapsing pressure that promotes alveolar collapse. Surfactant is composed of phospholipids (mainly lecithin and sphingomyelin) that reduce the collapsing pressure by minimizing the interaction between alveolar fluid and alveolar air (Fig. 2-3).
7 Why are smaller alveoli more prone to collapse, and how is this relevant to neonatal respiratory distress syndrome?



9 What is “dead space”? What is the difference between anatomic dead space and physiologic dead space?

Basic concepts—ventilation-perfusion matching
11 What does the ventilation/perfusion ratio measure, and what is its approximate value? What is an “ideal” value for this ratio?
 /
/ ) measures how well pulmonary perfusion and pulmonary ventilation are matched, indicating how efficiently oxygenation of blood is occurring in the pulmonary capillaries. Normally, the lungs receive close to the entire cardiac output (~5 L/min), and the prototypical 70-kg man has an alveolar ventilation rate of roughly 4 L/min (as shown in question 10). A ventilation rate of 4 L/min and a pulmonary perfusion rate of 5 L/min yield a
) measures how well pulmonary perfusion and pulmonary ventilation are matched, indicating how efficiently oxygenation of blood is occurring in the pulmonary capillaries. Normally, the lungs receive close to the entire cardiac output (~5 L/min), and the prototypical 70-kg man has an alveolar ventilation rate of roughly 4 L/min (as shown in question 10). A ventilation rate of 4 L/min and a pulmonary perfusion rate of 5 L/min yield a  /
/ ratio of 0.8, which implies suboptimal matching of pulmonary ventilation and perfusion. A
ratio of 0.8, which implies suboptimal matching of pulmonary ventilation and perfusion. A  /
/ ratio of 1 is ideal, and represents optimal matching of pulmonary ventilation and perfusion.
ratio of 1 is ideal, and represents optimal matching of pulmonary ventilation and perfusion. /
/ ratio can be applied to the lungs as a whole, or to separate areas of the lungs, and is a measure of the efficiency of ventilation in those separate areas as well. Regional differences in ventilation and perfusion exist across various zones of the lungs because of the force of gravity. In an upright subject, both blood flow and perfusion are decreased at the apex of the lung and increased at the base of the lung. However, the decrease in perfusion is greater than the decrease in ventilation at the apex of the lung, leading to an increased
ratio can be applied to the lungs as a whole, or to separate areas of the lungs, and is a measure of the efficiency of ventilation in those separate areas as well. Regional differences in ventilation and perfusion exist across various zones of the lungs because of the force of gravity. In an upright subject, both blood flow and perfusion are decreased at the apex of the lung and increased at the base of the lung. However, the decrease in perfusion is greater than the decrease in ventilation at the apex of the lung, leading to an increased  /
/ ratio. Likewise, the
ratio. Likewise, the  /
/ ratio at the base is decreased because the increase in perfusion is greater than the increase in ventilation. This difference leads to an apical
ratio at the base is decreased because the increase in perfusion is greater than the increase in ventilation. This difference leads to an apical  /
/ ratio of 3, while the basal
ratio of 3, while the basal  /
/ ratio is closer to 0.6.
ratio is closer to 0.6. /
/ ratio from apex to base that more closely approximates the ideal
ratio from apex to base that more closely approximates the ideal  /
/ ratio of 1.0.
ratio of 1.0. /
/ ratio?
ratio? /
/ ratio increases whenever pulmonary ventilation is proportionately greater than pulmonary perfusion. As just discussed, exercise is a normal situation in which ventilation increases proportionally more than perfusion, and in this case it optimizes the
ratio increases whenever pulmonary ventilation is proportionately greater than pulmonary perfusion. As just discussed, exercise is a normal situation in which ventilation increases proportionally more than perfusion, and in this case it optimizes the  /
/ ratio. A pathologic condition that increases the
ratio. A pathologic condition that increases the  /
/ ratio is a pulmonary embolus. In this condition, patients are often tachypneic (respiring rapidly), which increases ventilation. The clot in the lungs also reduces pulmonary perfusion, so both of these processes increase the
ratio is a pulmonary embolus. In this condition, patients are often tachypneic (respiring rapidly), which increases ventilation. The clot in the lungs also reduces pulmonary perfusion, so both of these processes increase the  /
/ ratio. In fact, the
ratio. In fact, the  /
/ ratio in the blocked segment would theoretically approach infinity because blood flow to that region is completely blocked (
ratio in the blocked segment would theoretically approach infinity because blood flow to that region is completely blocked ( = 0). The pathologic consequence of an increased
= 0). The pathologic consequence of an increased  /
/ ratio is that ventilation is “wasted” in lung areas that are not adequately perfused.
ratio is that ventilation is “wasted” in lung areas that are not adequately perfused. /
/ ratio.
ratio. /
/ ratio will respond to oxygen administration. However, a
ratio will respond to oxygen administration. However, a  /
/ ratio of 0 generally implies an obstructed mainstem bronchus and will not respond to oxygen.
ratio of 0 generally implies an obstructed mainstem bronchus and will not respond to oxygen.14 What effect does chronic obstructive pulmonary disease usually have on the ventilation-perfusion ratio?
 /
/ ratio. However, pulmonary capillary loss in COPD can increase ventilation relative to perfusion, causing an increased
ratio. However, pulmonary capillary loss in COPD can increase ventilation relative to perfusion, causing an increased  /
/ ratio. In fact, if these two processes are occurring in the same patient, this patient can have a normal
ratio. In fact, if these two processes are occurring in the same patient, this patient can have a normal  /
/ ratio despite severe ventilation/perfusion mismatches in different parts of the lung!
ratio despite severe ventilation/perfusion mismatches in different parts of the lung! /
/ ratio of 0.
ratio of 0.Basic concepts—gas exchange
16 What influences the diffusion of gases from the alveoli into the pulmonary capillaries, and vice versa?
where Vgas is the volume of gas that traverses the membrane per unit time, A is the surface area of the membrane, D is the diffusivity of the particular gas in the particular membrane, P1 − P2 is the partial pressure difference of the specific gas across the membrane, and T is the thickness of the membrane.
17 What is the alveolar-arterial oxygen gradient and what is the clinical significance of its magnitude?
18 How is the alveolar-arterial oxygen gradient calculated?

where

where FIO2 = the fraction of inspired oxygen (usually 0.21), PB is barometric pressure (usually 760 mm Hg), PH2O is water vapor pressure (usually 47 mm Hg), PACO2 = alveolar pressure of carbon dioxide, which equals the arterial pressure of carbon dioxide due to rapid diffusion across the alveolar membrane, and R = the respiratory quotient (usually 0.8).
20 How does increasing or decreasing the arterial PCO2 affect pH?
When CO2 dissolves in water, the following reaction occurs:

where CA is carbonic anhydrase.
23 What is the principal difference between “restrictive” and “obstructive” lung disease with respect to the FEV1/FVC ratio?
Table 2-1 lists some examples of obstructive and restrictive lung diseases.
Table 2-1 Obstructive and Restrictive Lung Diseases
| Obstructive Lung Diseases | Restrictive Lung Diseases |
|---|---|
| Chronic bronchitis Emphysema Asthma Bronchiectasis Cystic fibrosis | Neuromuscular diseases (poliomyelitis, myasthenia gravis, Duchenne muscular dystrophy, Guillain-Barré syndrome) Acute respiratory distress syndrome (ARDS) Neonatal respiratory distress syndrome Sarcoidosis Idiopathic pulmonary fibrosis Goodpasture’s syndrome Wegener’s granulomatosis Drug toxicity Pleural diseases |
4 About 5% of asthmatics are sensitive to aspirin, and some may even develop fatal bronchospasm from ingesting aspirin. What is currently believed to be the biochemical basis of this?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


