Chapter 13 Bleeding Disorders
Basic concepts
1 Differentiate between the processes of primary and secondary hemostasis
Primary hemostasis involves the formation of a temporary platelet “plug” following binding of platelets to exposed collagen, platelet secretion of procoagulant substances (e.g., adenosine diphosphate [ADP], Ca2+), and platelet aggregation. This platelet plug is referred to as temporary because it is readily reversible at this stage. Secondary hemostasis involves the covalent cross-linking of fibrin between platelets, resulting in the formation of an irreversible platelet plug. This process is dependent on activation of the coagulation cascade (Table 13-1).
Table 13-1 Primary and Secondary Hemostasis
| Feature | Primary Hemostasis | Secondary Hemostasis |
|---|---|---|
| Definition | Temporary platelet plug | Permanent platelet plug |
| Example disease(s) | Von Willebrand disease | Hemophilia A and B |
| Laboratory testing | Bleeding time, platelet aggregation studies | Prothrombin time (PT), partial thromboplastin time (PTT) |
| Clinical manifestations of disturbed mechanism | Relatively mild (e.g., excessive bleeding after dental work or surgery), mucocutaneous petechiae | Relatively severe (e.g., hemarthrosis) |
3 What constitutes the extrinsic, intrinsic, and common pathways in the coagulation cascade that forms the fibrin clot (secondary hemostasis)?
As mentioned, the common pathway is activated by either the extrinsic pathway or intrinsic pathway, and it eventuates in the formation of a fibrin clot. This pathway includes factors X, V, II, and I (Fig. 13-1).

4 What information can be provided by measuring the prothrombin time and activated partial thromboplastin time?
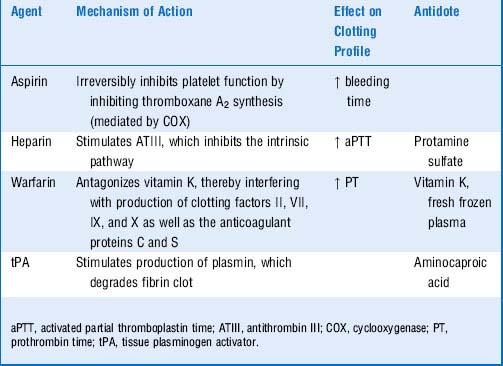
6 What is the mechanism of action of the following drugs? How do they affect the times just discussed?
7 What is the mechanism of action of tissue plasminogen activator?
As its name suggests, tissue plasminogen activator (tPA) is an enzyme that activates the plasma enzyme plasminogen by converting it into its active form, plasmin. Plasmin is an enzyme that proteolytically cleaves fibrin strands, thereby degrading fibrin clots that may obstruct vessels. In addition to tPA, streptokinase and urokinase are sometimes referred to as “clot busters” (Table 13-2).
Summary Box: Hemostasis, Coagulation Cascade, Pharmacotherapy











2 What is the cause of this disorder and how is it inherited?
Hemophilia A is caused by a hereditary deficiency of factor VIII and is inherited in an X-linked recessive manner. Females are very rarely affected because the approximate 50% factor levels in most carriers are sufficient to prevent excessive bleeding. In rare circumstances, females may be affected due to unequal inactivation (lyonization) of factor VIII or factor IX alleles (see Chapter 11, Genetic and Metabolic Disease, for more information).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


