Chapter 6 Noncardiogenic Pulmonary Edema; Stiff Lung; Shock Lung; Wet Lung Radical Neck Surgery; Laryngectomy
Pulmonary Care Plans
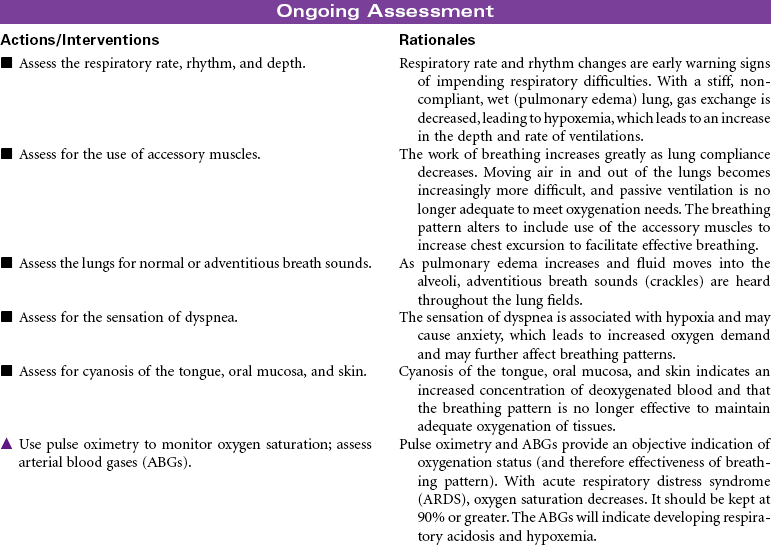
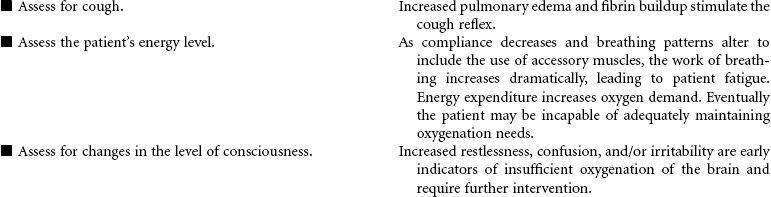
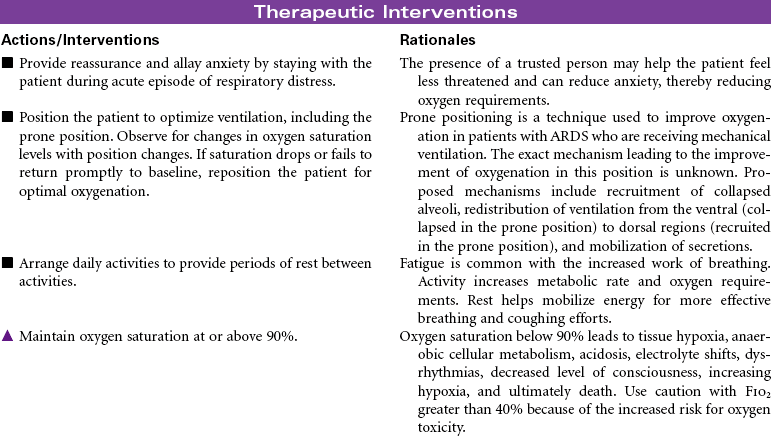
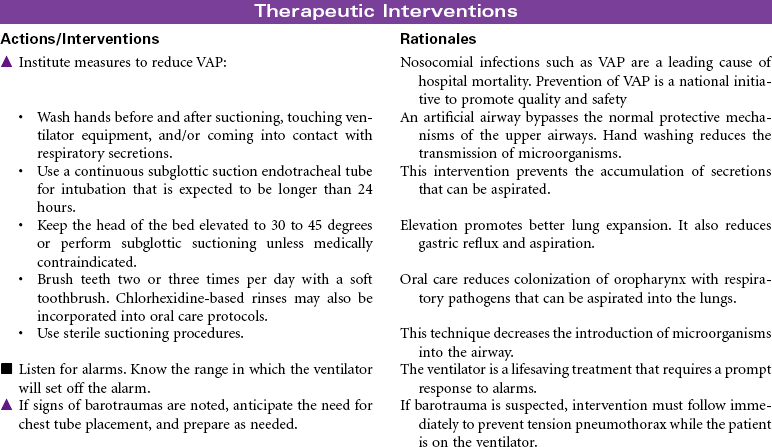
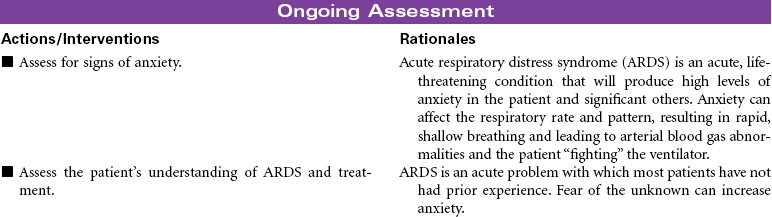
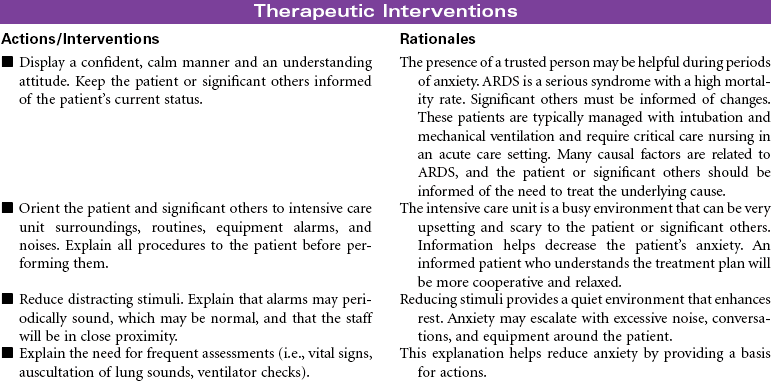
Acute Respiratory Distress Syndrome (ARDS)
 For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.
Head and Neck Cancer: Surgical Approaches
Pulmonary Care Plans
 = Independent
= Independent  = Collaborative
= Collaborative Ineffective Breathing Pattern
Ineffective Breathing Pattern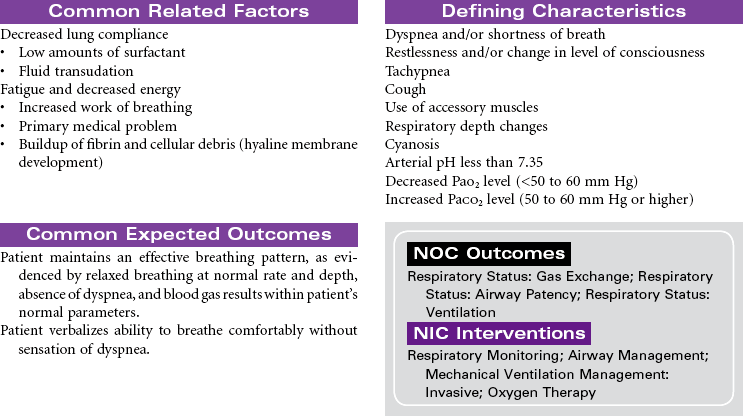
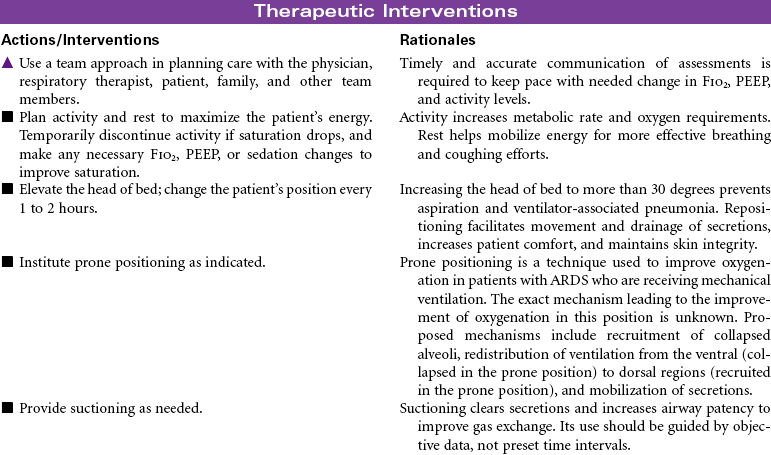
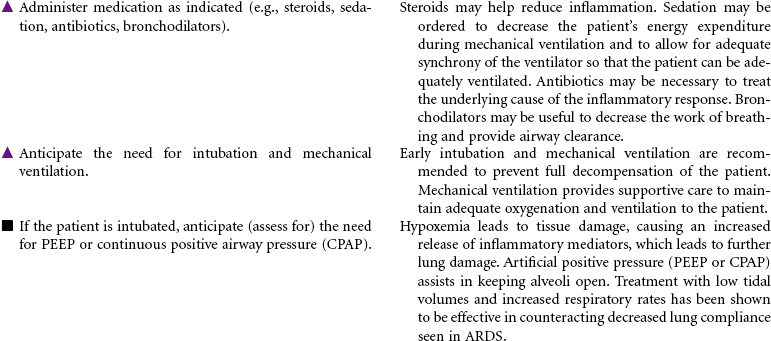
 Impaired Gas Exchange
Impaired Gas Exchange
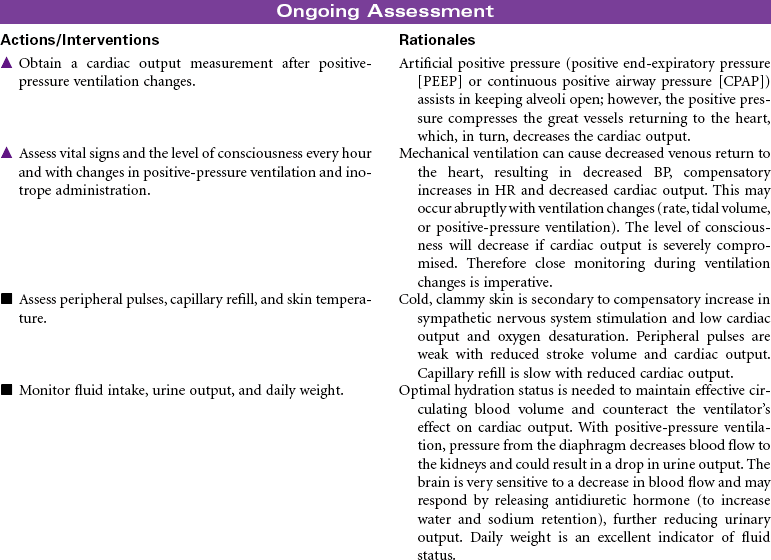
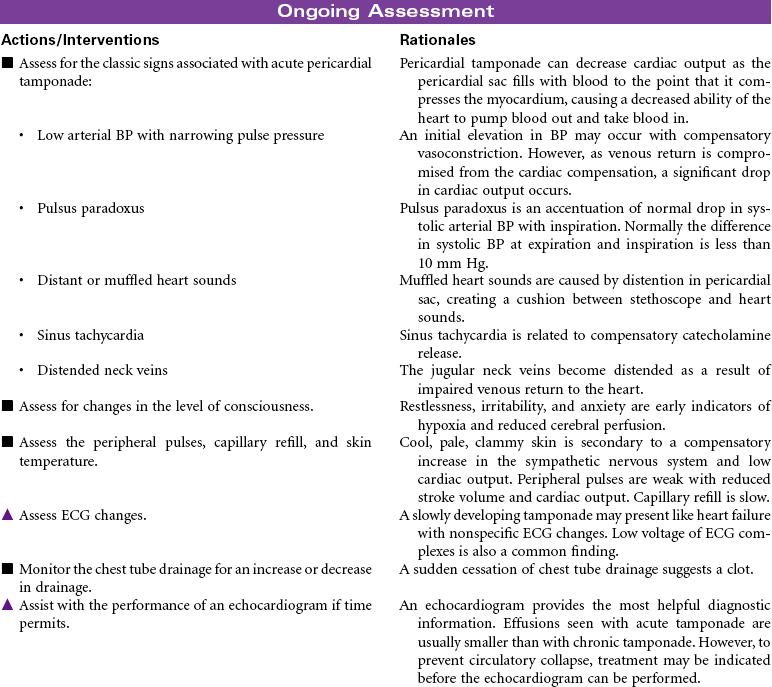
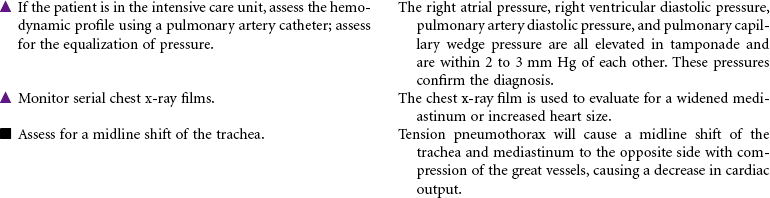
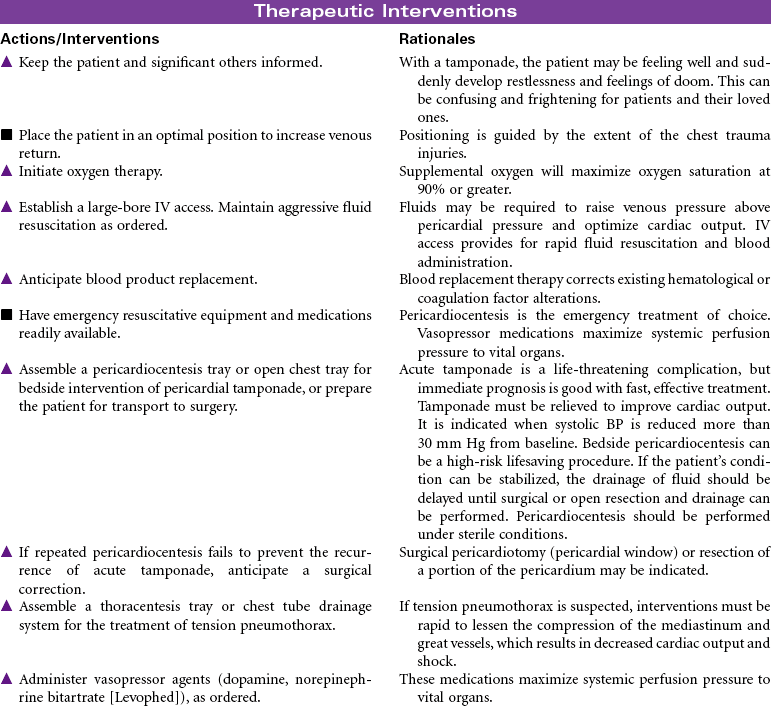
 Risk for Decreased Cardiac Output
Risk for Decreased Cardiac Output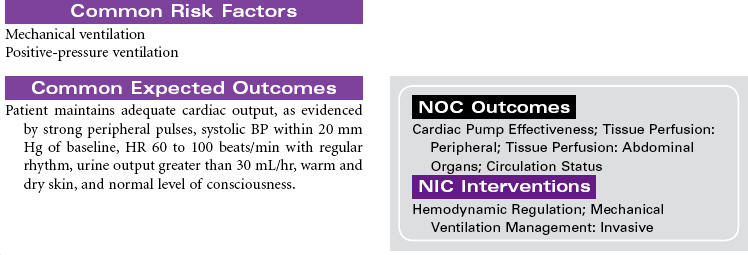
 Risk for Ineffective Protection
Risk for Ineffective Protection
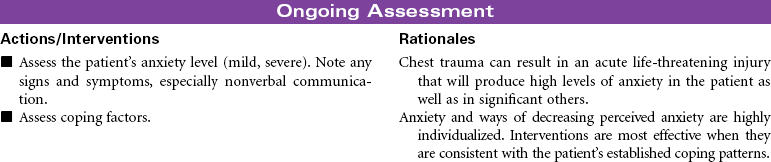
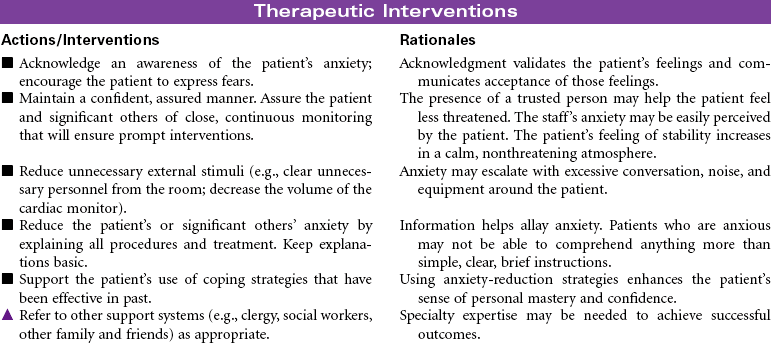
 Anxiety
Anxiety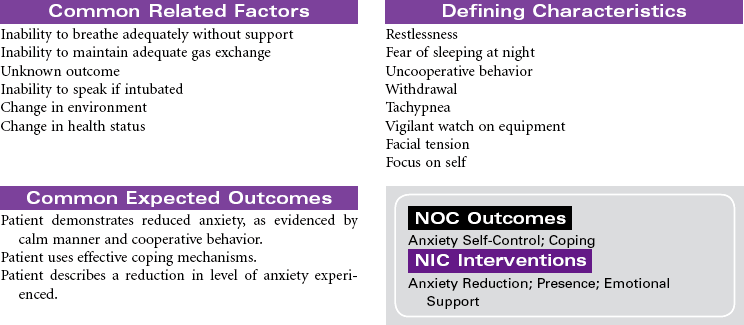

 Ineffective Breathing Pattern
Ineffective Breathing Pattern
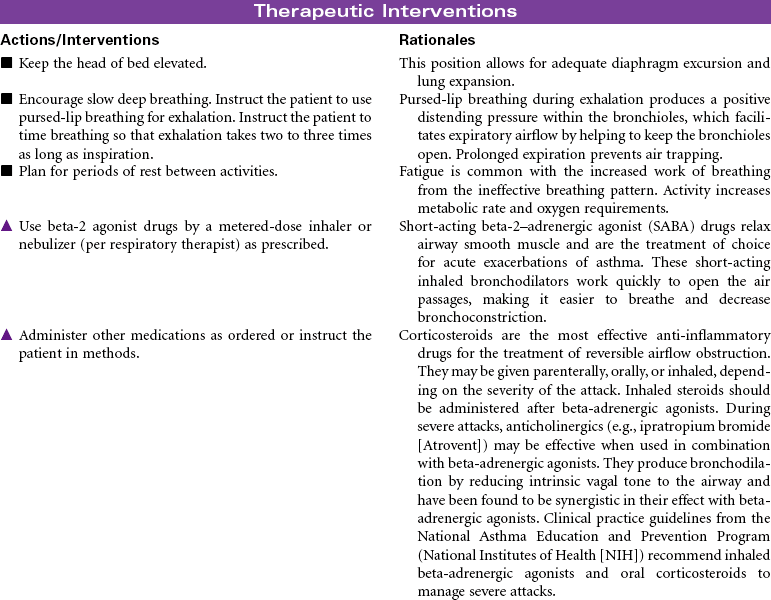
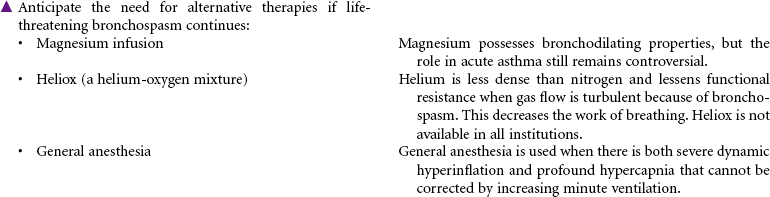
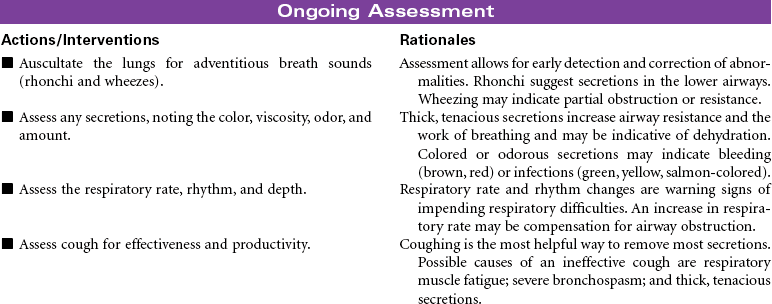
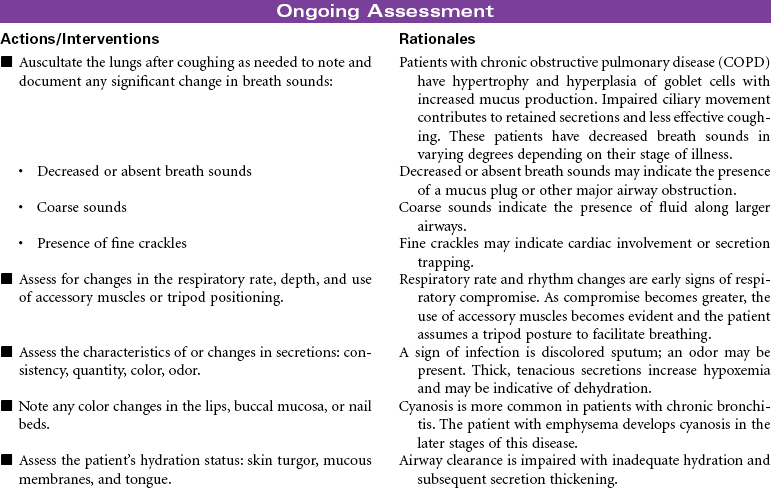
 Ineffective Airway Clearance
Ineffective Airway Clearance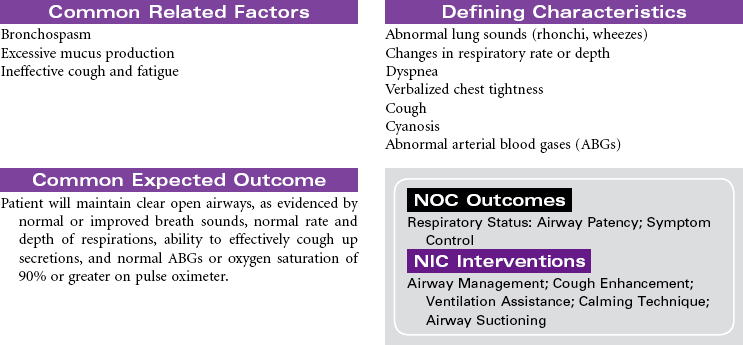
 Anxiety
Anxiety
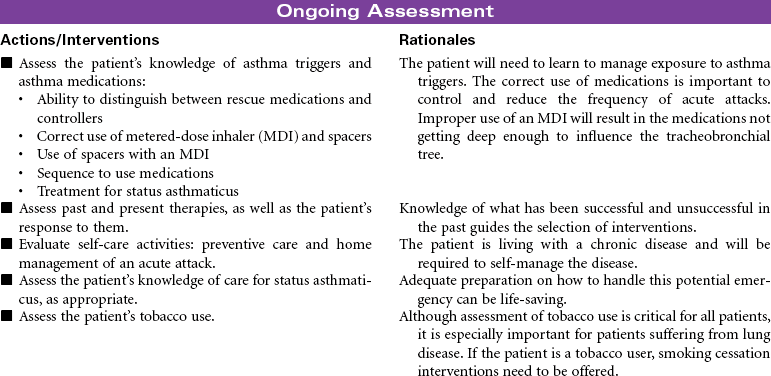
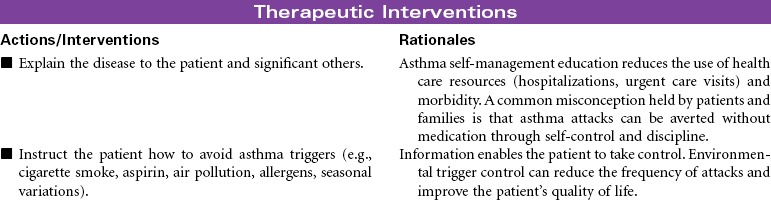
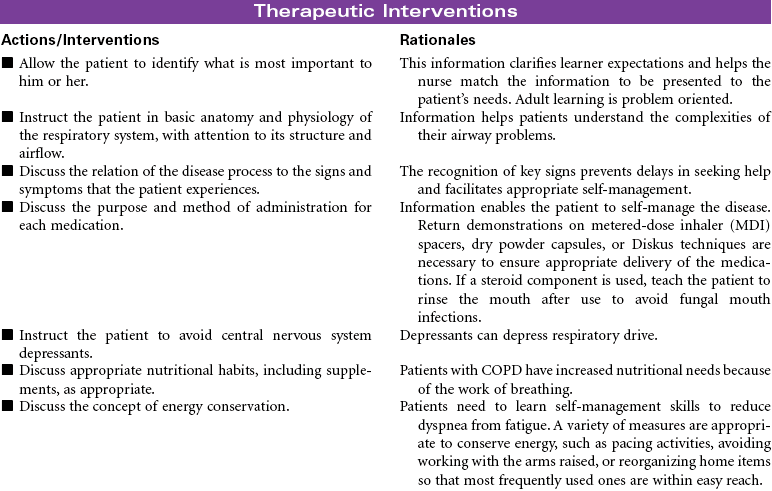
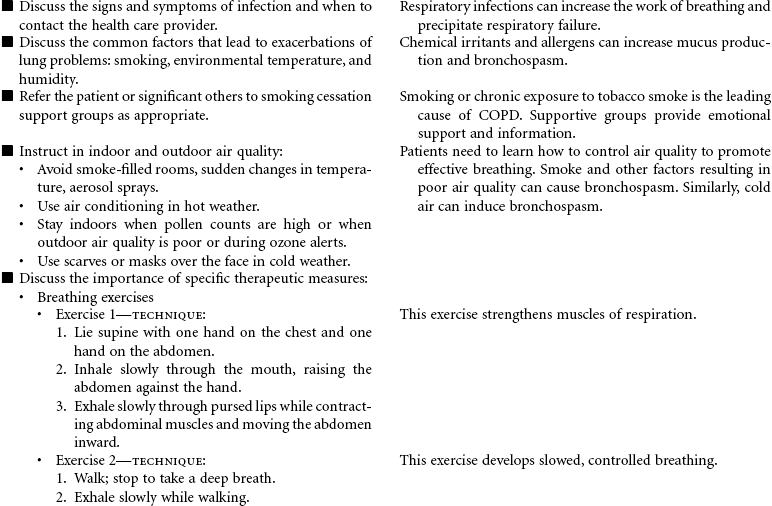
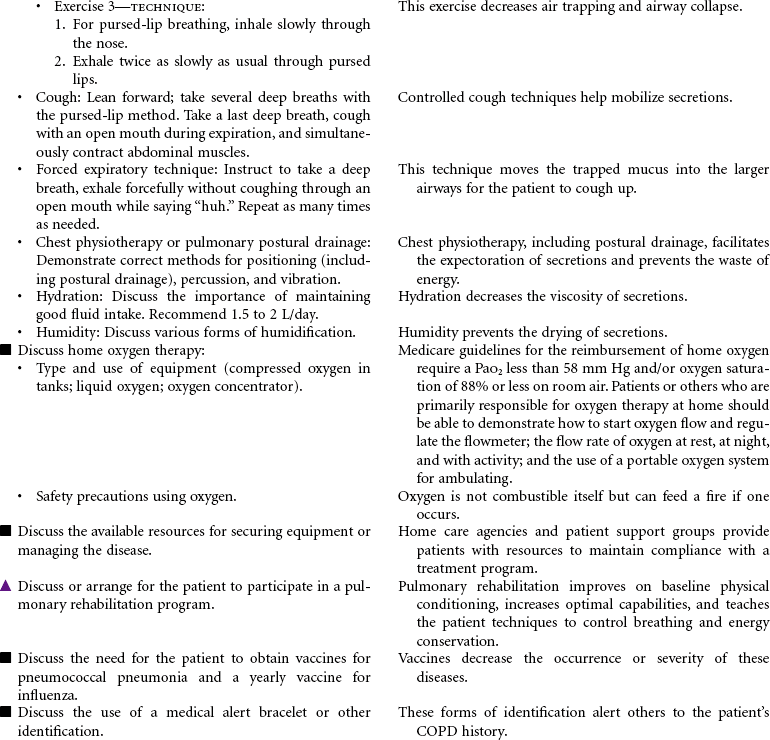
 Deficient Knowledge
Deficient Knowledge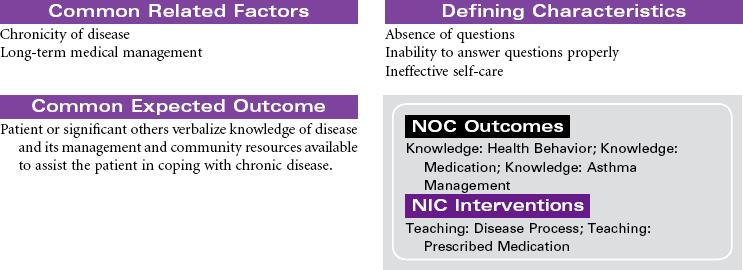
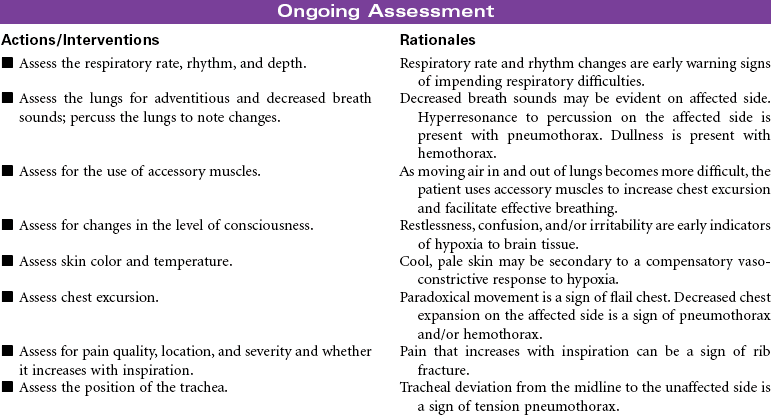
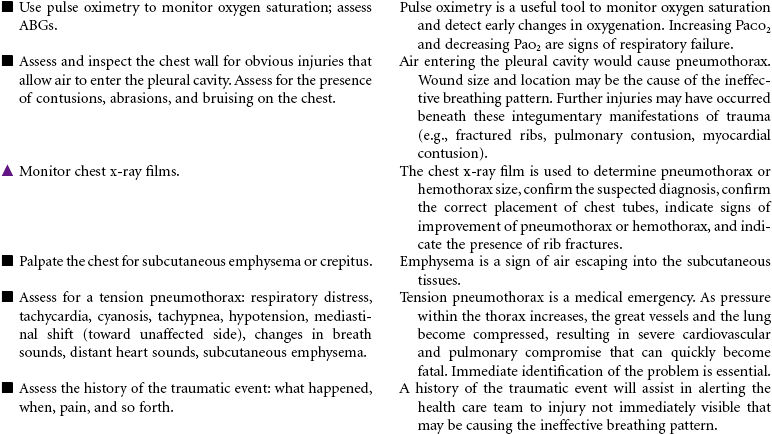
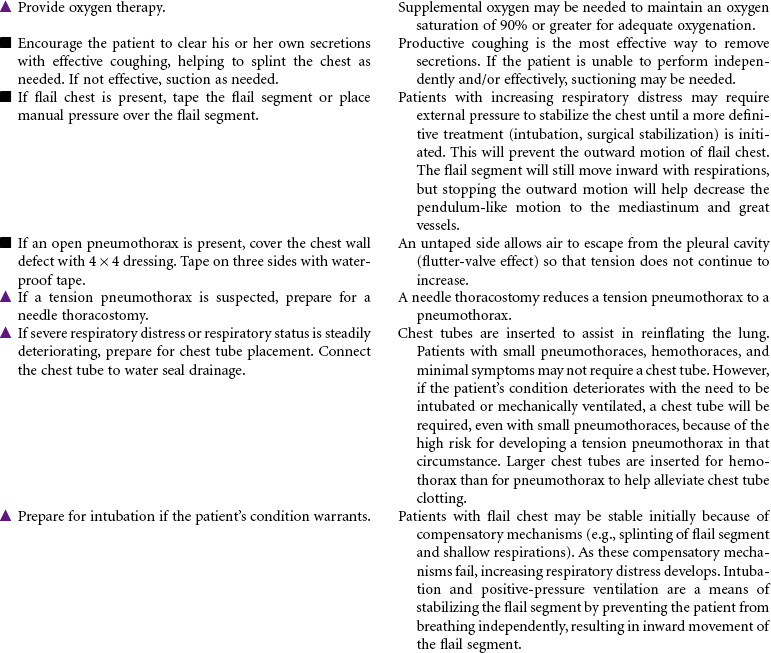
 Ineffective Breathing Pattern
Ineffective Breathing Pattern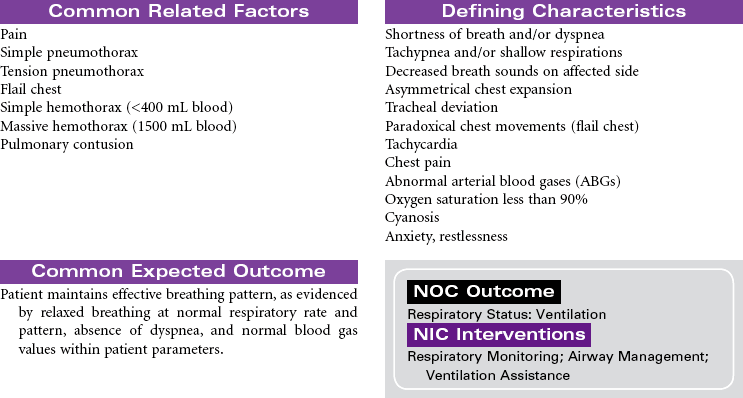

 Deficient Fluid Volume
Deficient Fluid Volume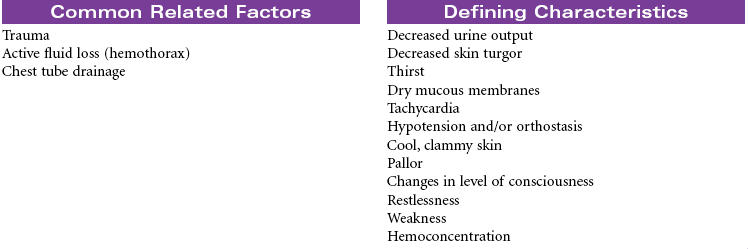
 Decreased Cardiac Output
Decreased Cardiac Output
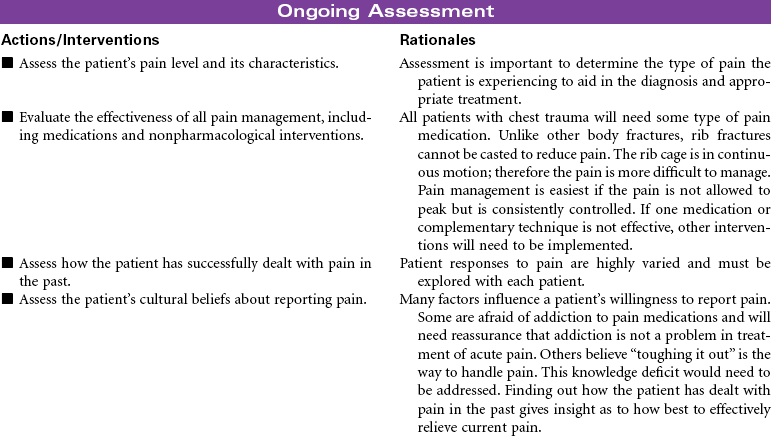
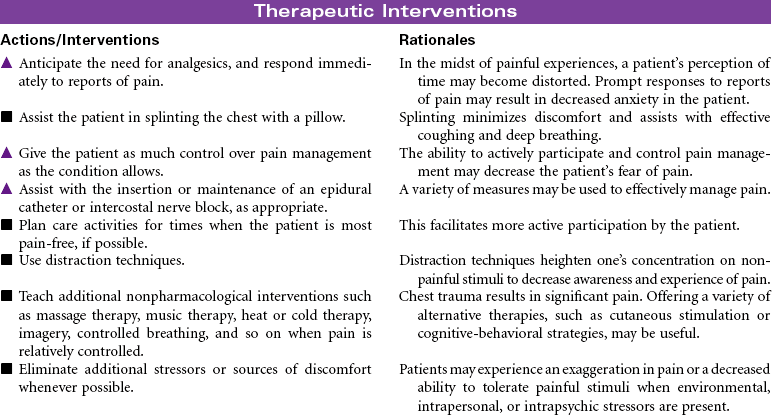
 Acute Pain
Acute Pain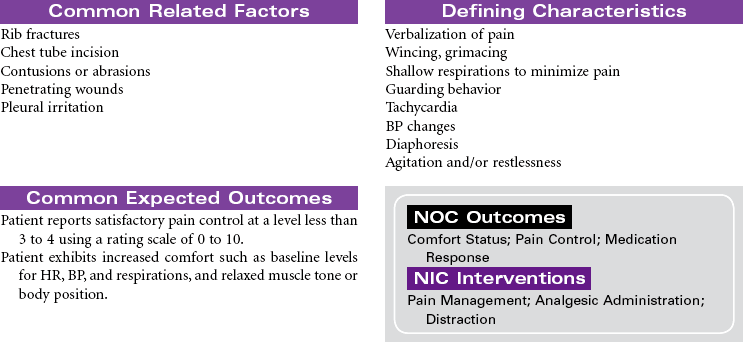
 Anxiety
Anxiety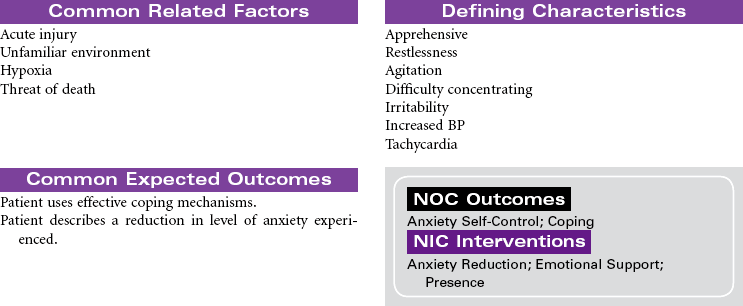
 Ineffective Airway Clearance
Ineffective Airway Clearance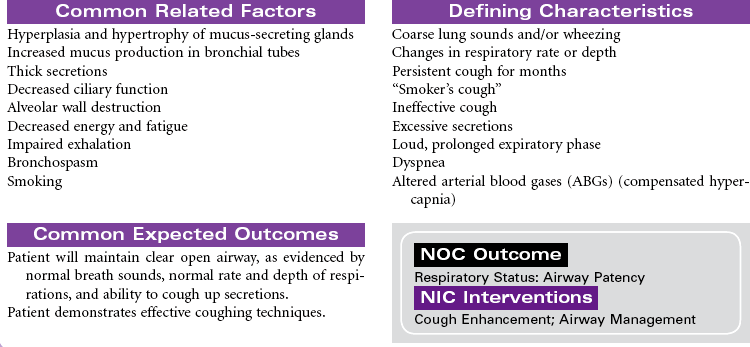
 Impaired Gas Exchange
Impaired Gas Exchange
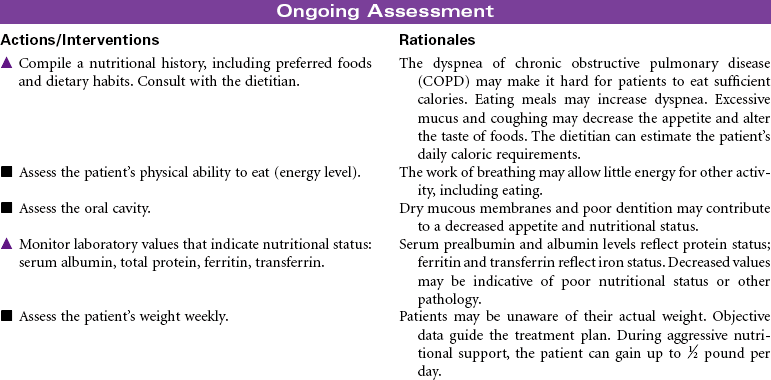
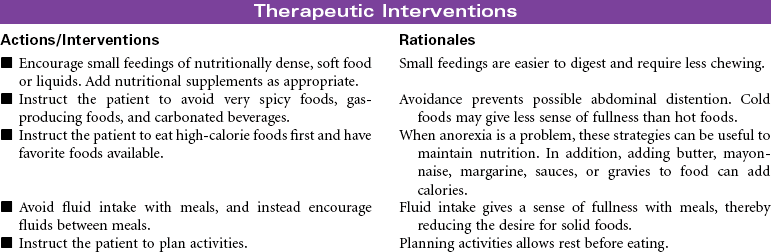
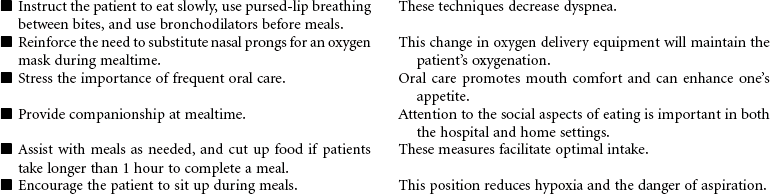
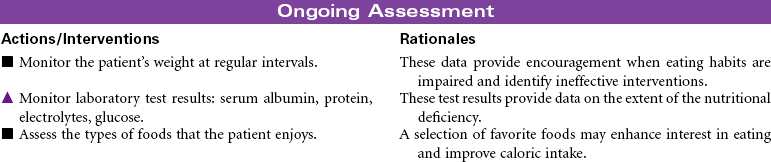
 Imbalanced Nutrition: Less Than Body Requirements
Imbalanced Nutrition: Less Than Body Requirements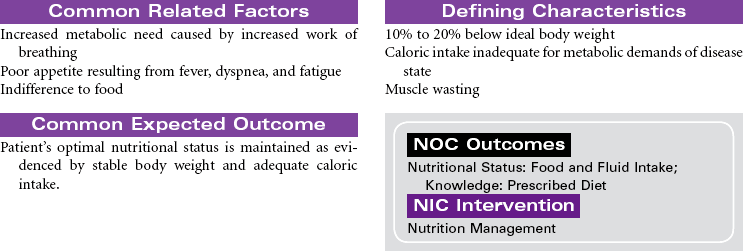
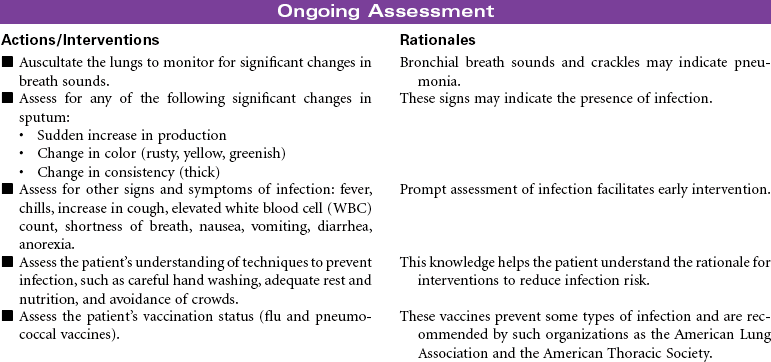
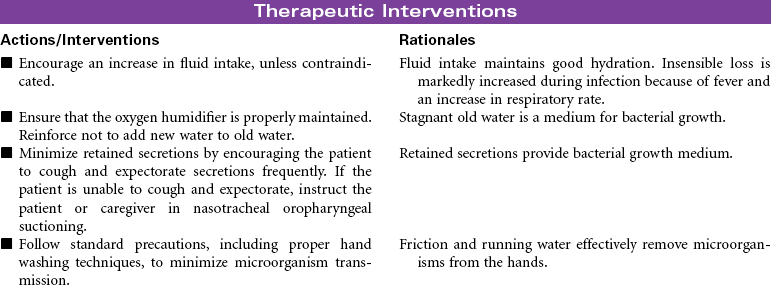
 Risk for Infection
Risk for Infection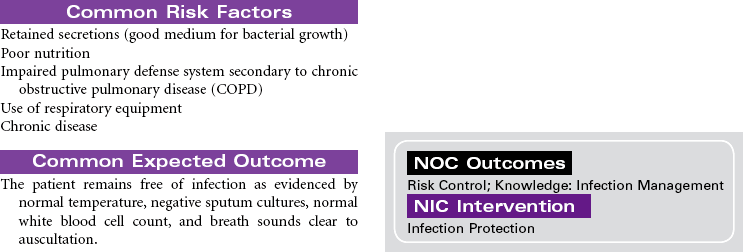
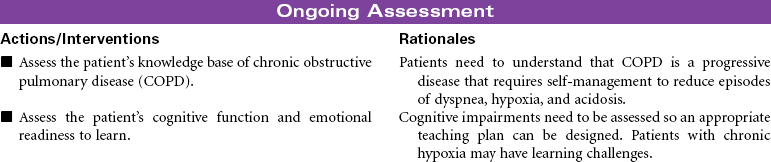
 Deficient Knowledge
Deficient Knowledge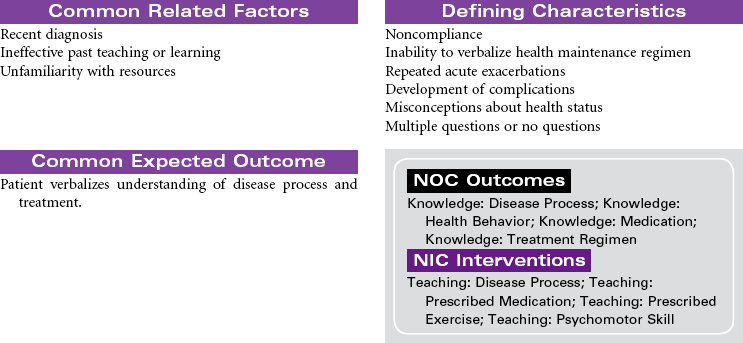
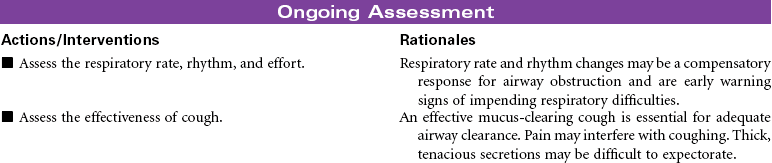
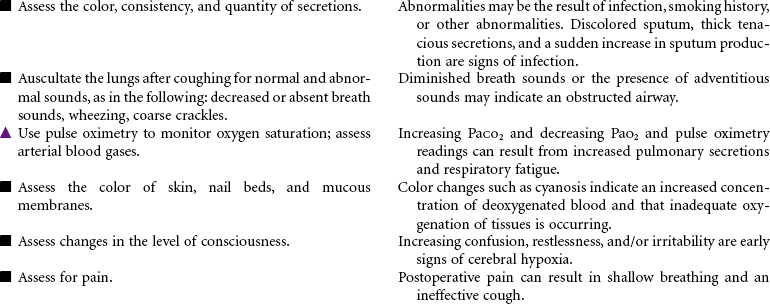
 Ineffective Airway Clearance
Ineffective Airway Clearance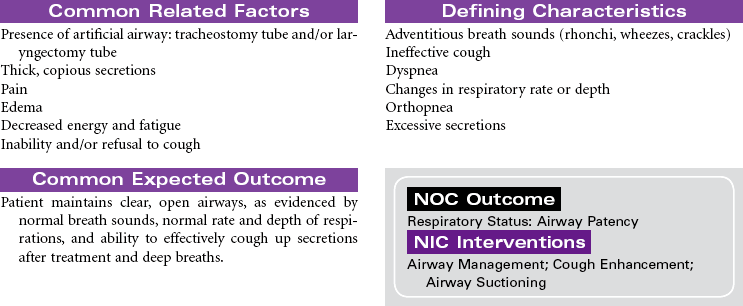
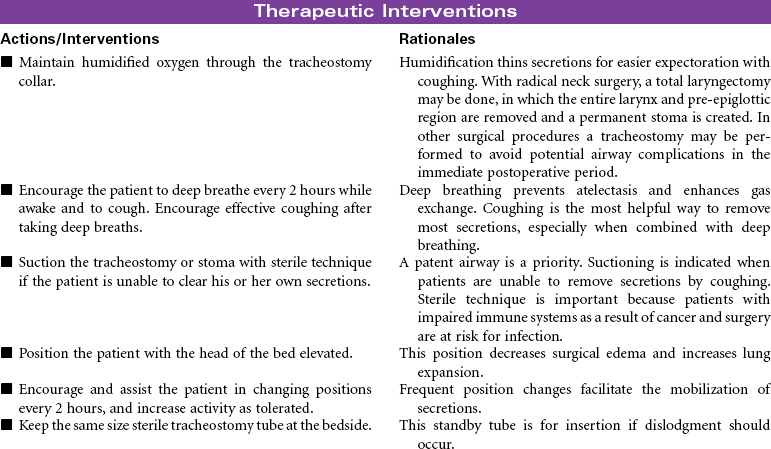
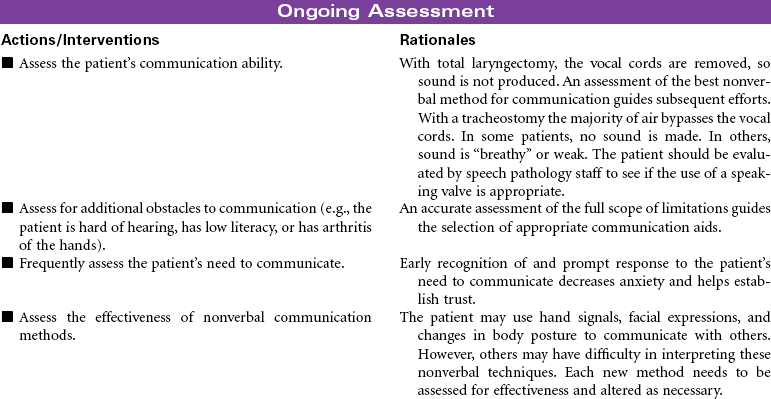
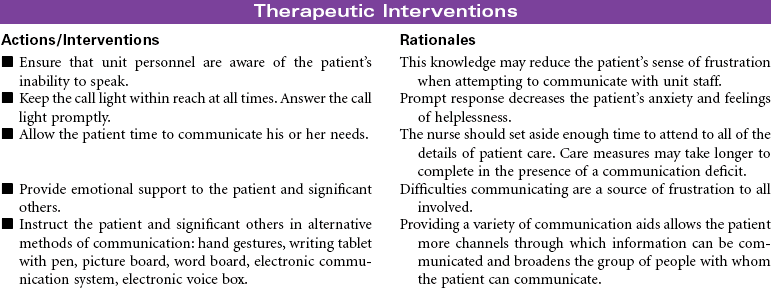
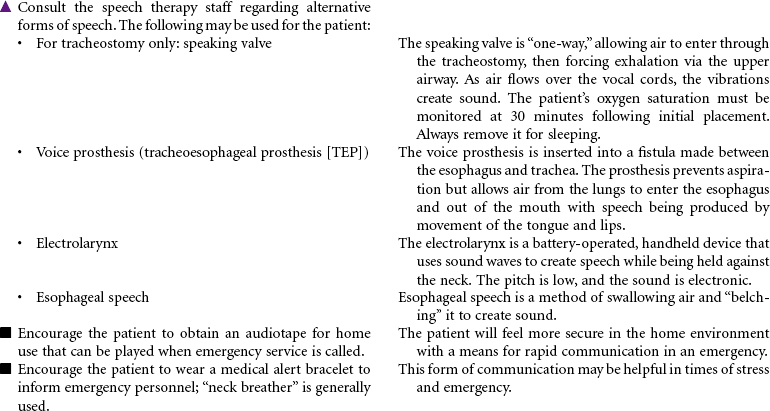
 Impaired Verbal Communication
Impaired Verbal Communication
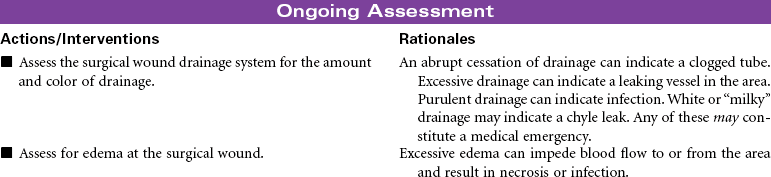
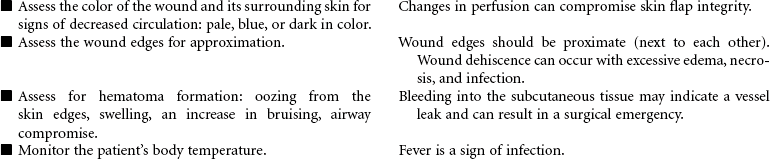
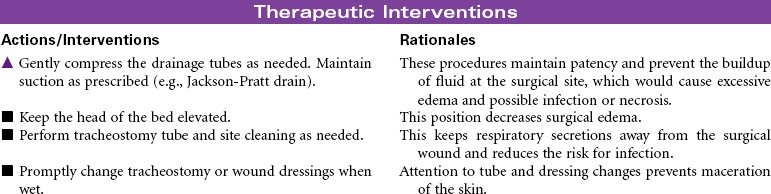
 Risk for Ineffective Tissue Perfusion
Risk for Ineffective Tissue Perfusion
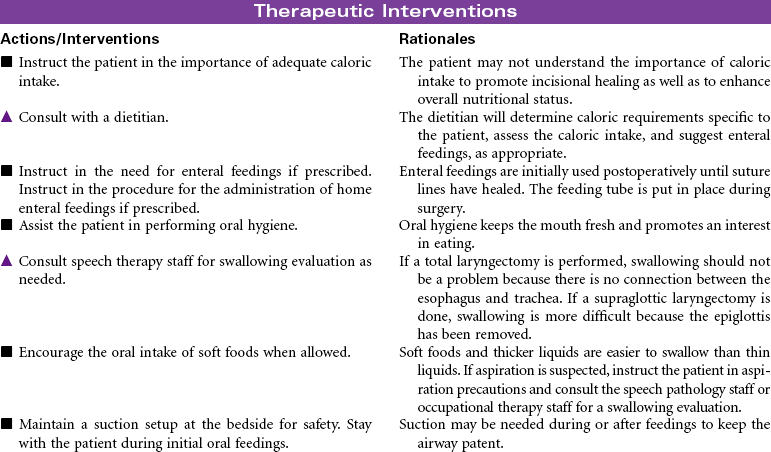
 Imbalanced Nutrition: Less Than Body Requirements
Imbalanced Nutrition: Less Than Body Requirements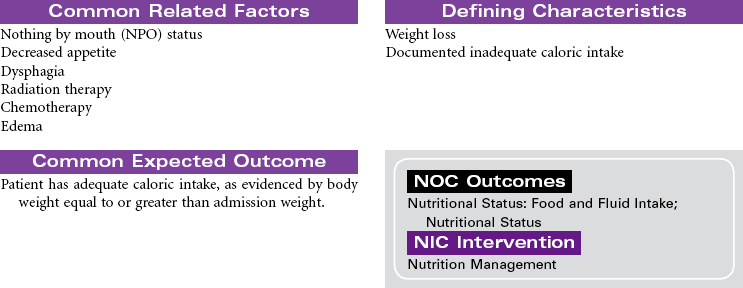

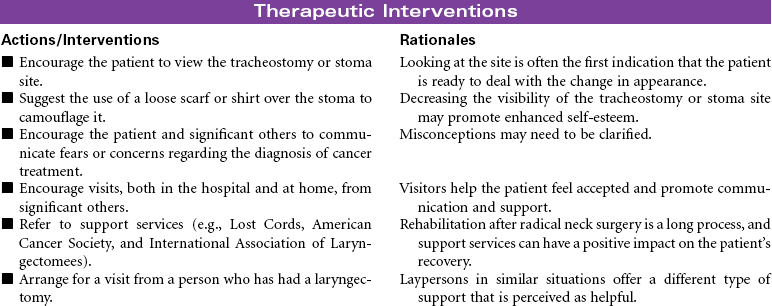
 Disturbed Body Image
Disturbed Body Image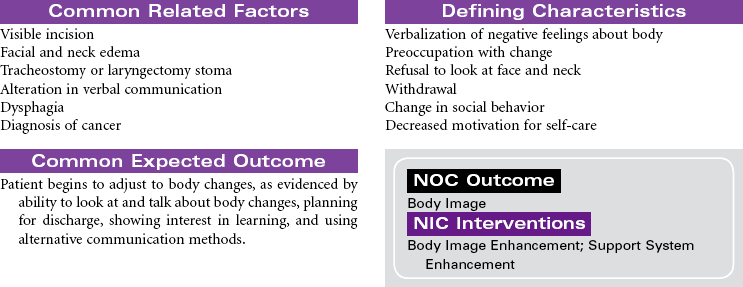

 Deficient Knowledge: Preoperative and Postoperative
Deficient Knowledge: Preoperative and Postoperative





Get Clinical Tree app for offline access
