Chapter 65 1. Compare and contrast the sequence of events leading to joint destruction in osteoarthritis and rheumatoid arthritis. 2. Detail the clinical manifestations, collaborative care, and nursing management of osteoarthritis and rheumatoid arthritis. 3. Describe the pathophysiology, clinical manifestations, and collaborative care of gout, Lyme disease, and septic arthritis. 4. Summarize the pathophysiology, clinical manifestations, collaborative care, and nursing management of ankylosing spondylitis, psoriatic arthritis, and reactive arthritis. 5. Differentiate the pathophysiology, clinical manifestations, collaborative care, and nursing management of systemic lupus erythematosus, scleroderma, polymyositis, dermatomyositis, and Sjögren’s syndrome. 6. Explain the drug therapy and related nursing management associated with arthritis and connective tissue diseases. 7. Compare and contrast the possible etiologies, clinical manifestations, and collaborative and nursing management of fibromyalgia and chronic fatigue syndrome. 1. Performs prescribed joint exercises to maintain and improve joint function 2. Uses joint protection measures to prevent increased joint inflammation 3. Performs activities of daily living to the maximum amount possible 1. Participates in planning and carrying out therapeutic regimen 2. Expresses confidence in ability to make treatment decisions 1. Maintains skin integrity with the use of topical treatments 2. Prevents exacerbations with the use of sunscreens and limited sun exposure 1. Describes the disease process and the rationale for prescribed treatment 2. Expresses confidence in ability to recognize complications and use precautions to prevent their occurrence This chapter discusses rheumatic diseases, which primarily affect body joints, tendons, ligaments, muscles, and bones. These diseases are often characterized by inflammation. Rheumatic diseases result from the loss of function in one or more of the connective or bone structures of the body. There are more than 100 kinds of rheumatic diseases. An estimated 46 million people in the United States have rheumatic conditions.1 Arthritis, a type of rheumatic disease, involves inflammation of a joint or joints. Most forms of arthritis affect women more frequently than men.2 The most common types of arthritis are osteoarthritis, rheumatoid arthritis, and gout. Osteoarthritis (OA), the most common form of joint (articular) disease in North America, is a slowly progressive noninflammatory disorder of the diarthrodial (synovial) joints. Currently 27 million Americans are affected by OA, with the numbers expected to greatly increase as the population ages.1 OA involves the formation of new joint tissue in response to cartilage destruction.3 OA is not considered a normal part of the aging process, but aging is one risk factor for disease development.4 Cartilage destruction may actually begin between ages 20 and 30, and the majority of adults are affected by age 40. Few patients experience symptoms until after age 50 or 60, but more than half of those over 65 years of age have x-ray evidence of OA in at least one joint. After 55 years of age, women are affected by OA more often than men.5 OA is usually caused by a known event or condition that directly damages cartilage or causes joint instability (Table 65-1). The increased incidence of OA in aging women is believed to be due to estrogen reduction at menopause. Modifiable risk factors for OA have been identified, including obesity, which contributes to hip and knee OA. Regular moderate exercise, which also helps with weight control, has been shown to decrease the likelihood of disease development and progression. Anterior cruciate ligament injury, which is associated with quick stops and pivoting as in football and soccer, has been linked to an increased risk of knee OA.6 Occupations that require frequent kneeling and stooping are also linked to a higher risk of knee OA. TABLE 65-1
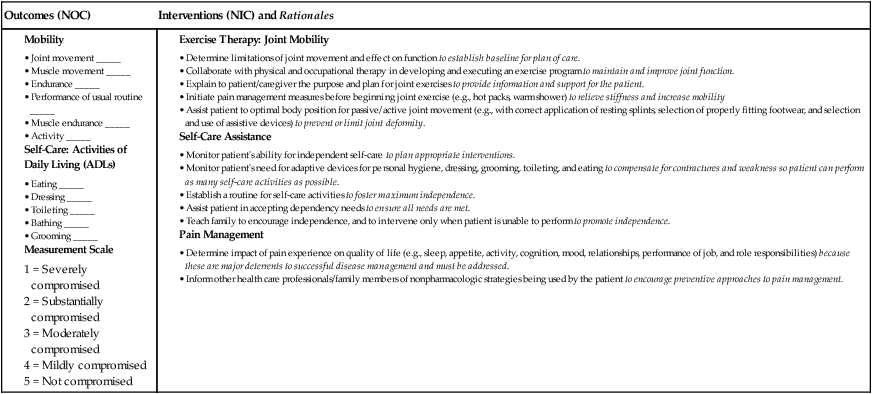
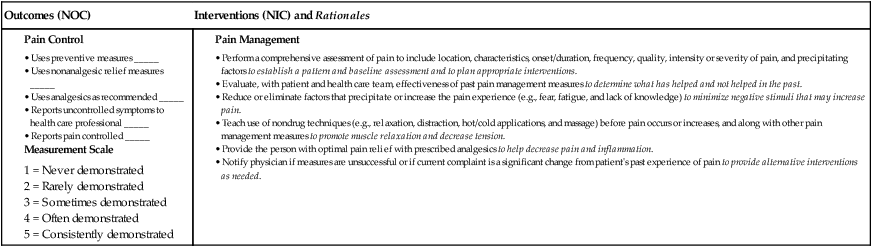
Nursing Management
Arthritis and Connective Tissue Diseases
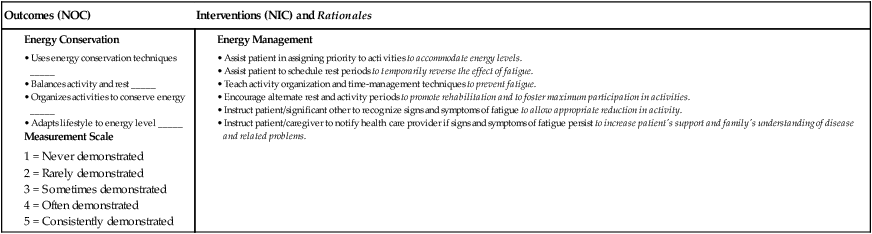
 eNursing Care Plan 65-1 Patient With Rheumatoid Arthritis
eNursing Care Plan 65-1 Patient With Rheumatoid Arthritis
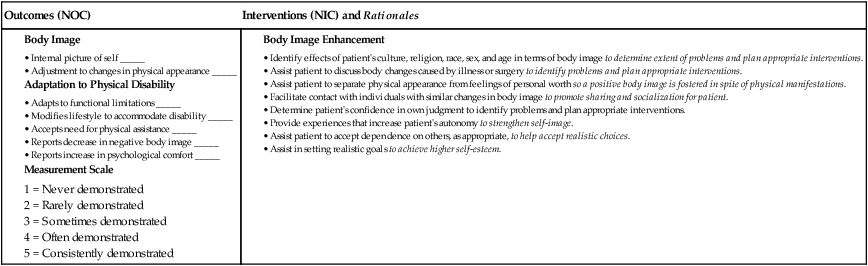
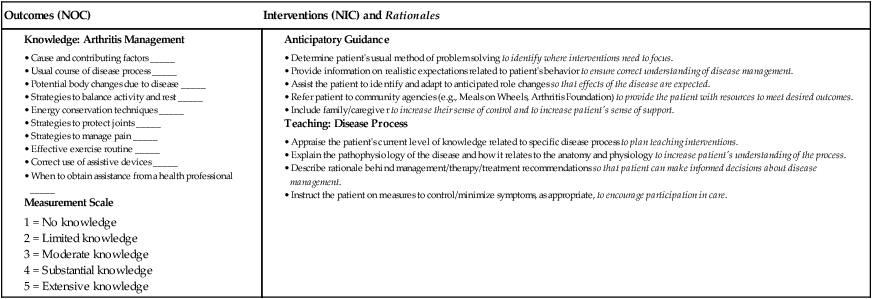
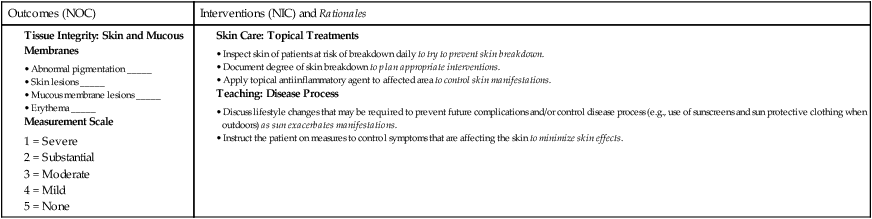
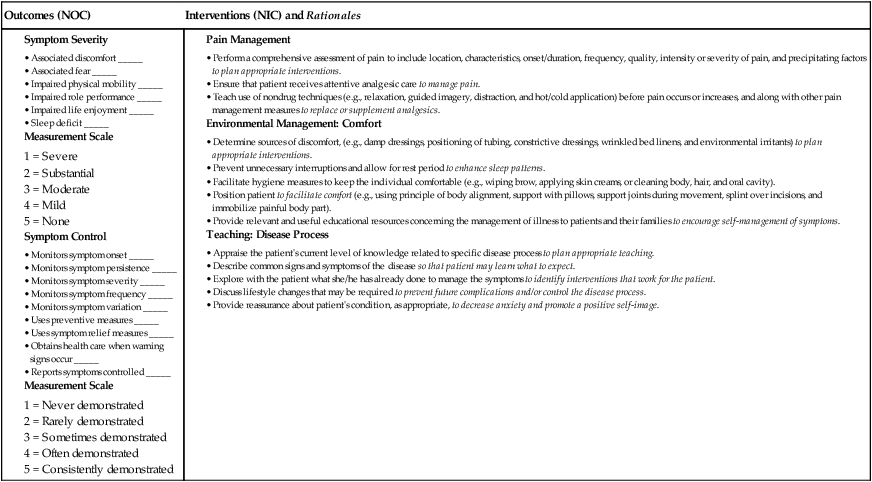
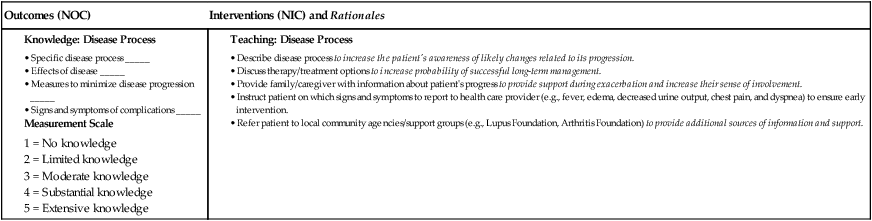
 eNursing Care Plan 65-2 Patient With Systemic Lupus Erythematosus
eNursing Care Plan 65-2 Patient With Systemic Lupus Erythematosus
Arthritis
Osteoarthritis
Etiology and Pathophysiology
Cause
Effects on Joint Cartilage
Trauma
Dislocations or fractures may lead to avascular necrosis or uneven stress on cartilage.
Mechanical stress
Repetitive physical activities (e.g., sports) cause cartilage deterioration.
Inflammation
Release of enzymes in response to local inflammation can affect cartilage integrity.
Joint instability
Damage to supporting structures causes instability, placing uneven stress on articular cartilage.
Neurologic disorders
Pain and loss of reflexes from neurologic disorders, such as diabetic neuropathy and Charcot’s joint, cause abnormal movements that contribute to cartilage deterioration.
Skeletal deformities
Congenital or acquired conditions such as Legg-Calvé-Perthes disease or dislocated hip contribute to cartilage deterioration.
Hematologic or endocrine disorders
Chronic hemarthrosis (e.g., hemophilia) contributes to cartilage deterioration.
Drugs
Drugs such as indomethacin (Indocin), colchicine, and corticosteroids can stimulate collagen-digesting enzymes in joint synovium. ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Nursing Management: Arthritis and Connective Tissue Diseases
Get Clinical Tree app for offline access
