Chapter 7 Multi-infarct Dementia (MID); Dementia of the Alzheimer Type (DAT) Lou Gehrig’s Disease; Motor Neuron Disease; Progressive Bulbar Palsy; Progressive Muscular Atrophy
Neurological Care Plans
Alzheimer’s Disease/Dementia
 For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
Amyotrophic Lateral Sclerosis
Neurological Care Plans
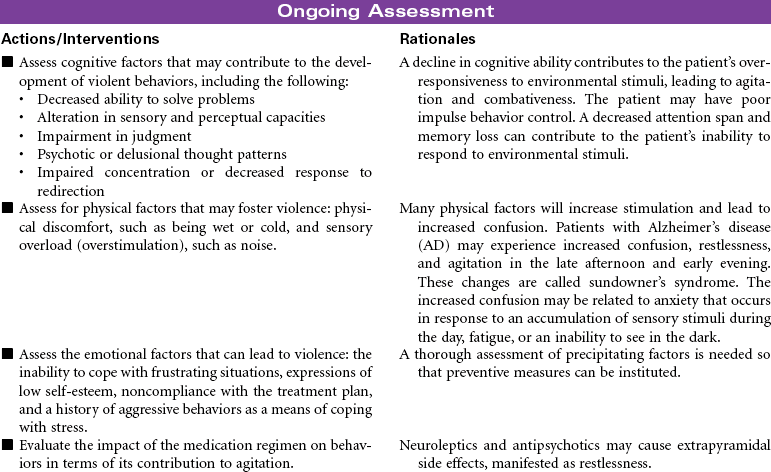
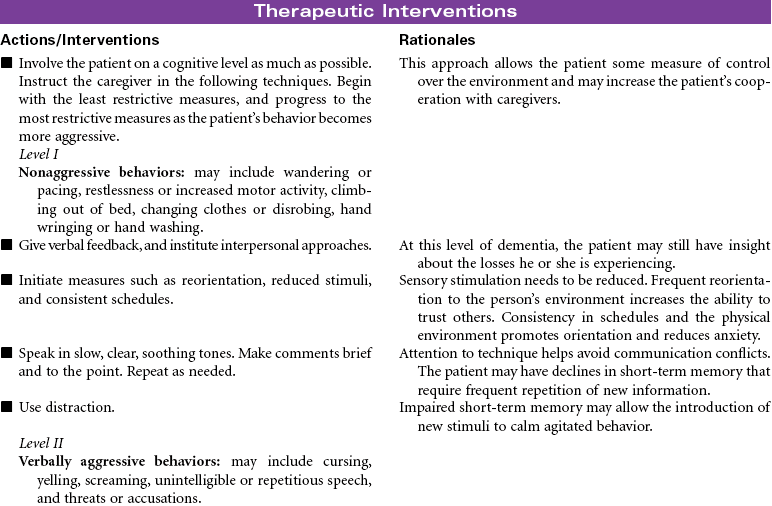
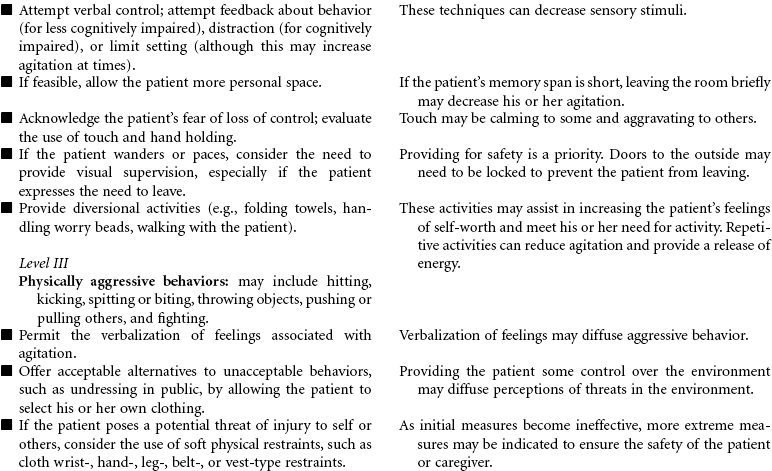
 Risk for Violence: Self-Directed or Other-Directed
Risk for Violence: Self-Directed or Other-Directed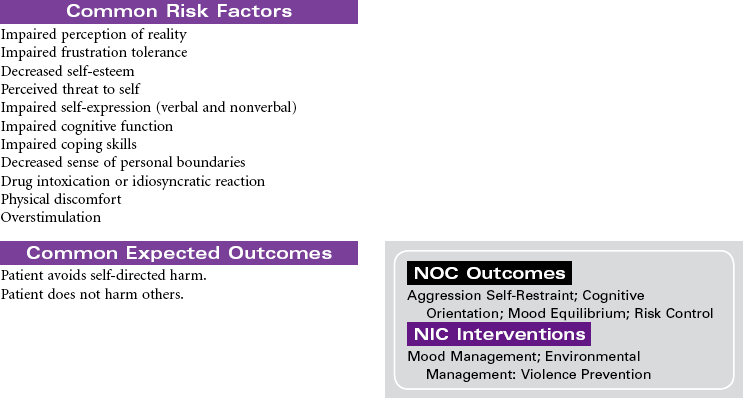

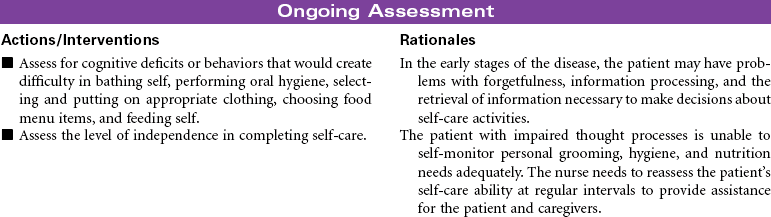
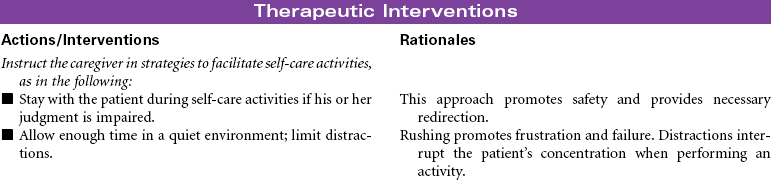
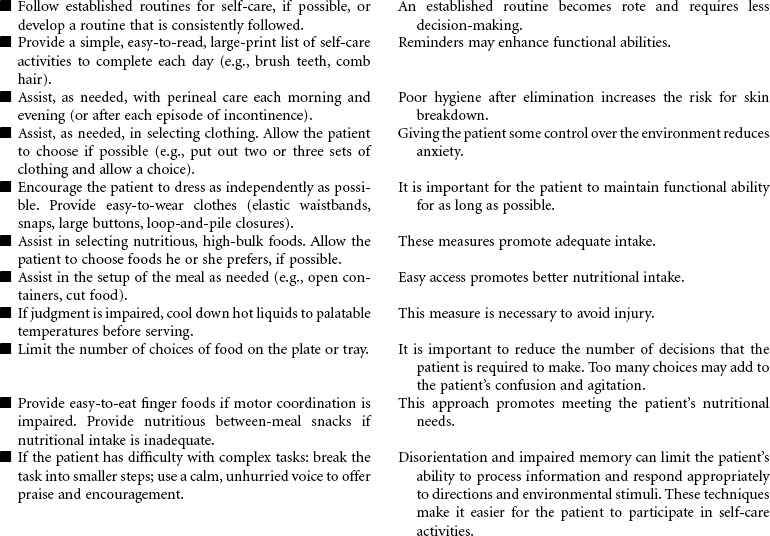
 Self-Care Deficit: Bathing, Dressing, Feeding
Self-Care Deficit: Bathing, Dressing, Feeding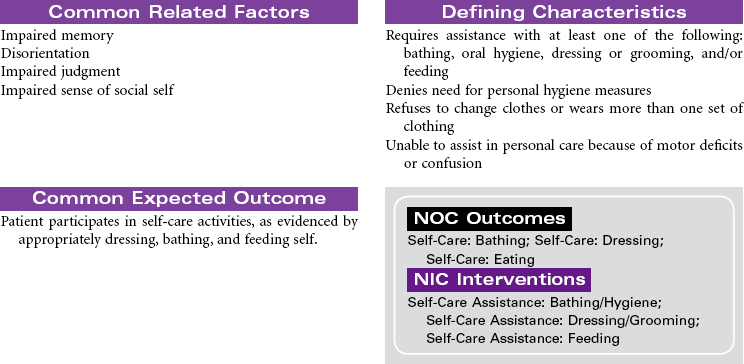
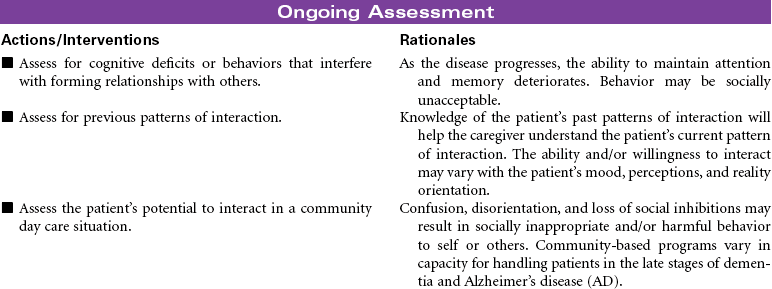
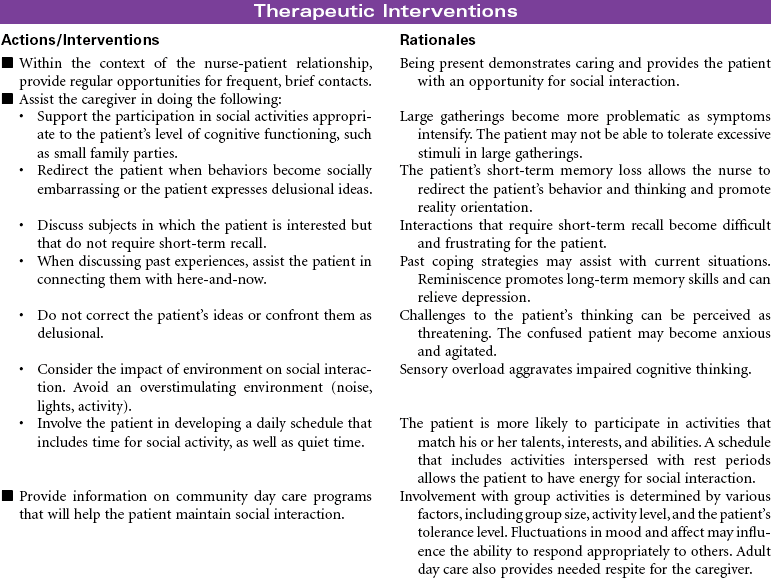
 Impaired Social Interaction
Impaired Social Interaction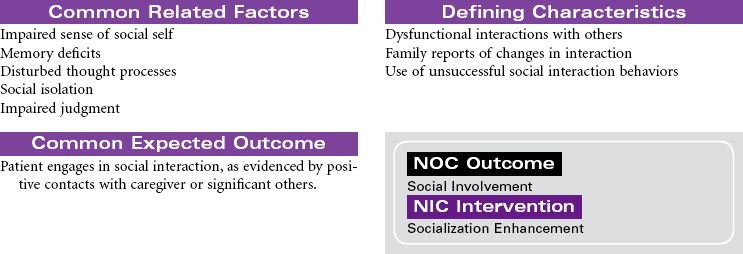
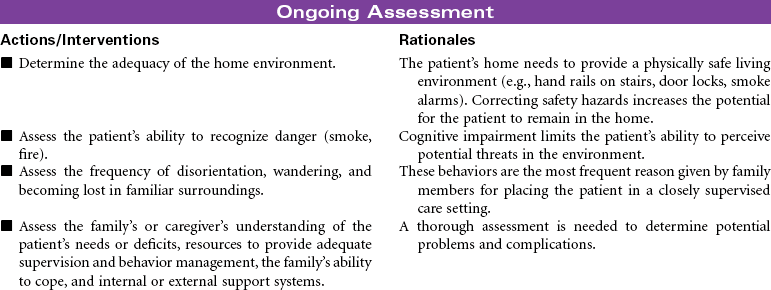
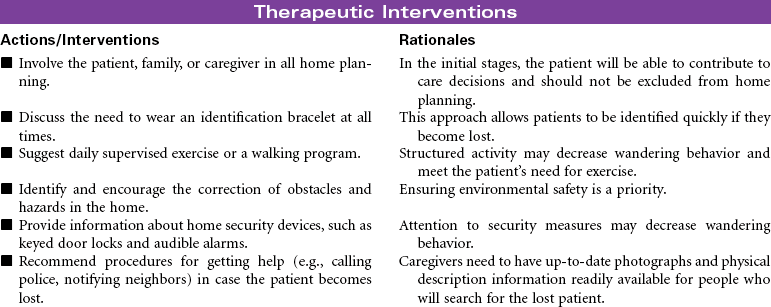
 Impaired Home Maintenance
Impaired Home Maintenance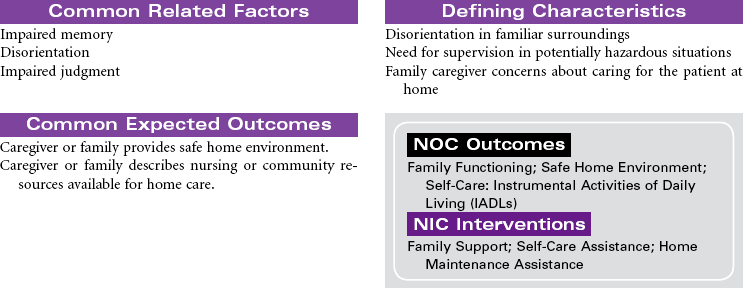

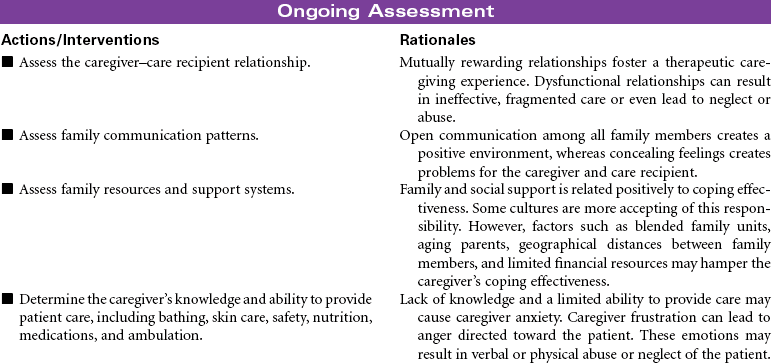
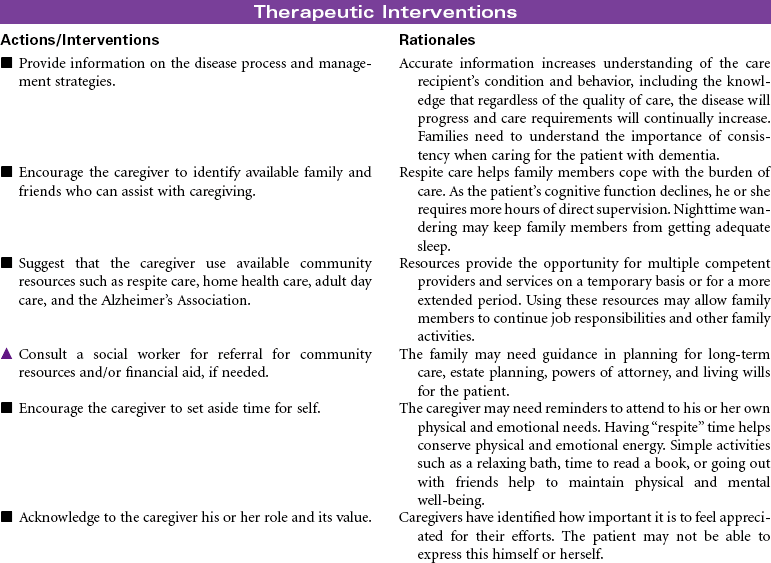
 Caregiver Role Strain
Caregiver Role Strain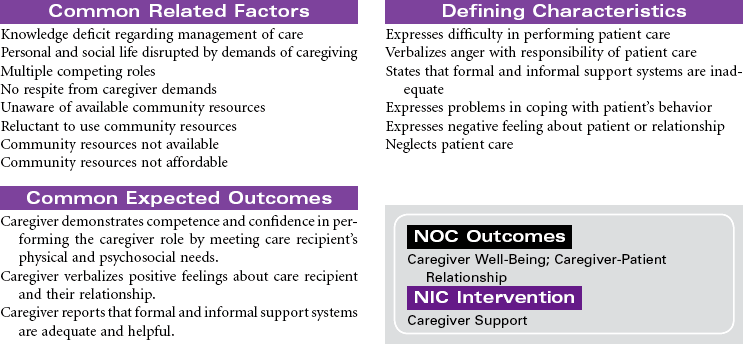
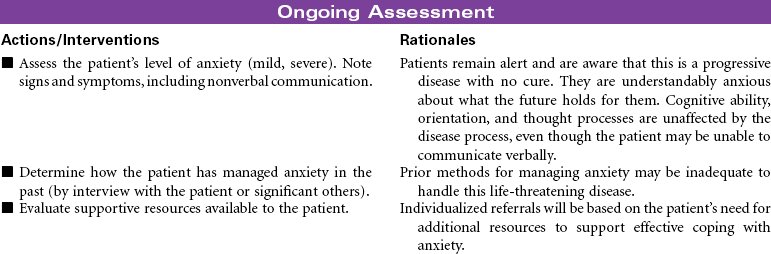
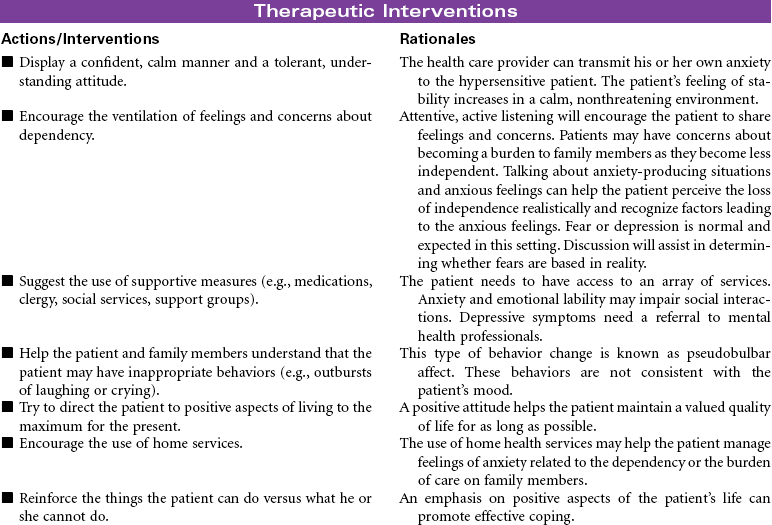
 Anxiety
Anxiety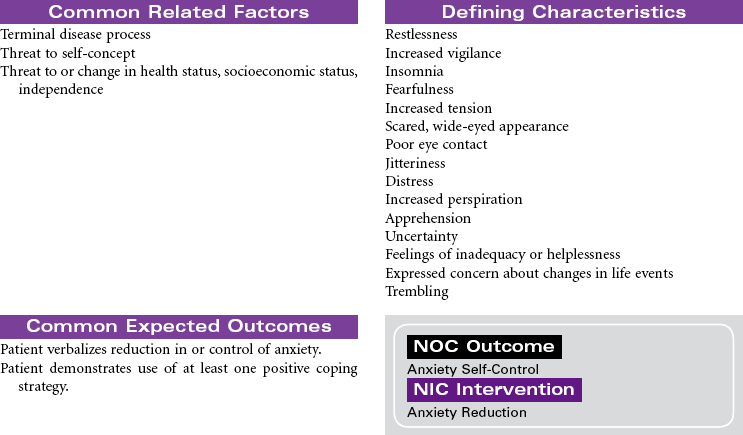
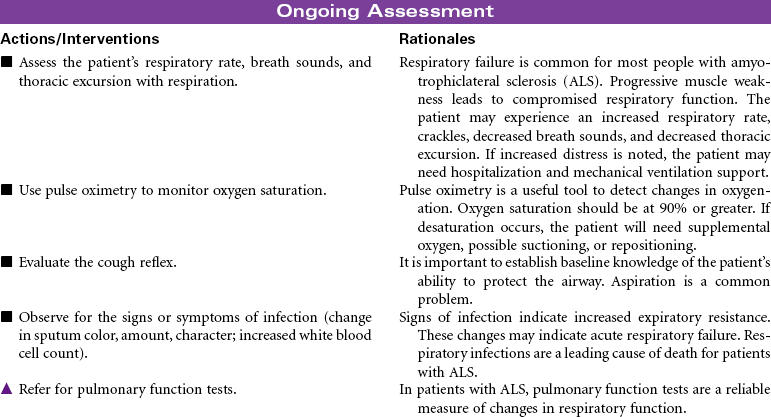
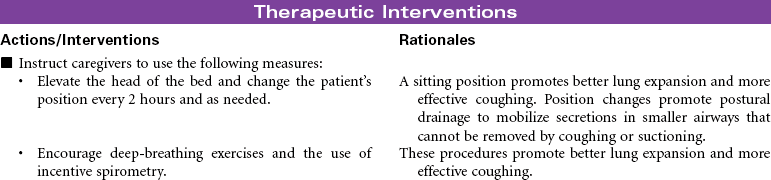
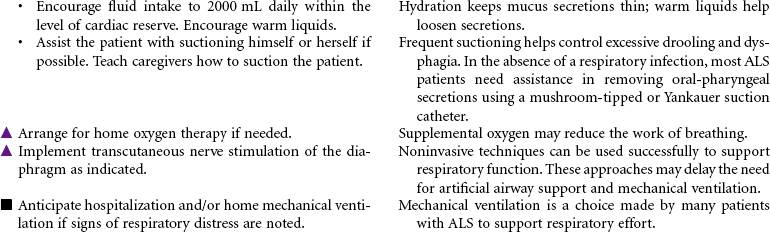
 Ineffective Airway Clearance
Ineffective Airway Clearance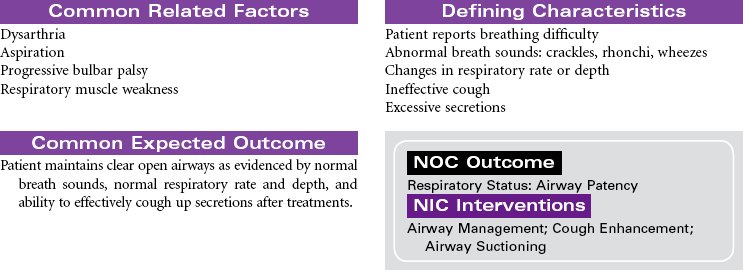
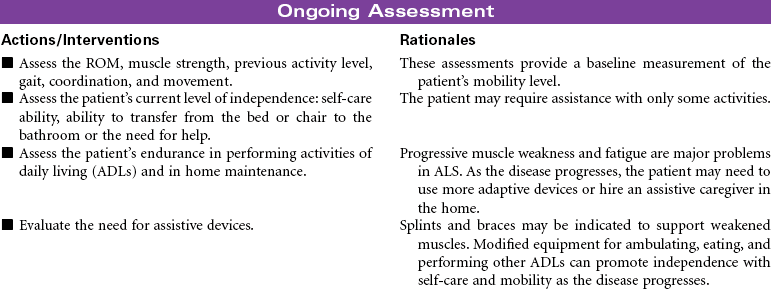
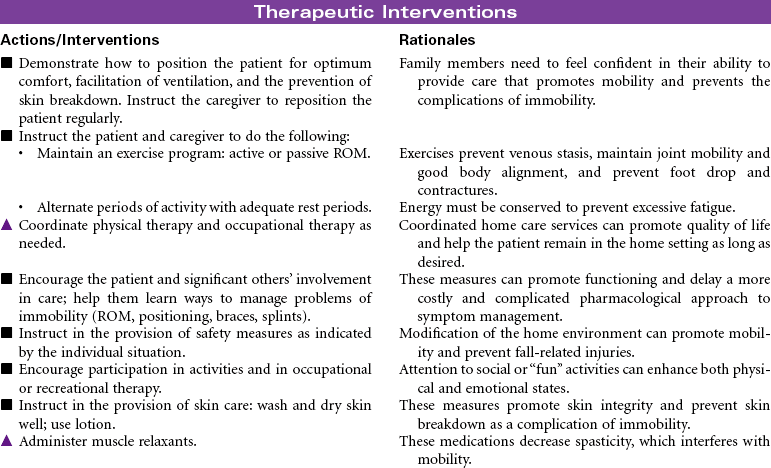
 Impaired Physical Mobility
Impaired Physical Mobility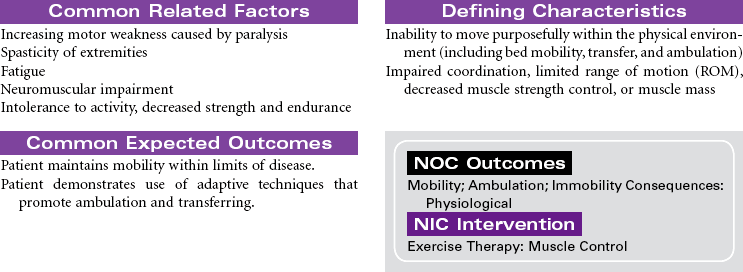
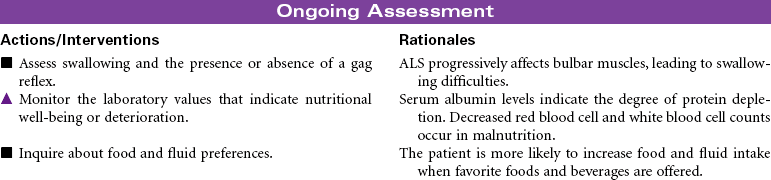
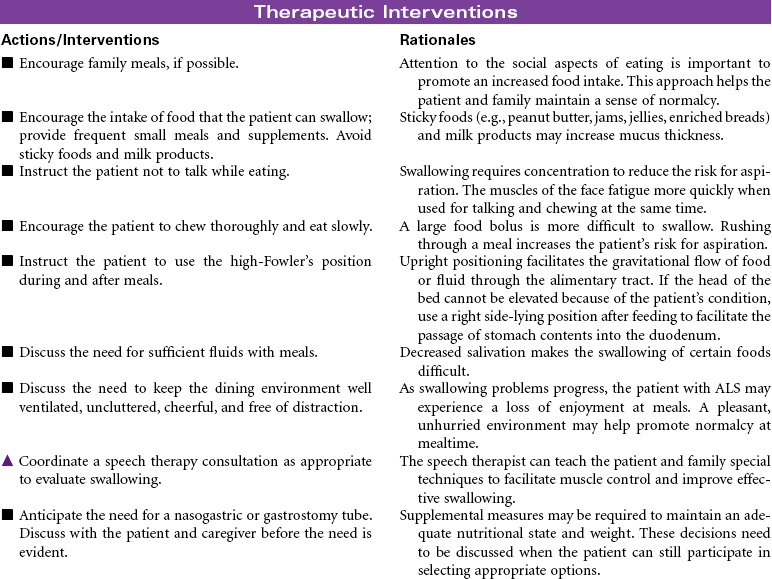
 Imbalanced Nutrition: Less Than Body Requirements
Imbalanced Nutrition: Less Than Body Requirements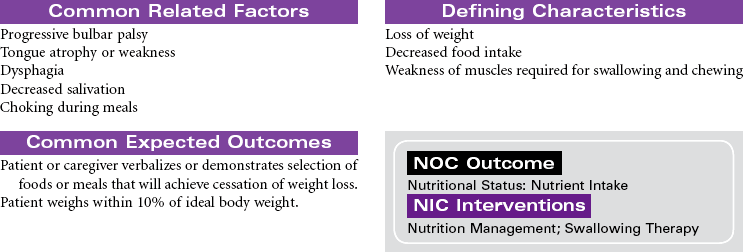

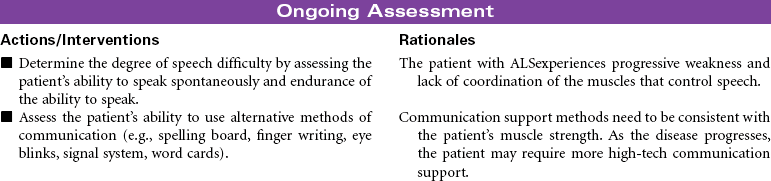
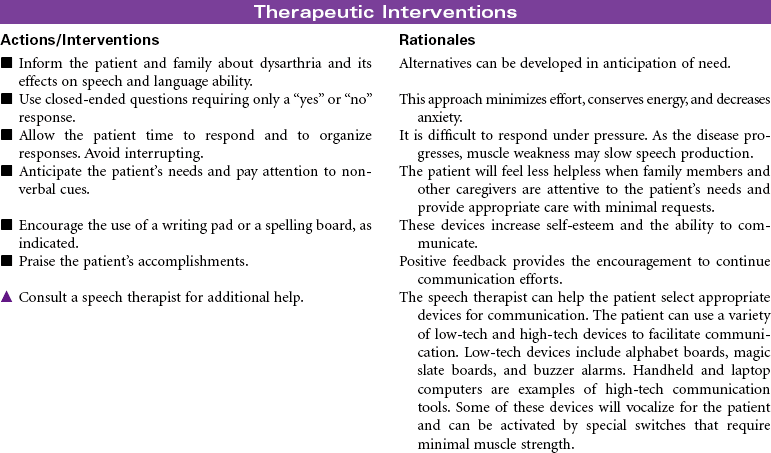
 Impaired Verbal Communication
Impaired Verbal Communication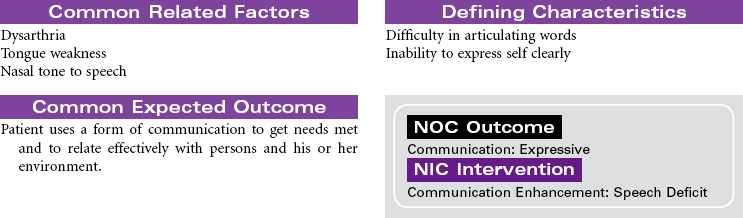
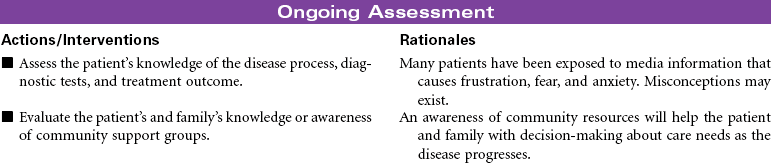
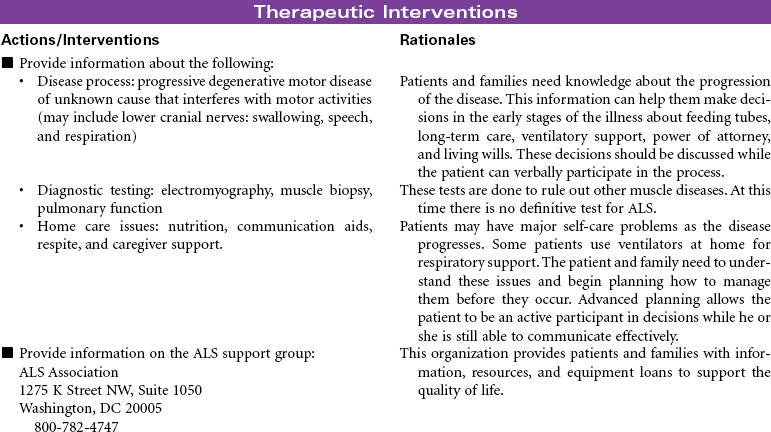
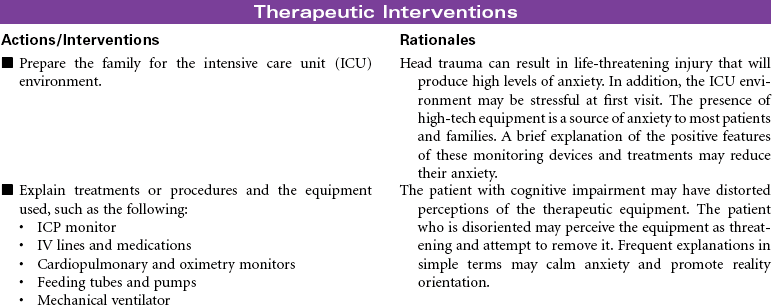
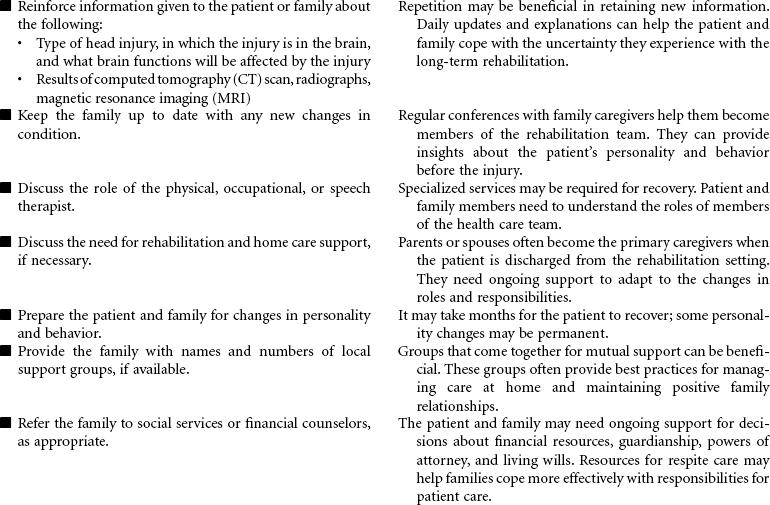
 Deficient Knowledge
Deficient Knowledge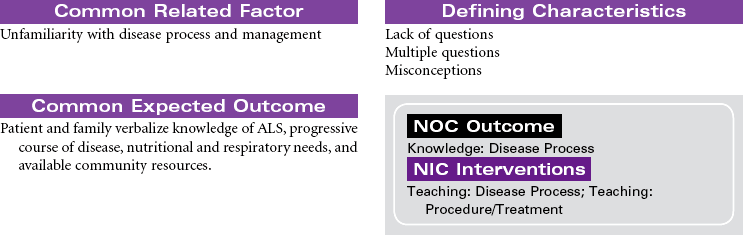
 = Independent
= Independent  = Collaborative
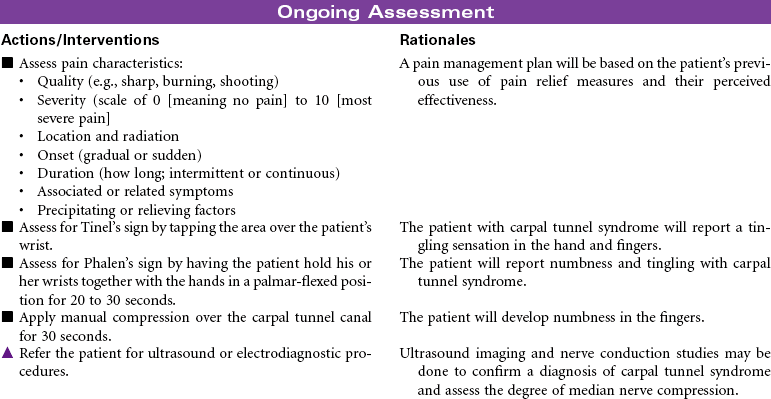
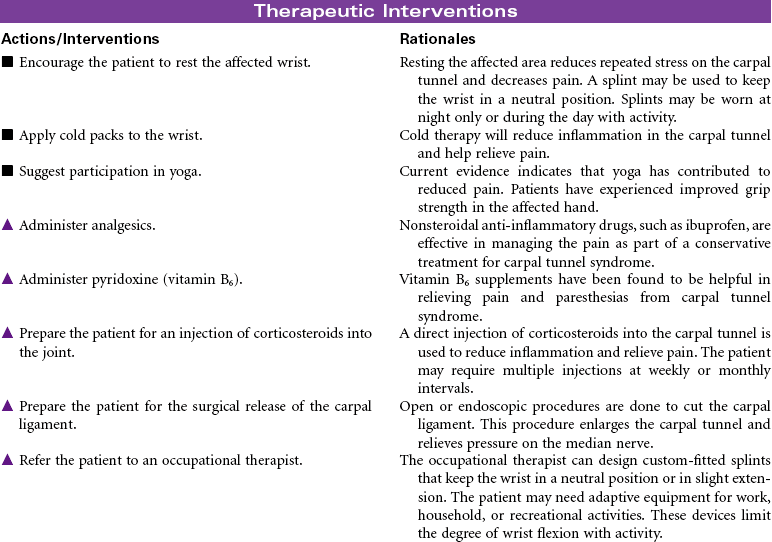
= Collaborative Acute Pain
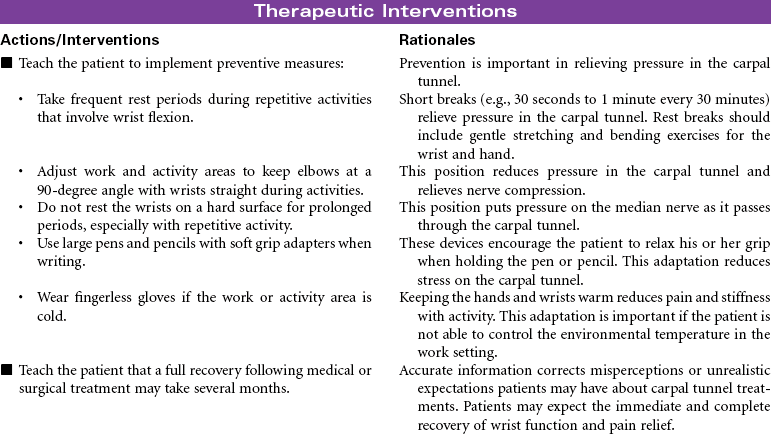
Acute Pain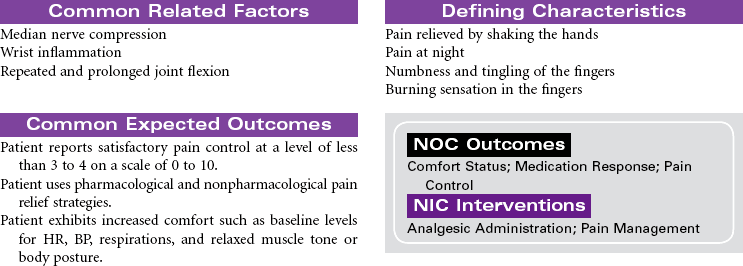
 Deficient Knowledge
Deficient Knowledge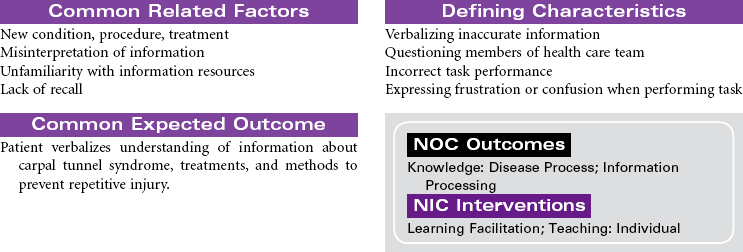

 = Independent
= Independent  = Collaborative
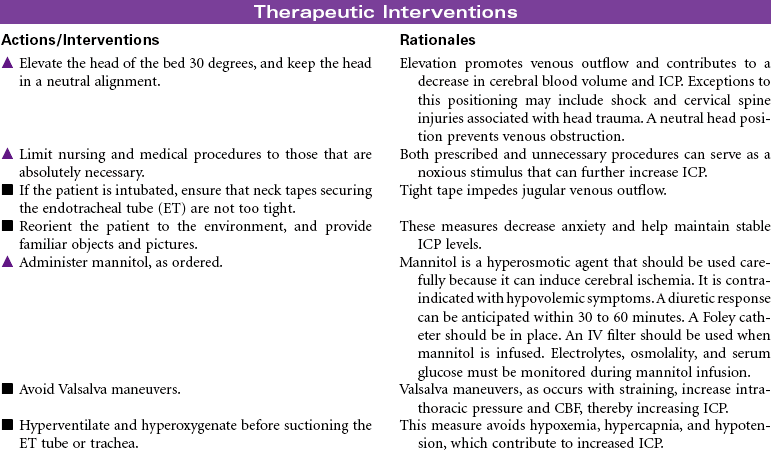
= Collaborative Decreased Intracranial Adaptive Capacity
Decreased Intracranial Adaptive Capacity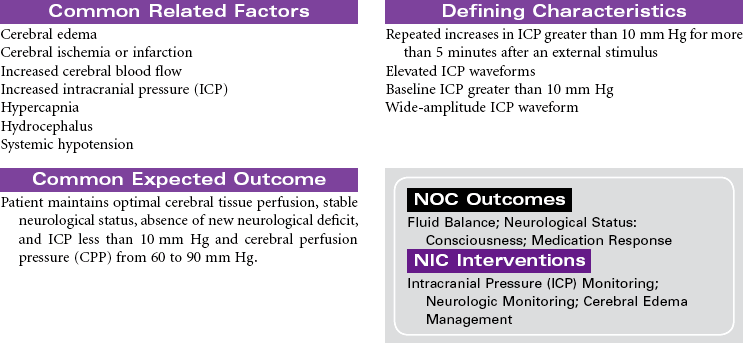
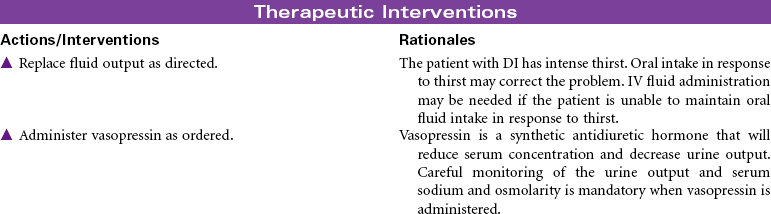
 Risk for Deficient Fluid Volume
Risk for Deficient Fluid Volume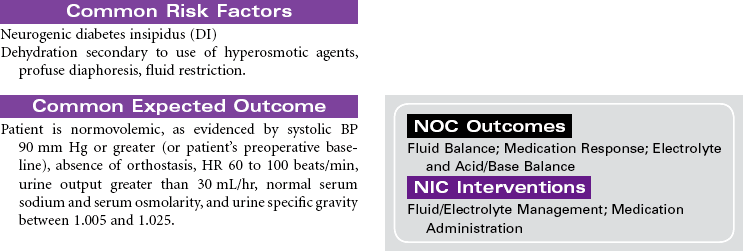
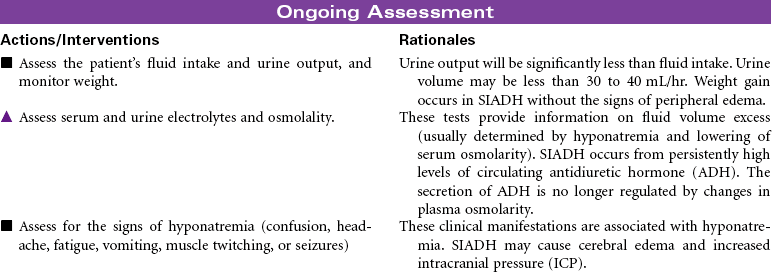
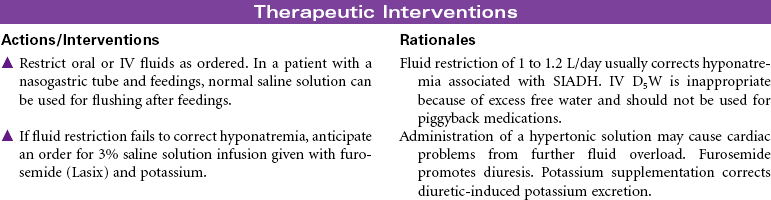
 Risk for Excess Fluid Volume
Risk for Excess Fluid Volume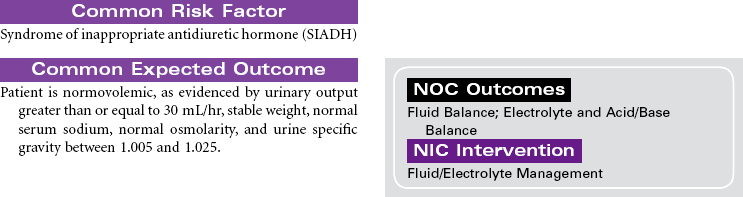
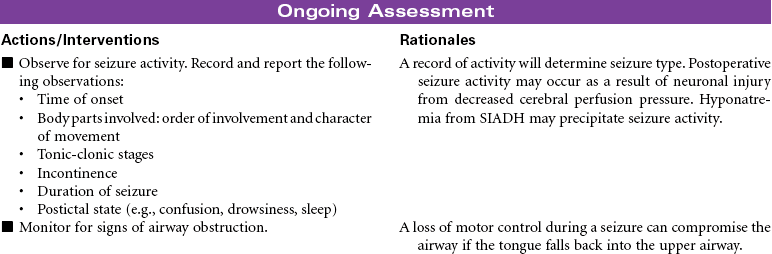
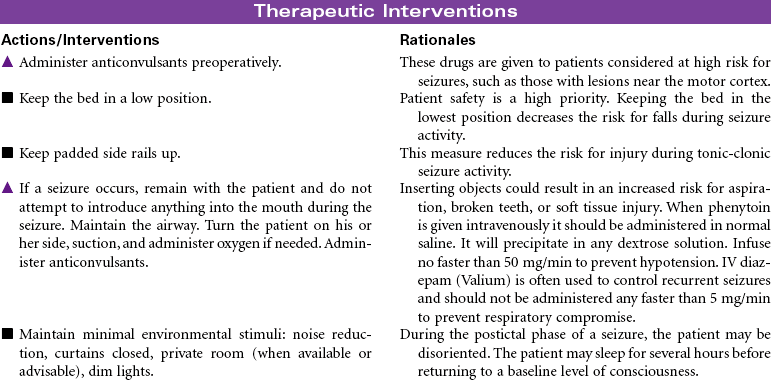
 Risk for Seizures
Risk for Seizures

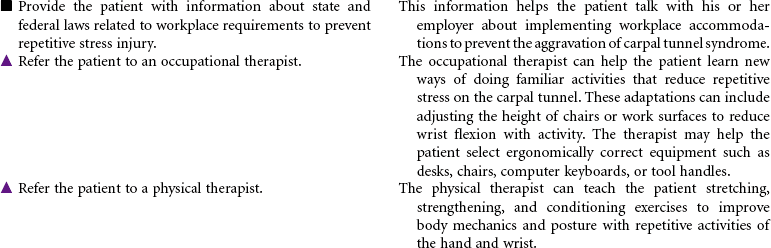
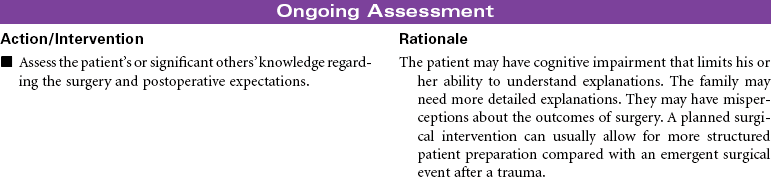
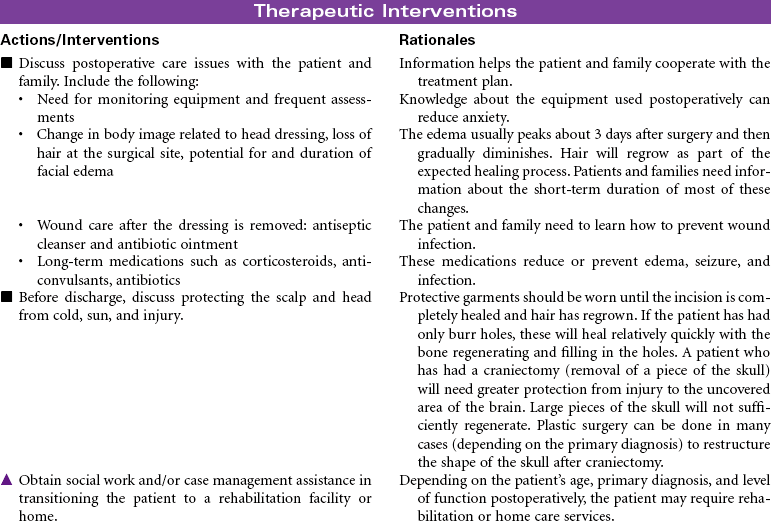
 Deficient Knowledge
Deficient Knowledge



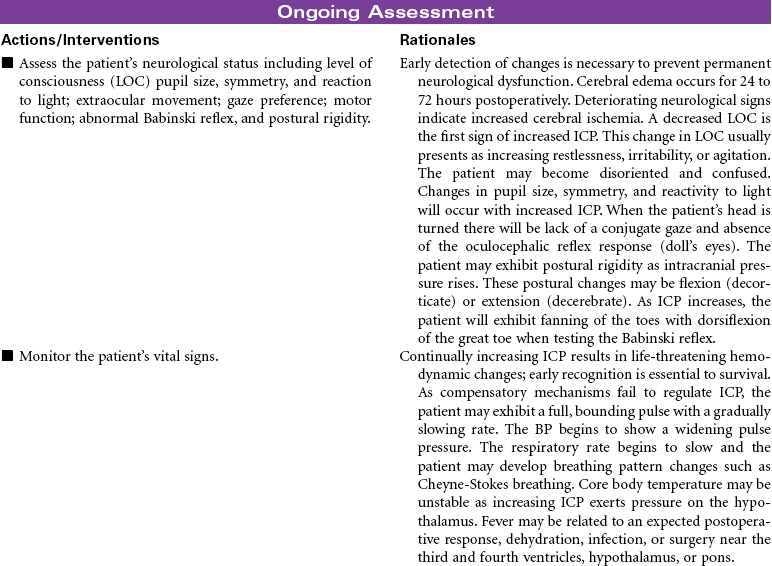
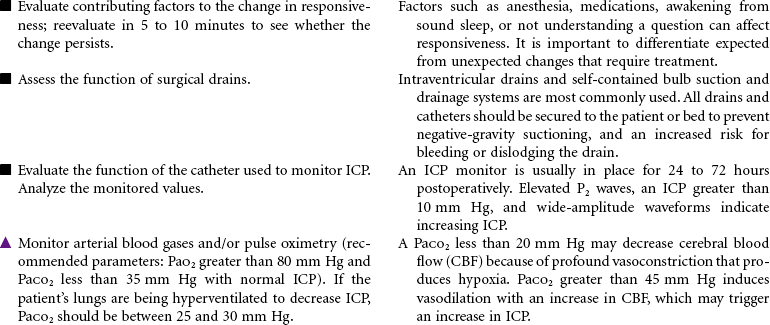
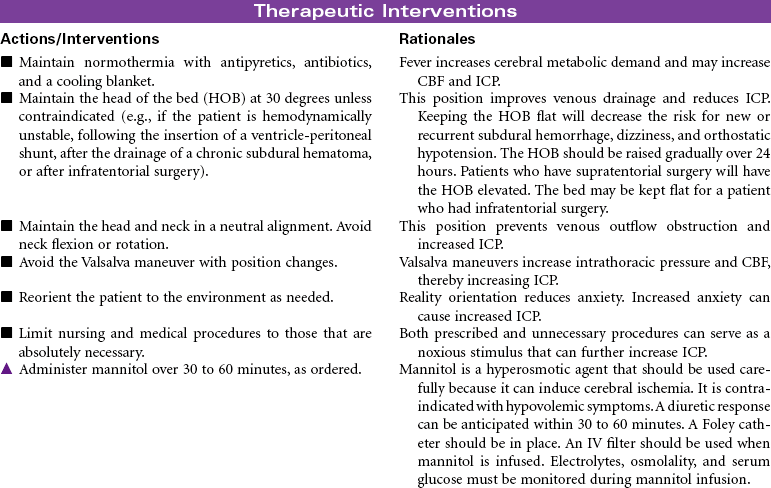
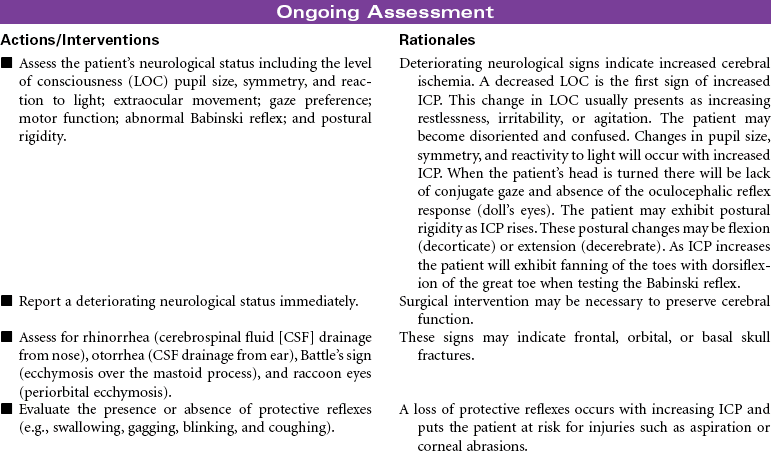
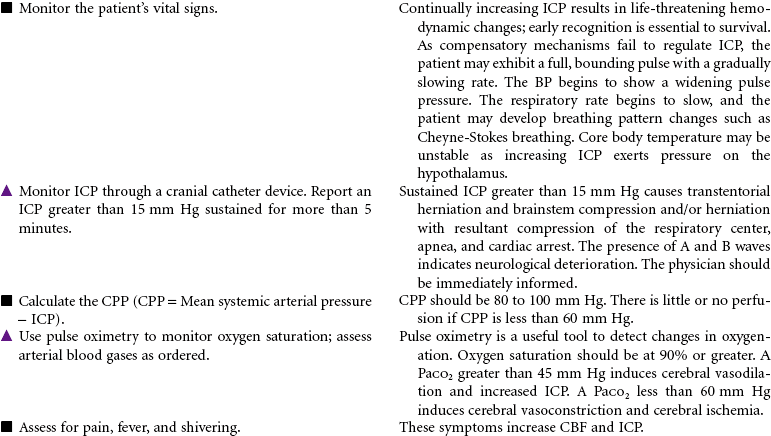
 Decreased Intracranial Adaptive Capacity
Decreased Intracranial Adaptive Capacity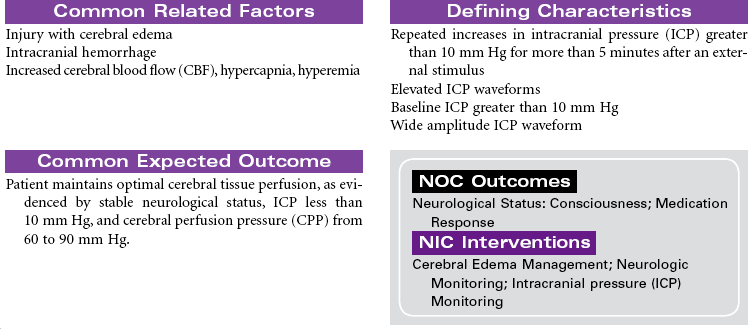
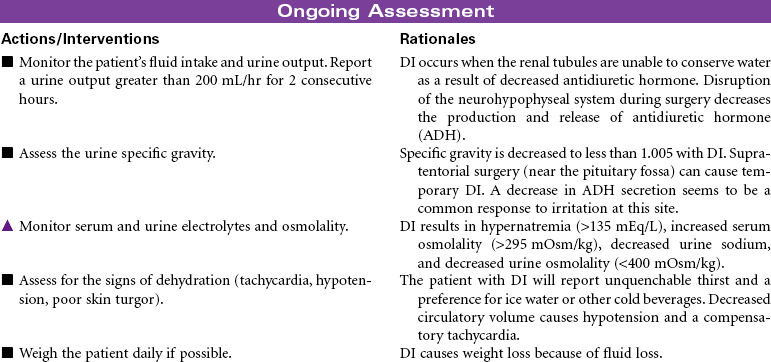
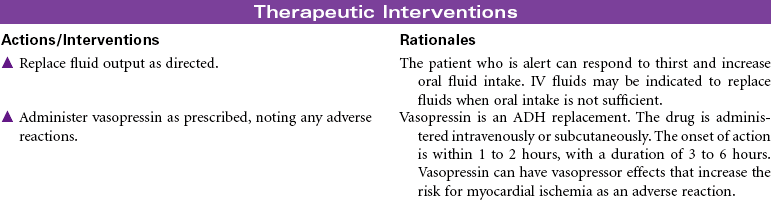
 Risk for Deficient Fluid Volume
Risk for Deficient Fluid Volume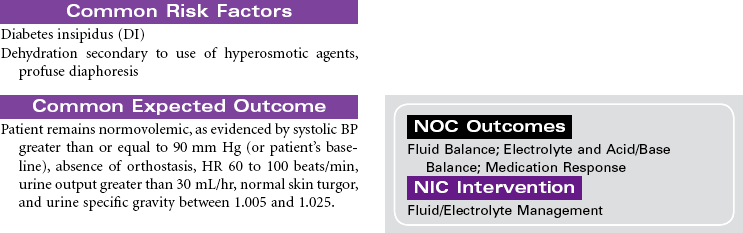


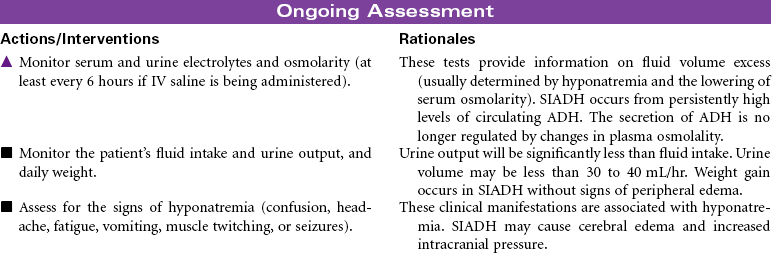
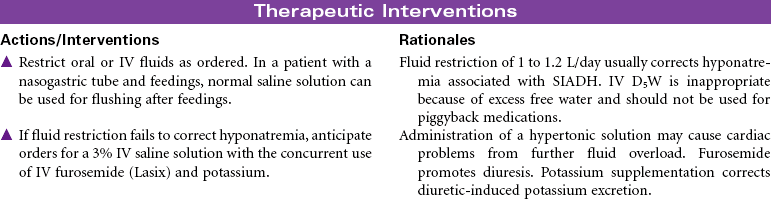
 Risk for Excess Fluid Volume
Risk for Excess Fluid Volume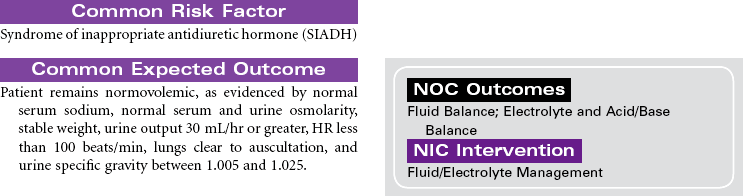
 Risk for Seizures
Risk for Seizures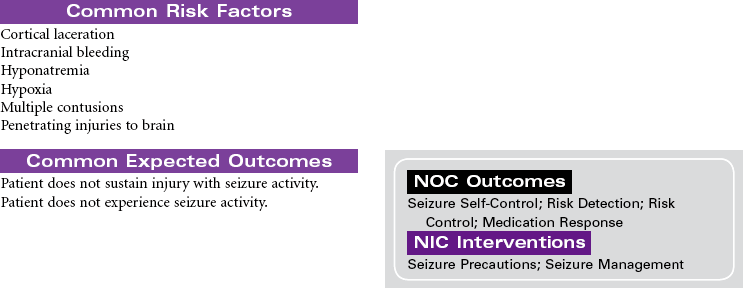



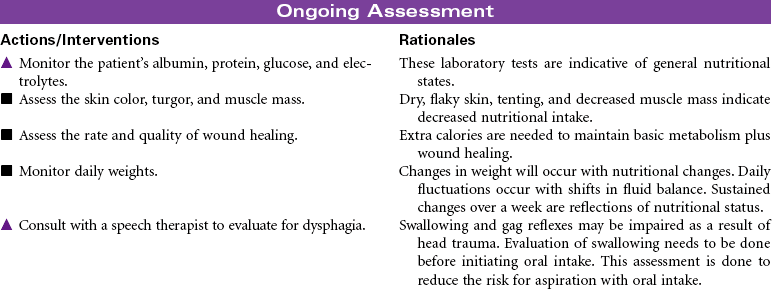
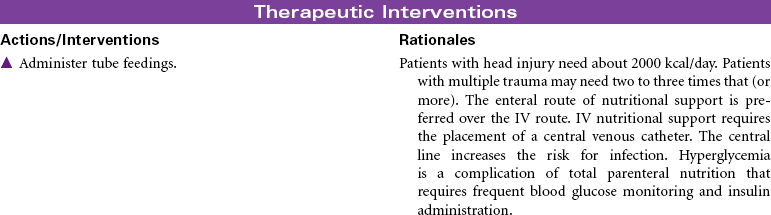
 Risk for Imbalanced Nutrition: Less Than Body Requirements
Risk for Imbalanced Nutrition: Less Than Body Requirements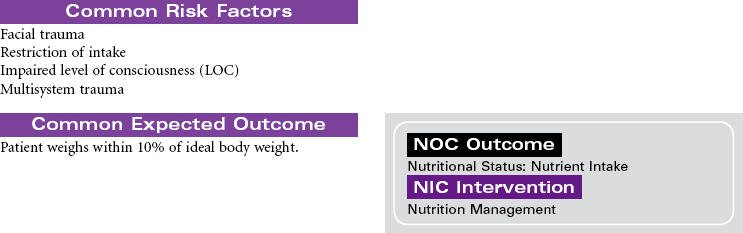

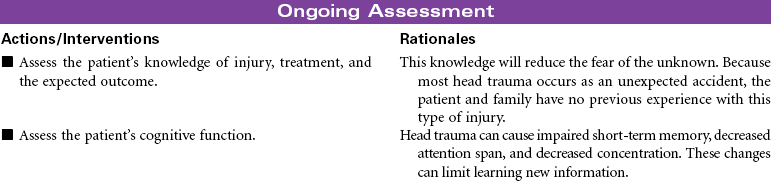
 Deficient Knowledge
Deficient Knowledge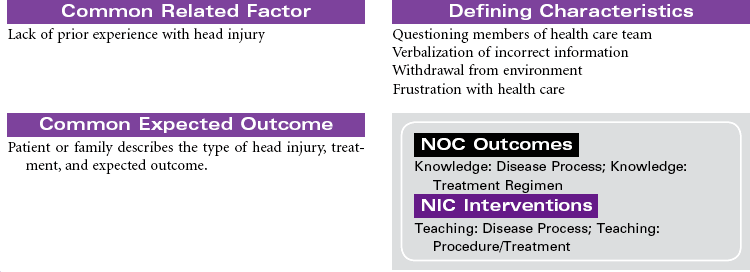
 Deficient Knowledge
Deficient Knowledge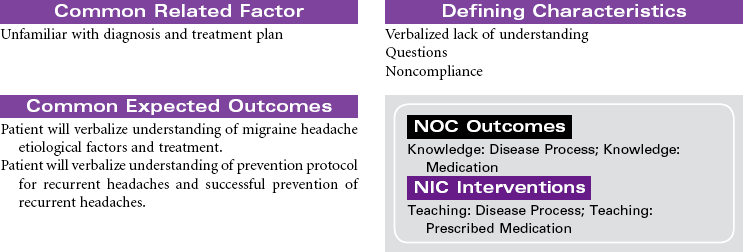



Get Clinical Tree app for offline access
