Chapter 9 Musculoskeletal Care Plans = Independent = Collaborative For additional care plans, go to http://evolve.elsevier.com/Gulanick/. Amputation, Lower Extremity Generally there are about 11 lower limb amputations for every upper limb amputation performed. The level of the amputation depends on the amount of affected tissue, the ability of the blood supply to promote healing, and the prognosis for fitting a functional prosthesis. The leading cause of amputation is vascular disease, with an equal prevalence rate in men and women, who are usually in the 61- to 70-year-old age range. Clinical conditions that predispose the patient to amputation include peripheral arterial disease, diabetes mellitus, and Buerger’s disease. The second leading cause of amputation is trauma, in which the accident itself may sever the limb or in which the limb is so damaged that it must be removed after the accident. Primary bone tumors account for less than 5% of all amputations, with about one third of these occurring in the 16- to 20-year-old age range. The surgical procedure for an uncomplicated amputation rarely requires hospitalization for more than 5 days, but often the clinical situations surrounding amputation make these patients medically unstable and requiring longer lengths of stay. The portion of the limb that remains intact after the surgery is referred to as the residual limb or stump and may be fitted with an artificial device called a prosthesis that takes the place of the severed limb. The vast majority of recovery takes place out of the hospital, either in a rehabilitation center or on an outpatient basis. This care plan primarily covers information about patient care before and immediately after lower extremity amputation. Because nurses will encounter patients in various stages of recovery and rehabilitation, references are made about posthospitalization rehabilitation. Anxiety, Preoperative Impaired Skin Integrity Impaired Physical Mobility Disturbed Body Image Acute Pain and Chronic Pain Deficient Knowledge Related Care Plans Ineffective coping, p. 53 Risks for falls, p. 64 Risk for infection, p. 106 Ineffective peripheral tissue perfusion, p. 197 Surgical experience: Preoperative and postoperative care, p. 235 Arthritis, Rheumatoid Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory disease. RA is classified as an autoimmune disorder that develops as a result of interactions between autoantibodies and immunoglobulins. Rheumatoid factor (RF) is the primary autoantibody that acts against immunoglobulin G (IgG). The disorder usually presents as symmetrical synovitis primarily of the small joints of the body. The diagnosis of RA is based on the presence of criteria established by the American Rheumatism Association. These criteria include morning joint stiffness lasting at least 1 hour, soft-tissue swelling of three or more joint areas, simultaneous symmetrical joint swelling, subcutaneous rheumatoid nodules, presence of RF in the serum, and radiographic evidence of joint erosion or periarticular osteopenia. Synovial fluid analysis may be done to confirm the diagnosis of RA. Extra-articular manifestations may include rheumatoid nodules, pericarditis, scleritis, and arteritis. RA is characterized by periods of remission and prolonged exacerbation of the disease, during which the joints can become damaged. In the initial phase of RA, the synovial membrane becomes inflamed and thickens, associated with an increased production of synovial fluid. As this tissue develops, it causes erosion and destruction of the joint capsule and subchondral bone. These processes result in decreased joint motion, deformity, and finally ankylosis, or joint immobilization. Anyone can develop RA, including children and older adults, but it usually strikes people in the young to middle years. RA strikes women at a 3 : 1 ratio compared with men and occurs in all ethnic groups worldwide. The specific cause of RA is unknown, but the tendency to develop it may be inherited. The gene that seems to control RA is one of the genes that control the immune system, but not everyone who has this gene goes on to develop RA. The disease behaves differently in each person who contracts it. In some people the joint inflammation that marks RA will be mild, with long periods of remission between “exacerbations,” or increased periods of disease activity. For others the activity of the disease may seem continuous and worsening as time passes. The goals of treatment are to relieve pain and inflammation and reduce joint damage. The long-term goal of treatment is to maintain or restore use in the joints damaged by RA. This care plan focuses on the outpatient management of patients who are affected by RA. Deficient Knowledge Joint Pain Joint Stiffness Impaired Physical Mobility Related Care Plans Chronic pain, p. 148 Fatigue, p. 70 Self-care deficit, p. 163 Risk for infection, p. 106 Arthroscopy Arthroscopy is the direct visualization of a joint interior using a rigid fiberoptic endoscope. The procedure can be done for diagnostic evaluation or surgical repair of a joint. Arthroscopy is used when joint problems cannot be identified by noninvasive techniques such as x-ray examination. The procedure has wide application in the diagnosis and management of joint problems associated with sports injuries, degenerative disorders, and acute or chronic inflammatory disorders. Most arthroscopic procedures are done to evaluate and correct injuries to the knee. Problems related to the meniscus, cartilage, and ligaments of the knee can be repaired with arthroscopy. There is increasing use of the technique with other joints in the body such as rotator cuff injuries of the shoulder. Joint arthroscopy may be used in patients with rheumatoid arthritis (RA) to remove joint debris and thereby reduce joint pain. Advantages of this procedure for the patient include decreased surgical risks and fewer complications because it can be done using smaller incisions and usually with local or regional anesthesia. Complications of arthroscopy are not common but include infection, neurovascular damage, hemarthrosis (bleeding into the joint), and joint injury. The majority of arthroscopic procedures are done on an outpatient basis. Deficient Knowledge Acute Pain Impaired Physical Mobility Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Endocrine and Metabolic Care Plans Integumentary Care Plans Cardiac and Vascular Care Plans Nursing Diagnosis Care Plans Stay updated, free articles. Join our Telegram channel Join Tags: Nursing Care Plans Nursing Diagnosis and Intervention Dec 3, 2016 | Posted by admin in NURSING | Comments Off on Musculoskeletal Care Plans Full access? Get Clinical Tree
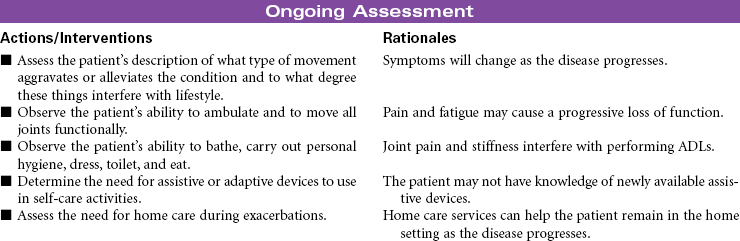
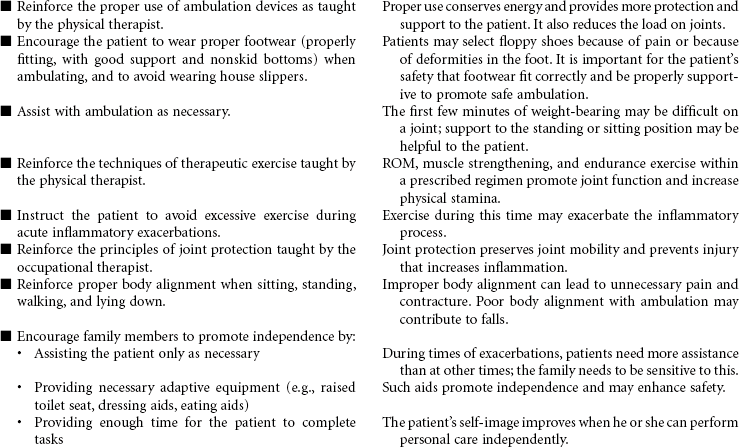
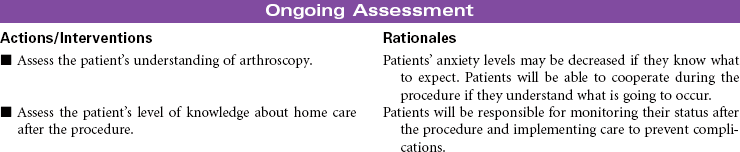
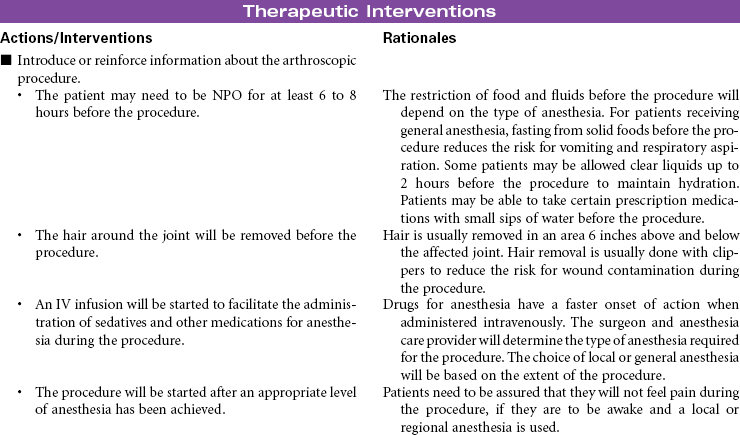
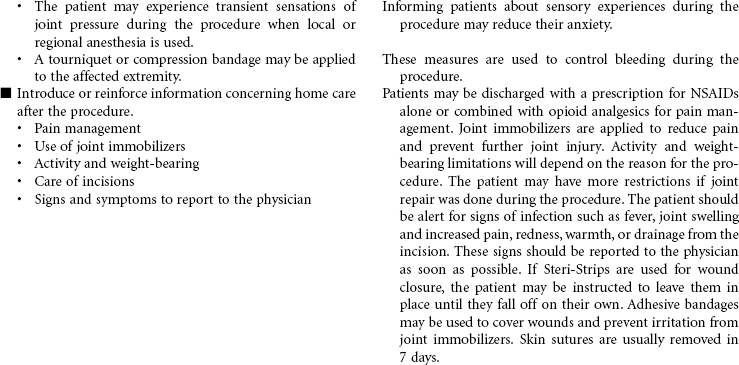
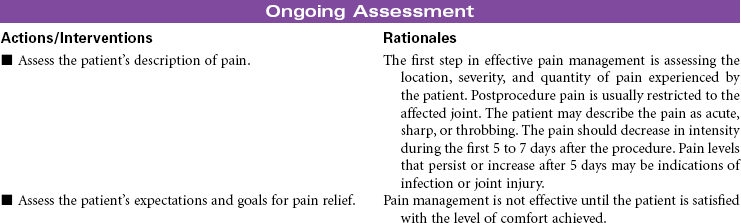
Chapter 9 Musculoskeletal Care Plans = Independent = Collaborative For additional care plans, go to http://evolve.elsevier.com/Gulanick/. Amputation, Lower Extremity Generally there are about 11 lower limb amputations for every upper limb amputation performed. The level of the amputation depends on the amount of affected tissue, the ability of the blood supply to promote healing, and the prognosis for fitting a functional prosthesis. The leading cause of amputation is vascular disease, with an equal prevalence rate in men and women, who are usually in the 61- to 70-year-old age range. Clinical conditions that predispose the patient to amputation include peripheral arterial disease, diabetes mellitus, and Buerger’s disease. The second leading cause of amputation is trauma, in which the accident itself may sever the limb or in which the limb is so damaged that it must be removed after the accident. Primary bone tumors account for less than 5% of all amputations, with about one third of these occurring in the 16- to 20-year-old age range. The surgical procedure for an uncomplicated amputation rarely requires hospitalization for more than 5 days, but often the clinical situations surrounding amputation make these patients medically unstable and requiring longer lengths of stay. The portion of the limb that remains intact after the surgery is referred to as the residual limb or stump and may be fitted with an artificial device called a prosthesis that takes the place of the severed limb. The vast majority of recovery takes place out of the hospital, either in a rehabilitation center or on an outpatient basis. This care plan primarily covers information about patient care before and immediately after lower extremity amputation. Because nurses will encounter patients in various stages of recovery and rehabilitation, references are made about posthospitalization rehabilitation. Anxiety, Preoperative Impaired Skin Integrity Impaired Physical Mobility Disturbed Body Image Acute Pain and Chronic Pain Deficient Knowledge Related Care Plans Ineffective coping, p. 53 Risks for falls, p. 64 Risk for infection, p. 106 Ineffective peripheral tissue perfusion, p. 197 Surgical experience: Preoperative and postoperative care, p. 235 Arthritis, Rheumatoid Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory disease. RA is classified as an autoimmune disorder that develops as a result of interactions between autoantibodies and immunoglobulins. Rheumatoid factor (RF) is the primary autoantibody that acts against immunoglobulin G (IgG). The disorder usually presents as symmetrical synovitis primarily of the small joints of the body. The diagnosis of RA is based on the presence of criteria established by the American Rheumatism Association. These criteria include morning joint stiffness lasting at least 1 hour, soft-tissue swelling of three or more joint areas, simultaneous symmetrical joint swelling, subcutaneous rheumatoid nodules, presence of RF in the serum, and radiographic evidence of joint erosion or periarticular osteopenia. Synovial fluid analysis may be done to confirm the diagnosis of RA. Extra-articular manifestations may include rheumatoid nodules, pericarditis, scleritis, and arteritis. RA is characterized by periods of remission and prolonged exacerbation of the disease, during which the joints can become damaged. In the initial phase of RA, the synovial membrane becomes inflamed and thickens, associated with an increased production of synovial fluid. As this tissue develops, it causes erosion and destruction of the joint capsule and subchondral bone. These processes result in decreased joint motion, deformity, and finally ankylosis, or joint immobilization. Anyone can develop RA, including children and older adults, but it usually strikes people in the young to middle years. RA strikes women at a 3 : 1 ratio compared with men and occurs in all ethnic groups worldwide. The specific cause of RA is unknown, but the tendency to develop it may be inherited. The gene that seems to control RA is one of the genes that control the immune system, but not everyone who has this gene goes on to develop RA. The disease behaves differently in each person who contracts it. In some people the joint inflammation that marks RA will be mild, with long periods of remission between “exacerbations,” or increased periods of disease activity. For others the activity of the disease may seem continuous and worsening as time passes. The goals of treatment are to relieve pain and inflammation and reduce joint damage. The long-term goal of treatment is to maintain or restore use in the joints damaged by RA. This care plan focuses on the outpatient management of patients who are affected by RA. Deficient Knowledge Joint Pain Joint Stiffness Impaired Physical Mobility Related Care Plans Chronic pain, p. 148 Fatigue, p. 70 Self-care deficit, p. 163 Risk for infection, p. 106 Arthroscopy Arthroscopy is the direct visualization of a joint interior using a rigid fiberoptic endoscope. The procedure can be done for diagnostic evaluation or surgical repair of a joint. Arthroscopy is used when joint problems cannot be identified by noninvasive techniques such as x-ray examination. The procedure has wide application in the diagnosis and management of joint problems associated with sports injuries, degenerative disorders, and acute or chronic inflammatory disorders. Most arthroscopic procedures are done to evaluate and correct injuries to the knee. Problems related to the meniscus, cartilage, and ligaments of the knee can be repaired with arthroscopy. There is increasing use of the technique with other joints in the body such as rotator cuff injuries of the shoulder. Joint arthroscopy may be used in patients with rheumatoid arthritis (RA) to remove joint debris and thereby reduce joint pain. Advantages of this procedure for the patient include decreased surgical risks and fewer complications because it can be done using smaller incisions and usually with local or regional anesthesia. Complications of arthroscopy are not common but include infection, neurovascular damage, hemarthrosis (bleeding into the joint), and joint injury. The majority of arthroscopic procedures are done on an outpatient basis. Deficient Knowledge Acute Pain Impaired Physical Mobility Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Endocrine and Metabolic Care Plans Integumentary Care Plans Cardiac and Vascular Care Plans Nursing Diagnosis Care Plans Stay updated, free articles. Join our Telegram channel Join Tags: Nursing Care Plans Nursing Diagnosis and Intervention Dec 3, 2016 | Posted by admin in NURSING | Comments Off on Musculoskeletal Care Plans Full access? Get Clinical Tree
 = Independent
= Independent  = Collaborative
= Collaborative For additional care plans, go to
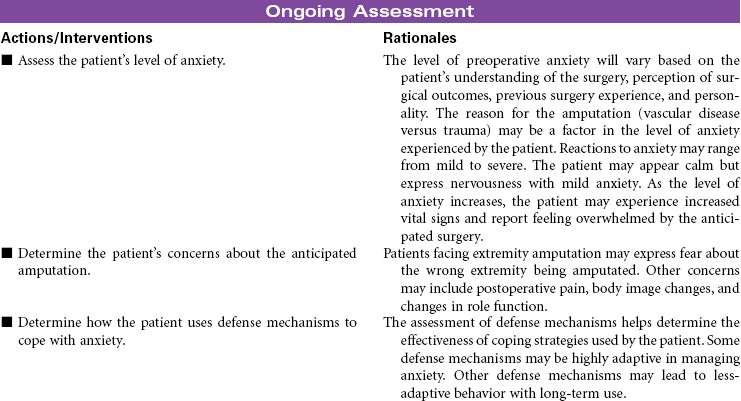
For additional care plans, go to  Anxiety, Preoperative
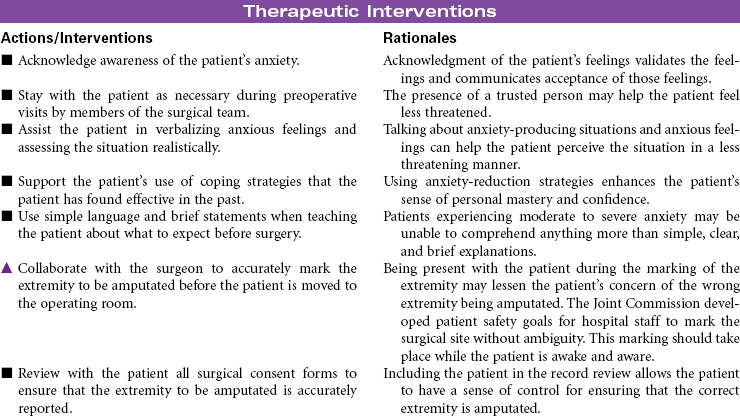
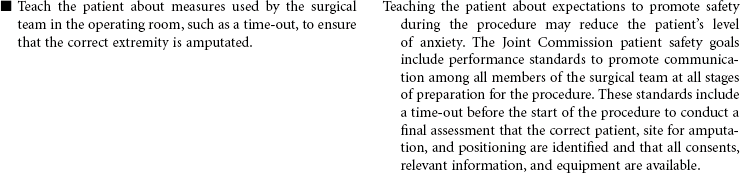
Anxiety, Preoperative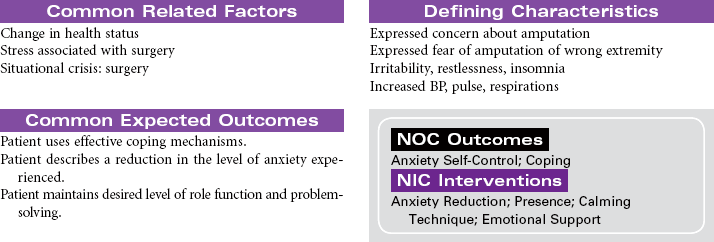
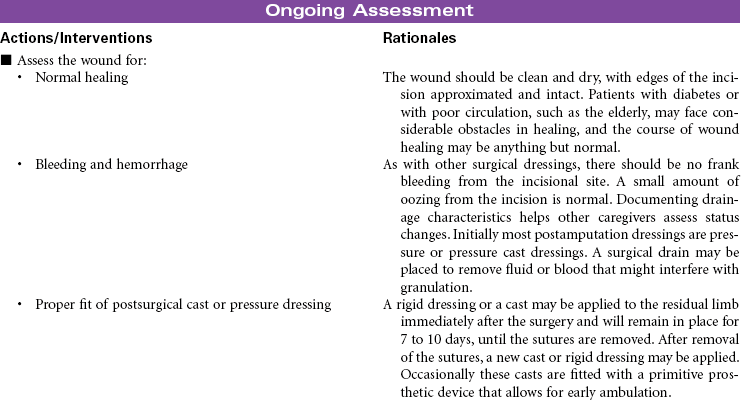
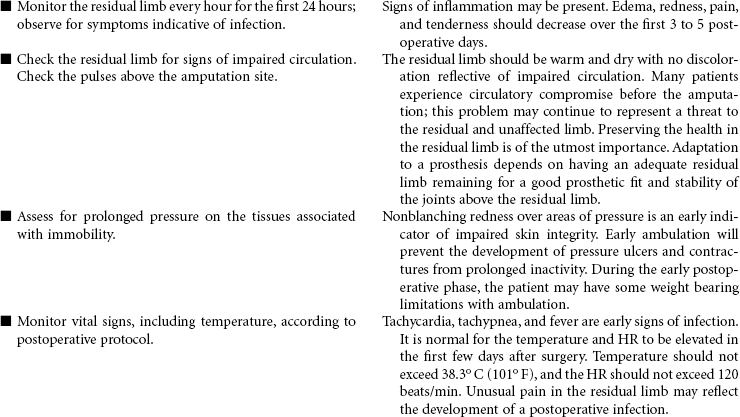
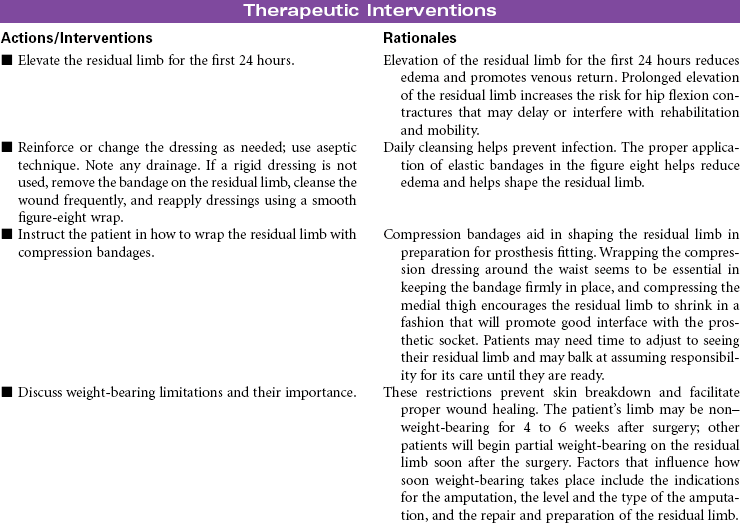
 Impaired Skin Integrity
Impaired Skin Integrity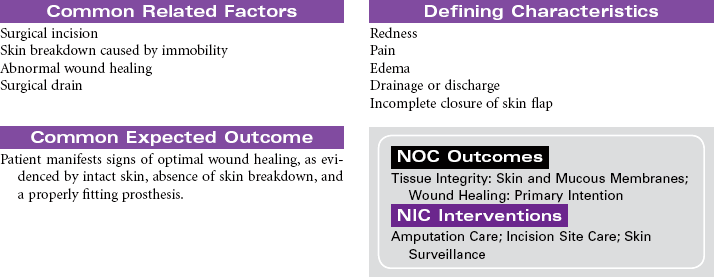

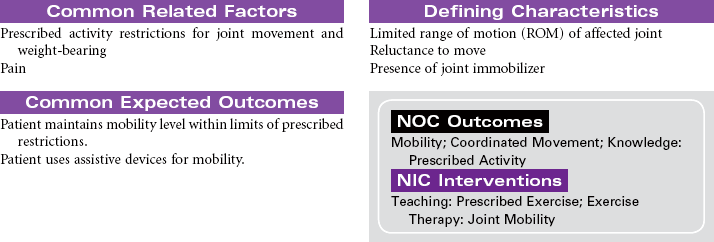
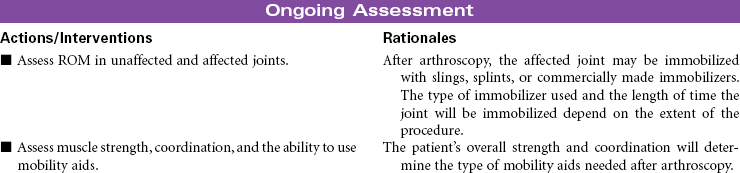
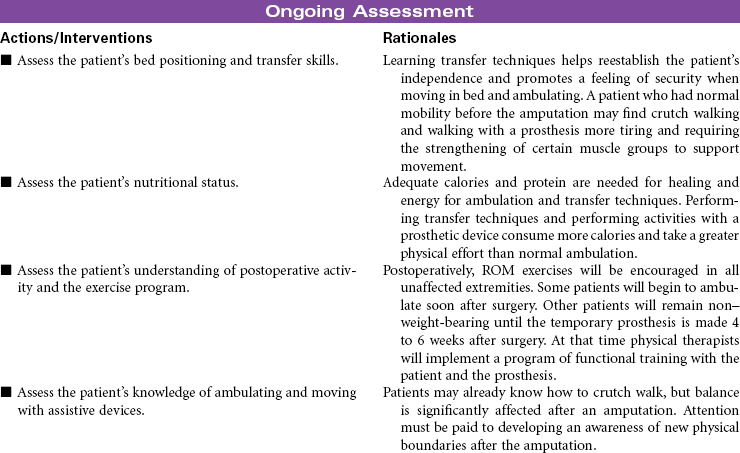
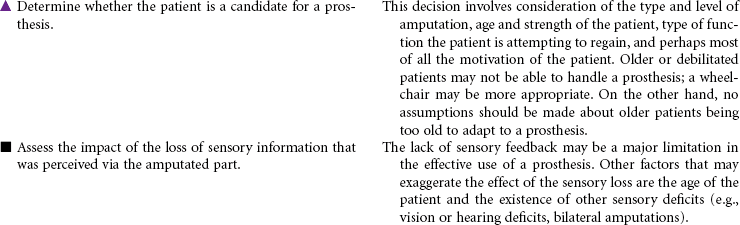
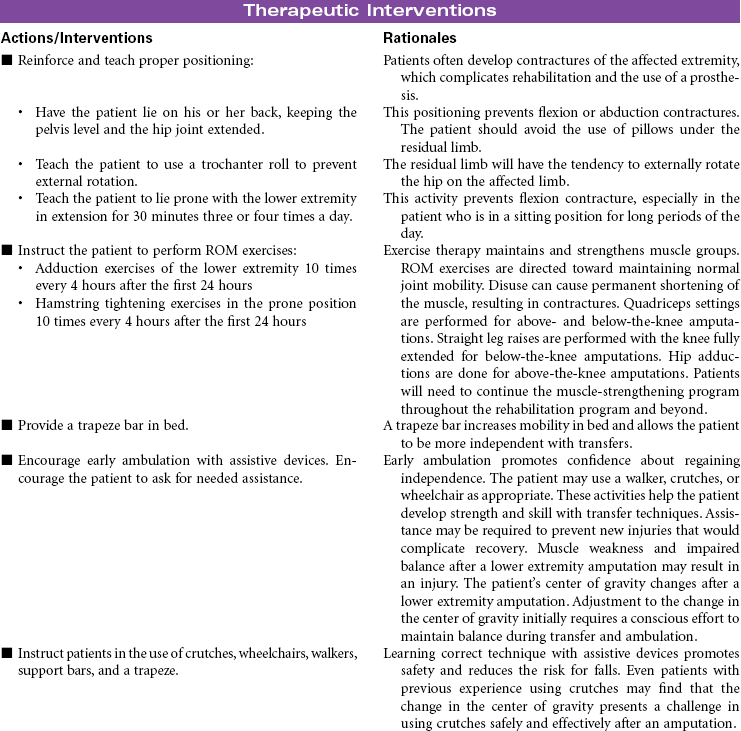
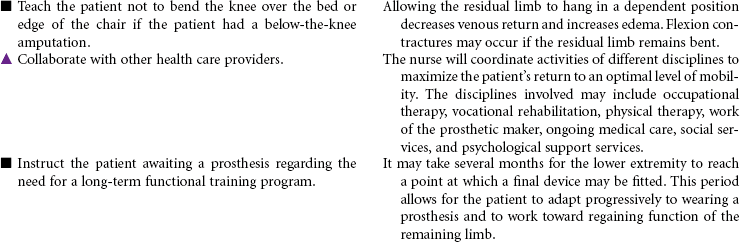
 Impaired Physical Mobility
Impaired Physical Mobility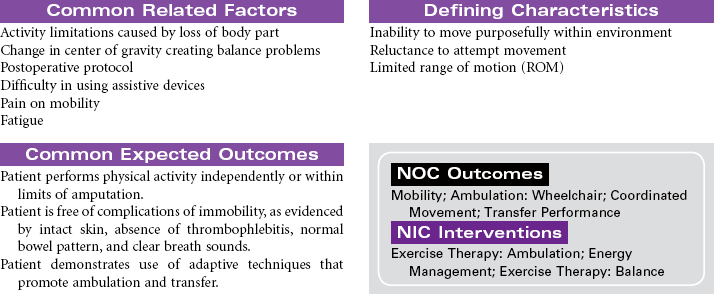
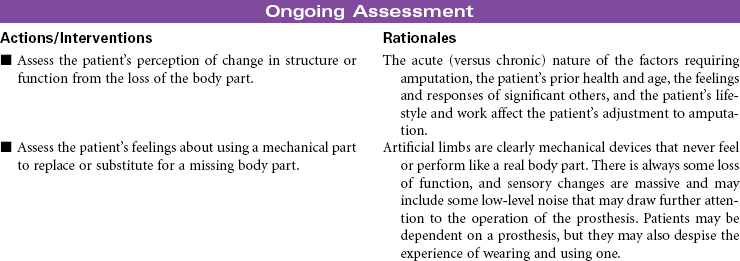
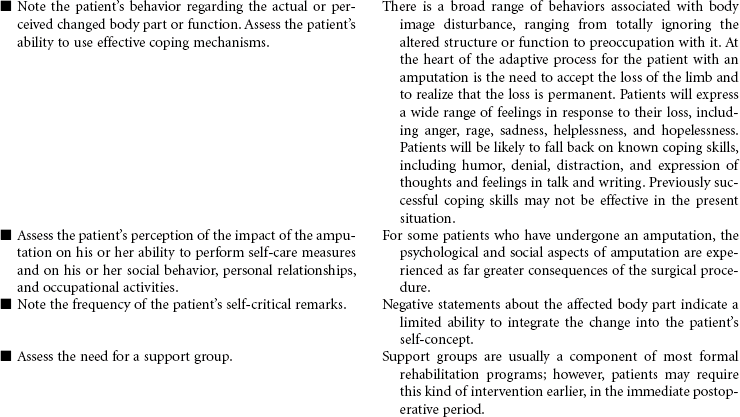
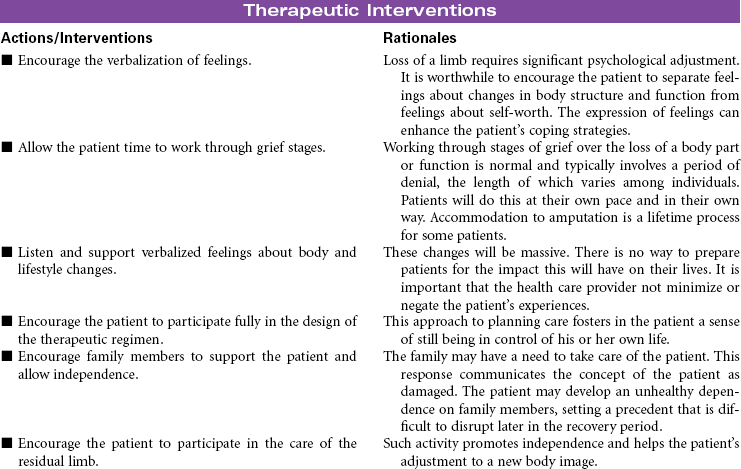
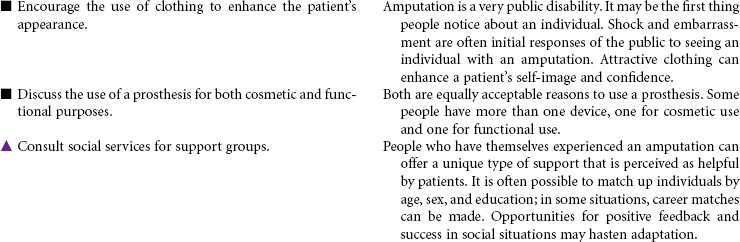
 Disturbed Body Image
Disturbed Body Image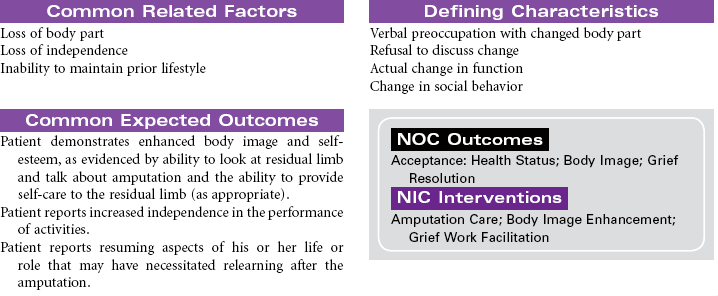
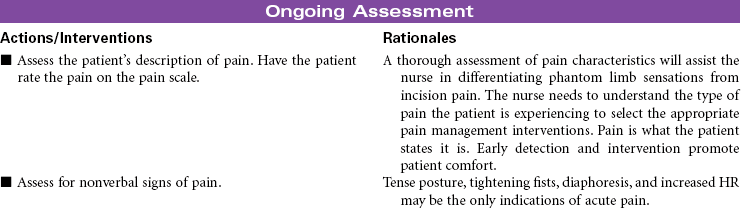
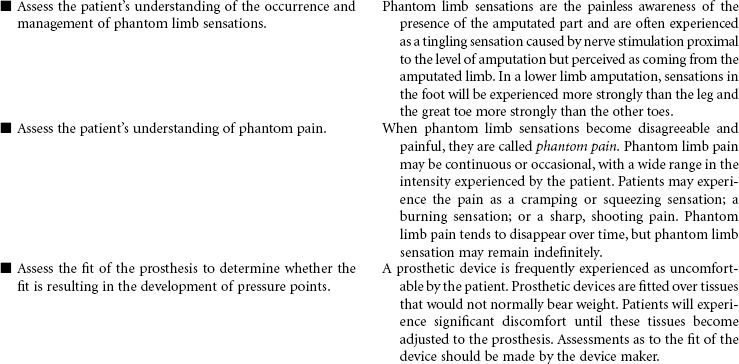
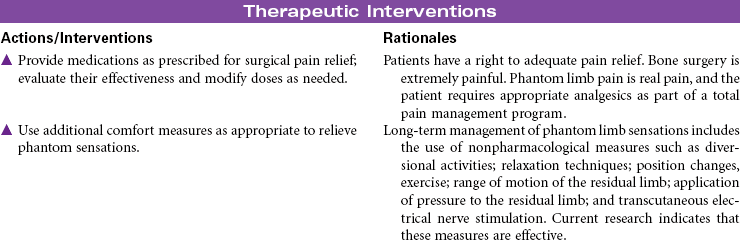
 Acute Pain and Chronic Pain
Acute Pain and Chronic Pain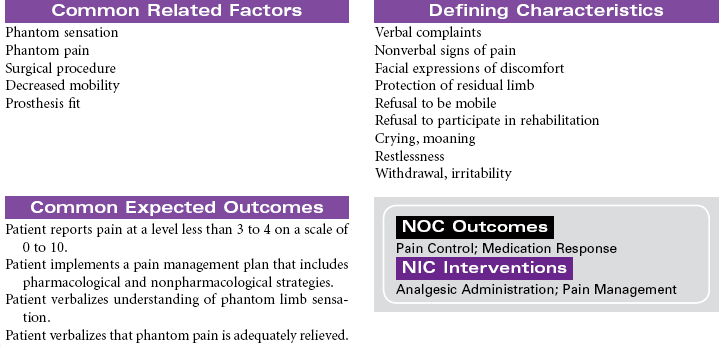
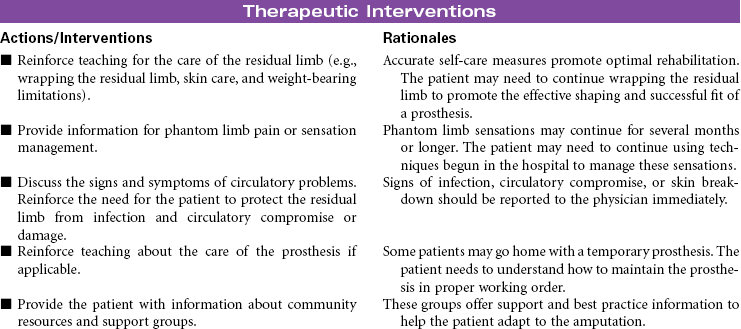
 Deficient Knowledge
Deficient Knowledge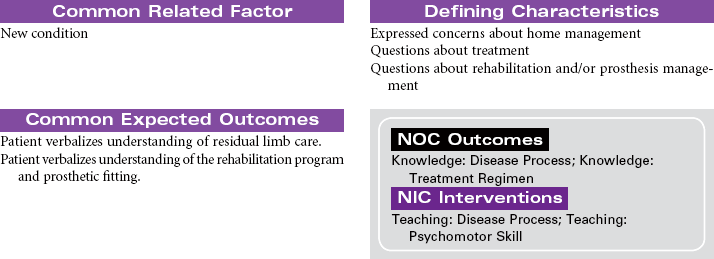

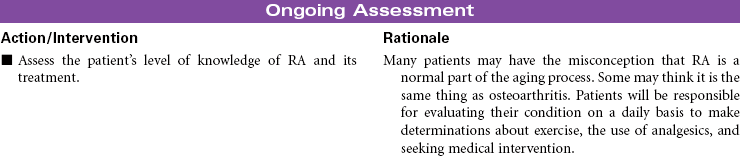
 Deficient Knowledge
Deficient Knowledge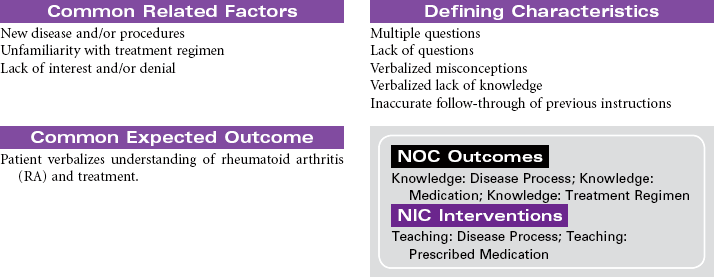


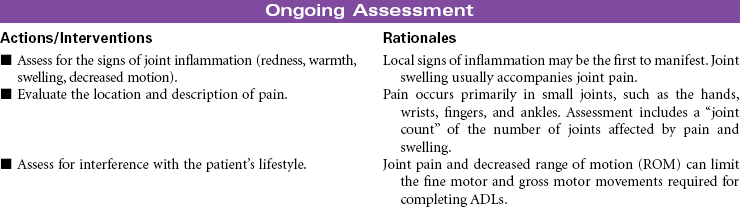
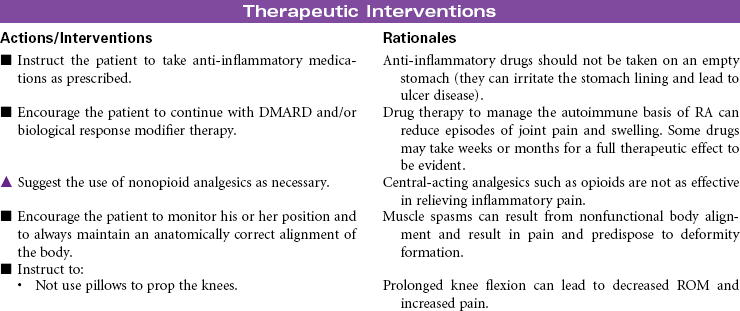
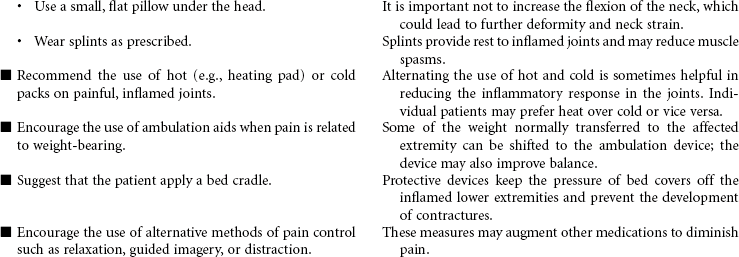
 Joint Pain
Joint Pain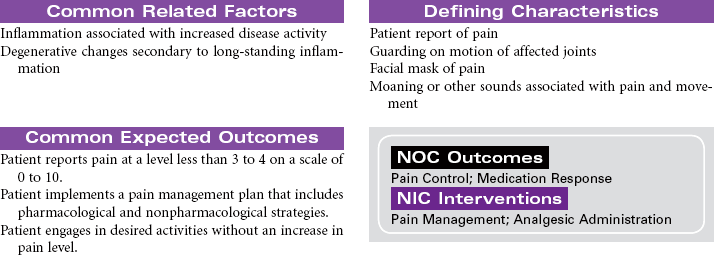
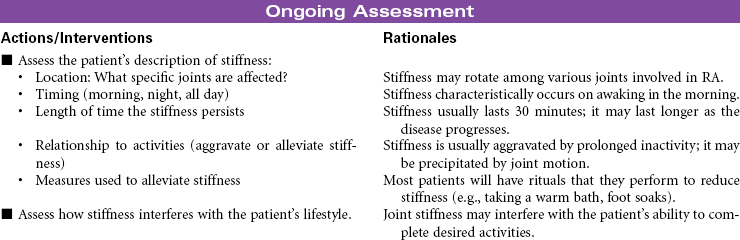
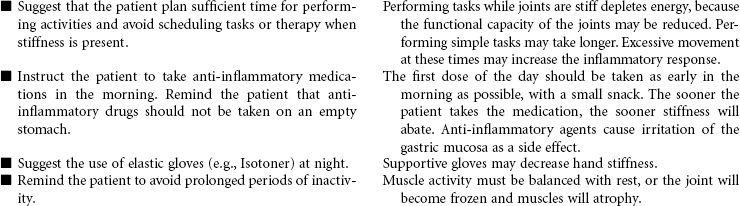
 Joint Stiffness
Joint Stiffness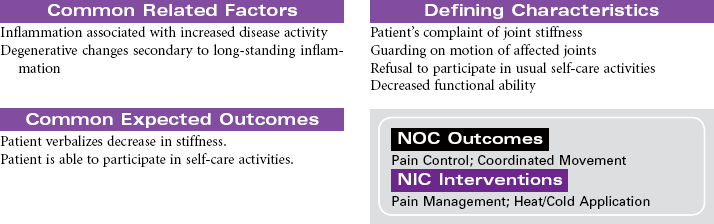

 Impaired Physical Mobility
Impaired Physical Mobility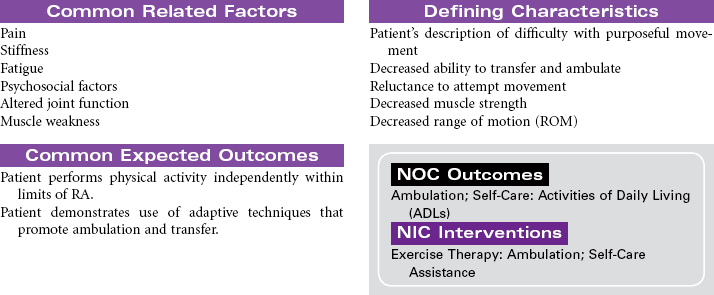

 Deficient Knowledge
Deficient Knowledge
 Acute Pain
Acute Pain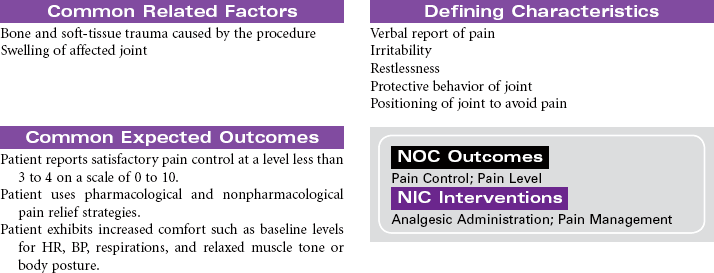
 Impaired Physical Mobility
Impaired Physical Mobility