Chapter 10 Bone Marrow Transplant; Peripheral Blood Stem Cell Transplant There are three major types of transplants: • Syngeneic: Donor from an identical twin • Allogeneic: Can be related (from a matched sibling) or unrelated (from a volunteer in the Be The Match Registry). This is also referred to as a matched unrelated donor (MUD) transplant. There are three sources of hematopoietic stem cells: • Peripheral blood: The stem cells that normally reside in the bone marrow can be moved or mobilized into the bloodstream (peripheral circulation) and collected in an outpatient procedure via a cell separator or apheresis machine. This procedure does not require anesthesia. The majority of all transplants performed today use peripheral blood stem cells rather than bone marrow stem cells. • Bone marrow: These cells are collected from the pelvic bones through a series of aspirations. Bone marrow harvesting is a surgical procedure done under general anesthesia. • Umbilical cord, placental: This is a rich source of stem cells that are collected at the time of delivery from tissue that is normally discarded.
Hematolymphatic, Immunological, and Oncological Care Plans
 For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
Hematopoietic Stem Cell Transplantation
Hematolymphatic, Immunological, and Oncological Care Plans
 = Independent
= Independent  = Collaborative
= Collaborative
 Deficient Knowledge
Deficient Knowledge
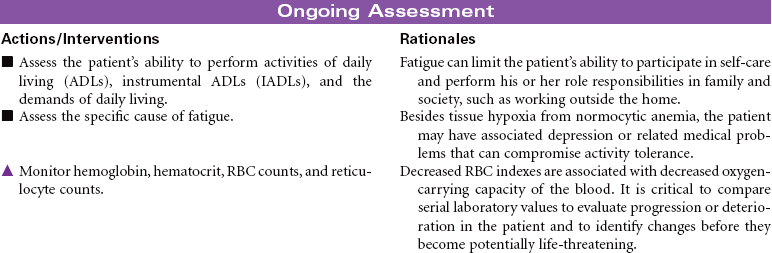
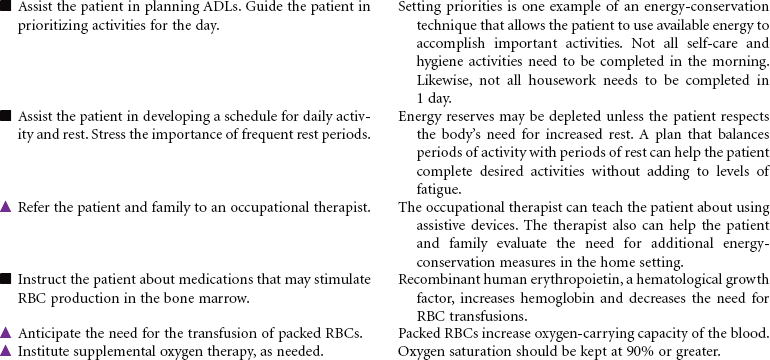
 Fatigue
Fatigue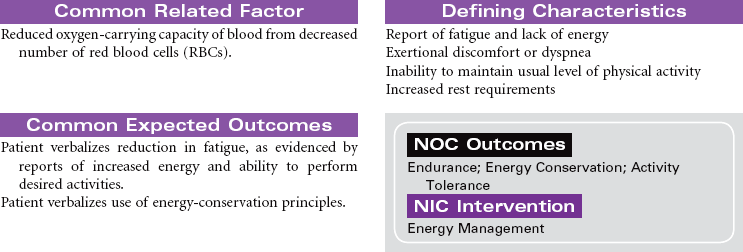

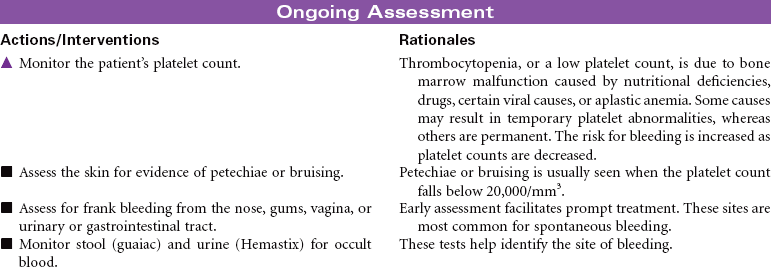
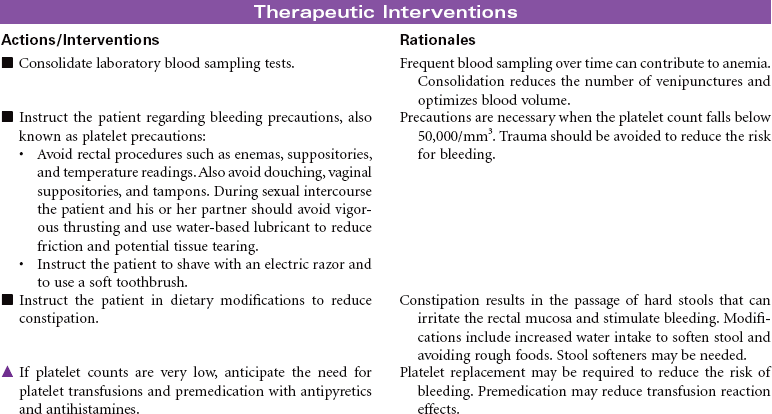
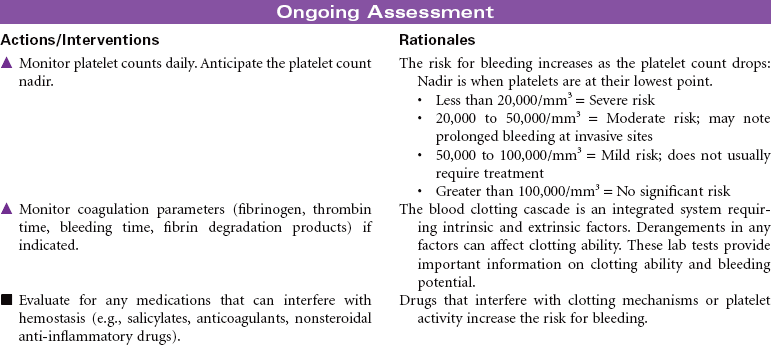
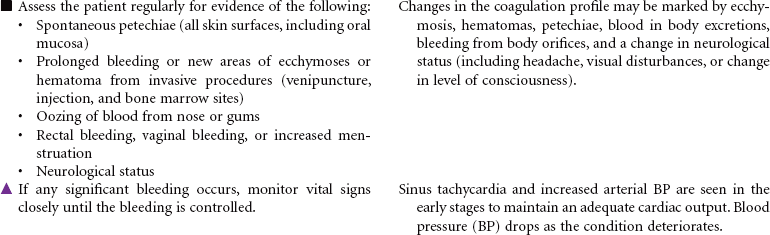
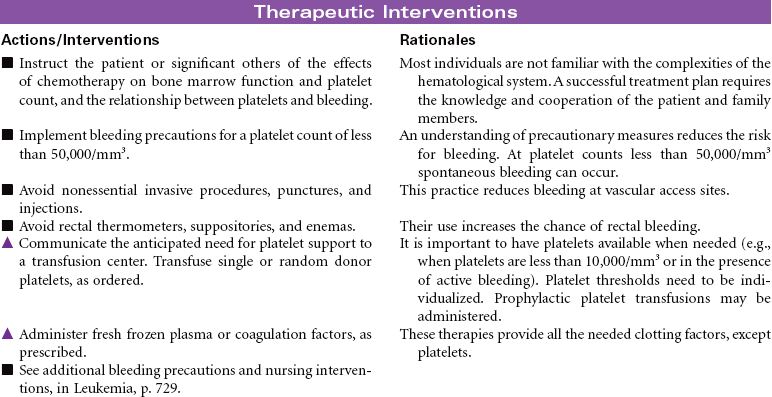
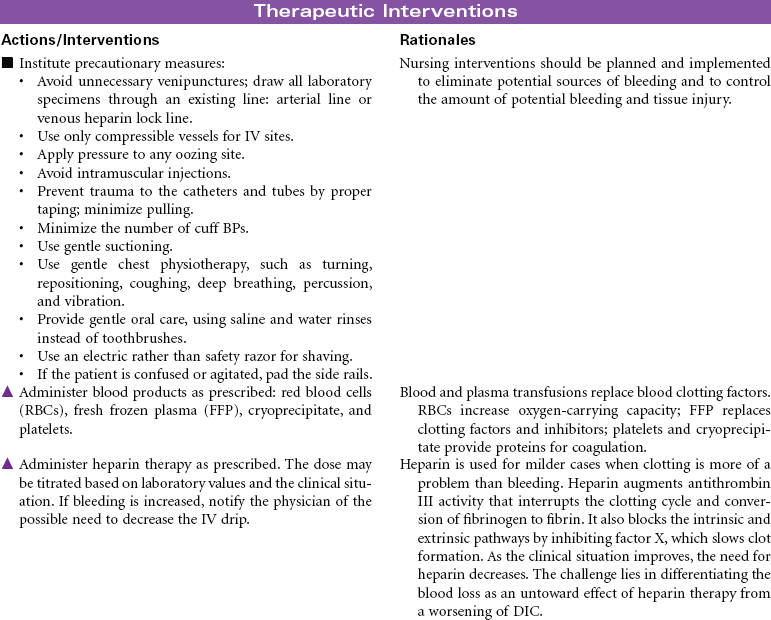
 Risk for Bleeding
Risk for Bleeding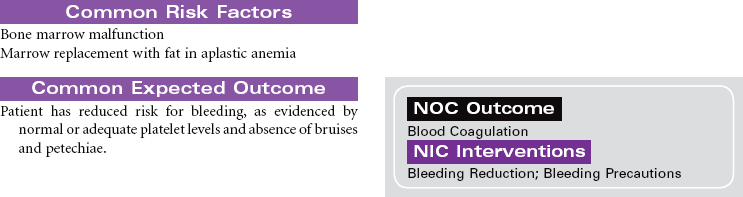
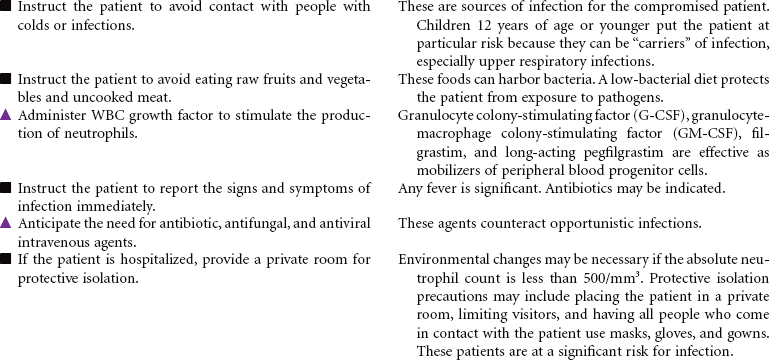
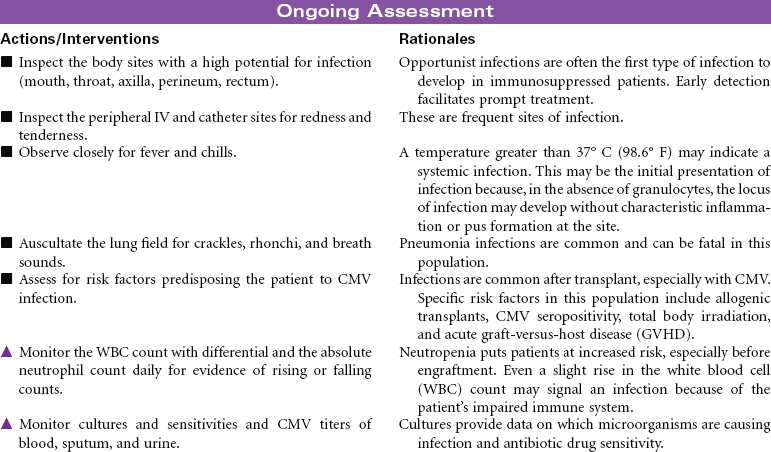
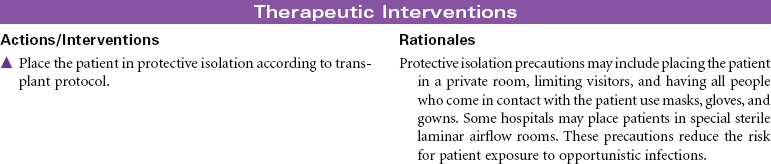
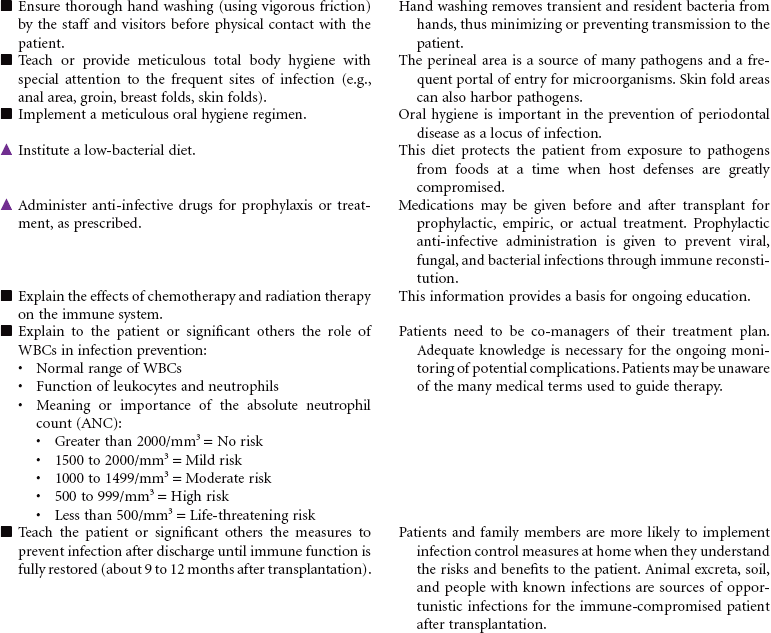
 Risk for Infection
Risk for Infection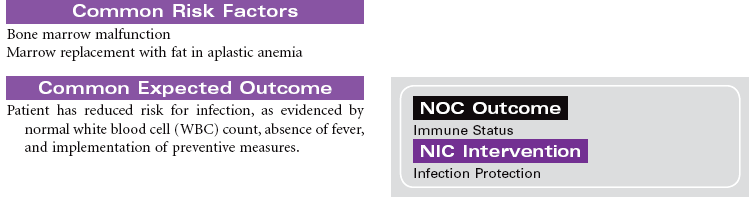


 Deficient Knowledge
Deficient Knowledge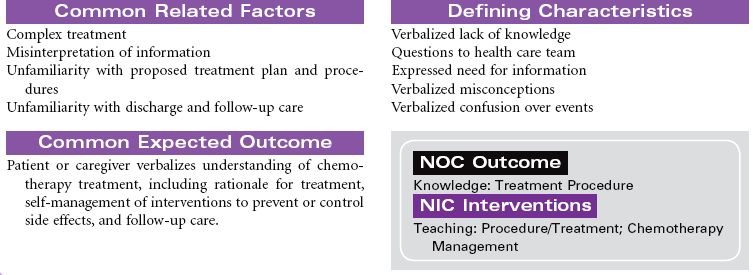
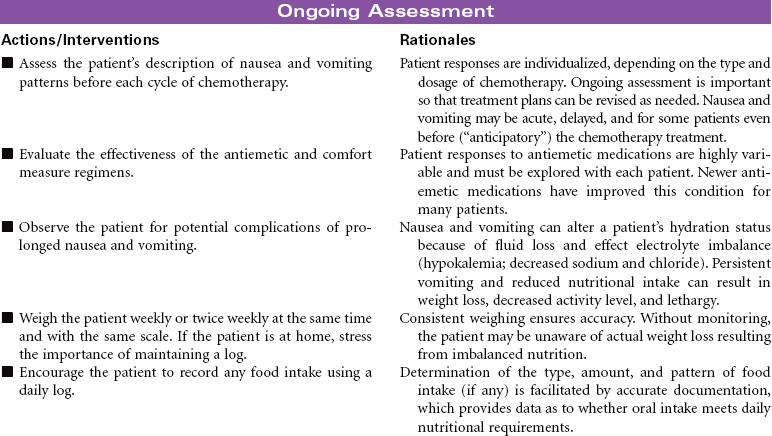
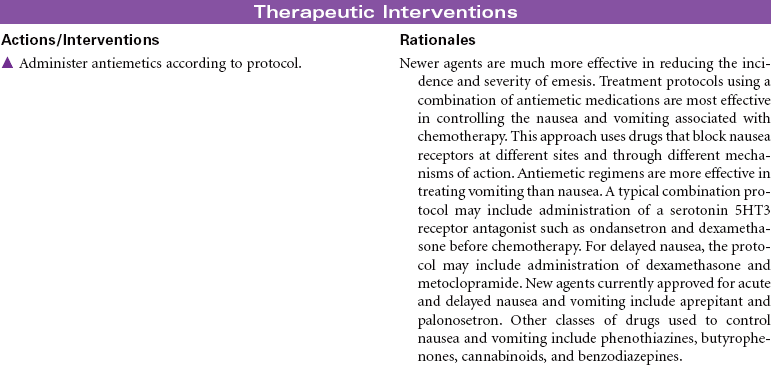
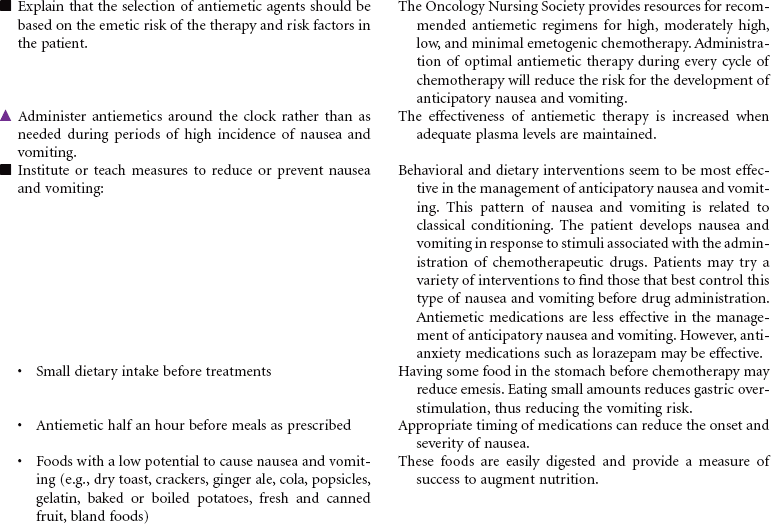
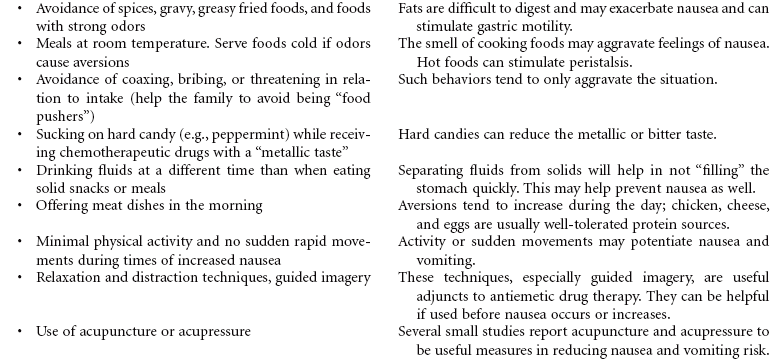
 Nausea
Nausea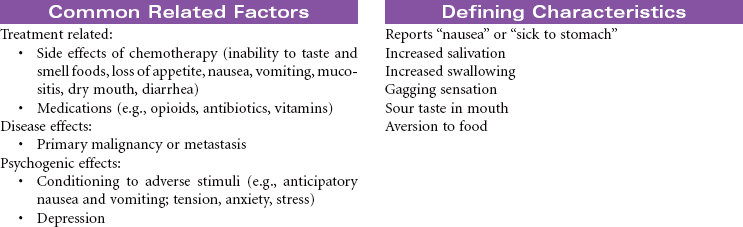
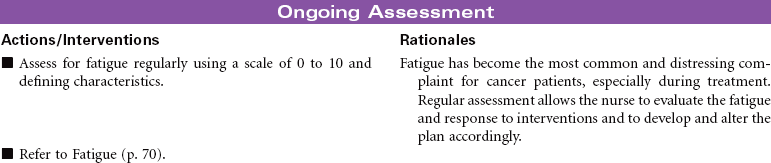
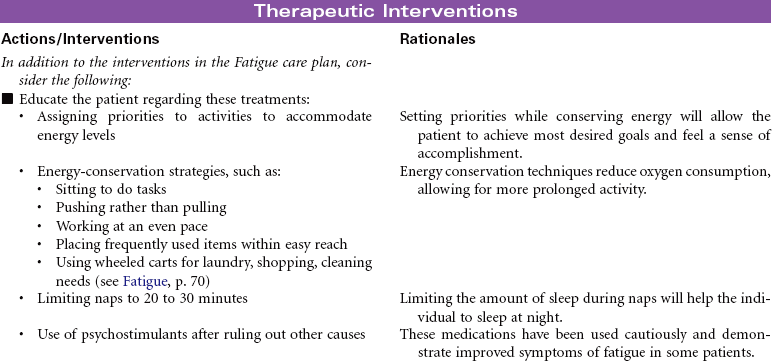
 Cancer-Related Fatigue
Cancer-Related Fatigue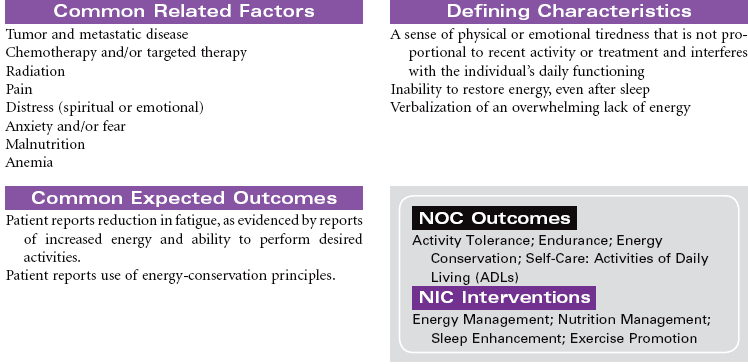
 Risk for Bleeding
Risk for Bleeding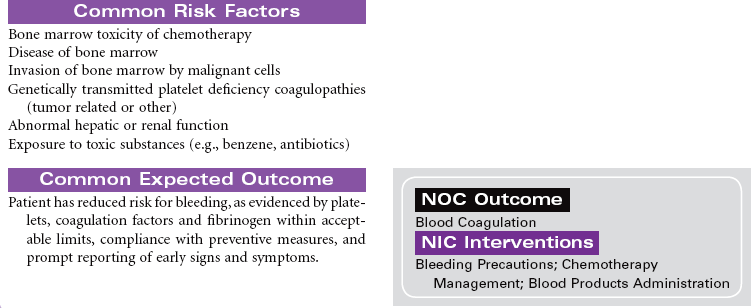
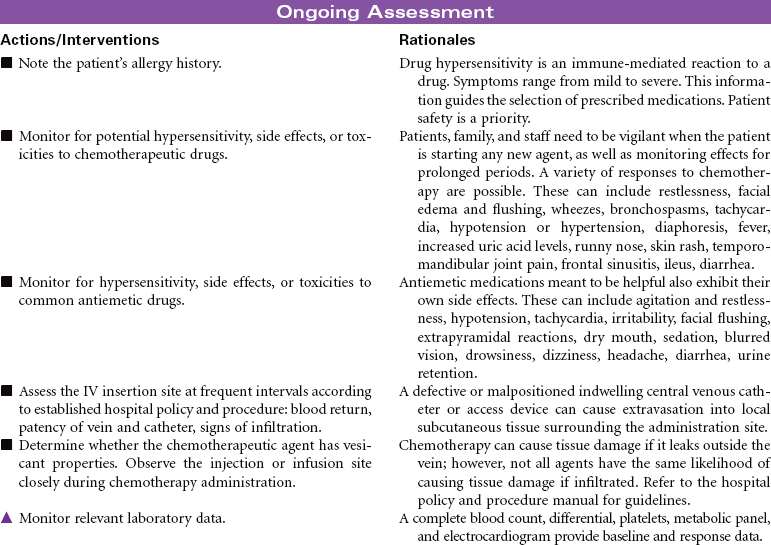
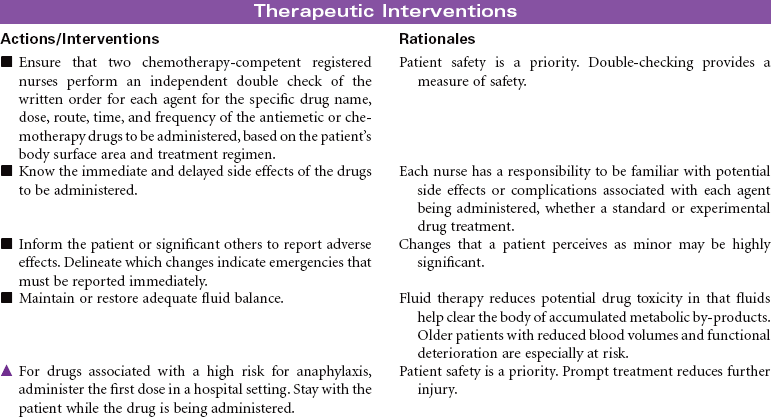
 Risk for Injury
Risk for Injury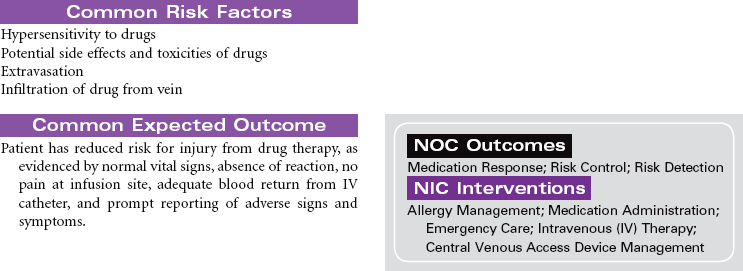
 Disturbed Body Image
Disturbed Body Image
 Risk for Injury
Risk for Injury

 Deficient Knowledge
Deficient Knowledge
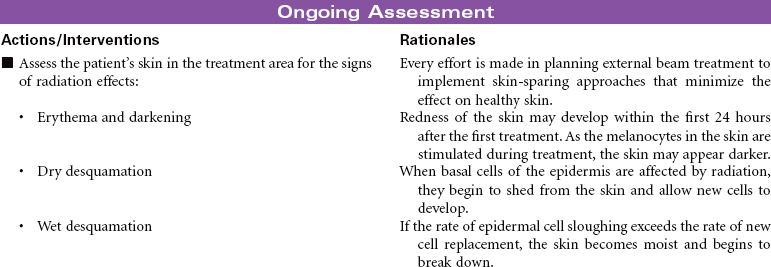
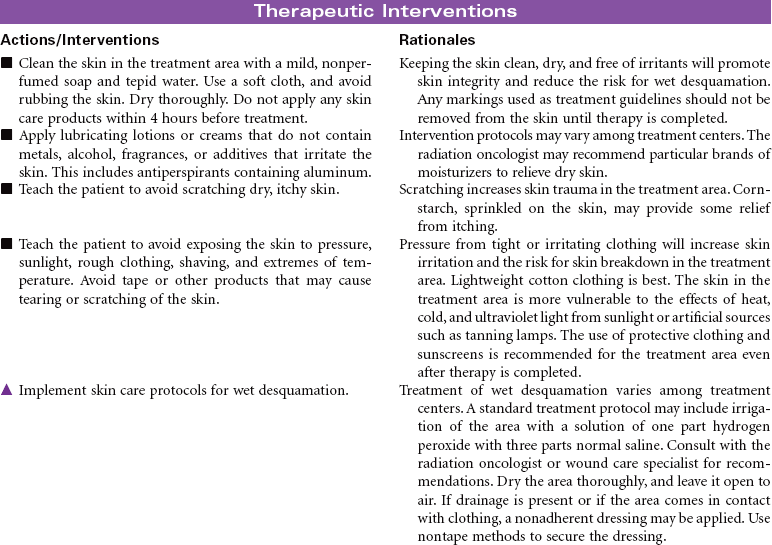
 Risk for Impaired Skin Integrity
Risk for Impaired Skin Integrity

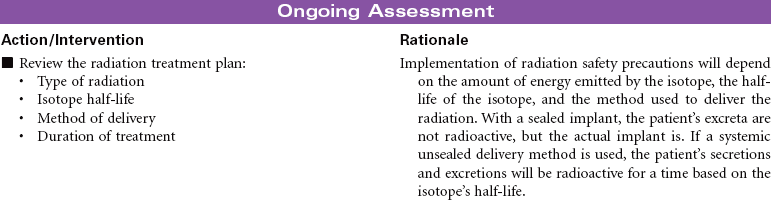
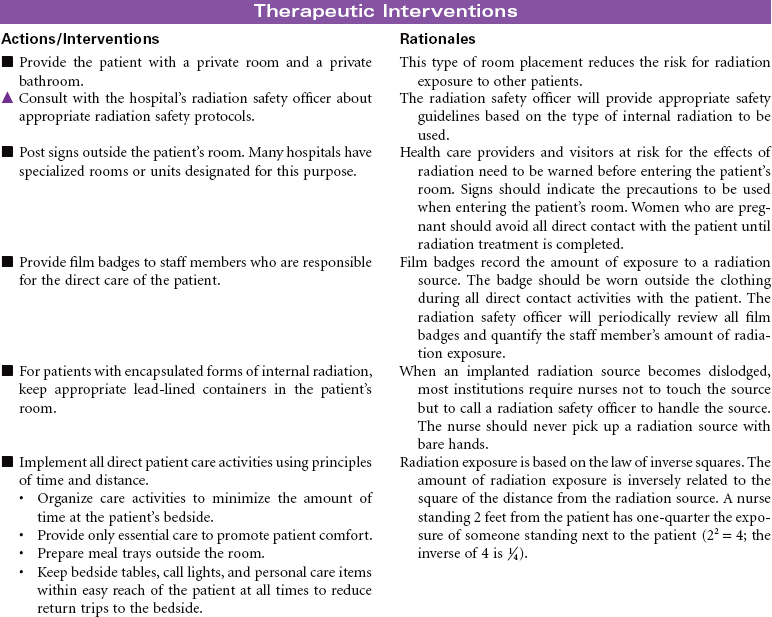
 Risk for Injury (Radiation Exposure)
Risk for Injury (Radiation Exposure)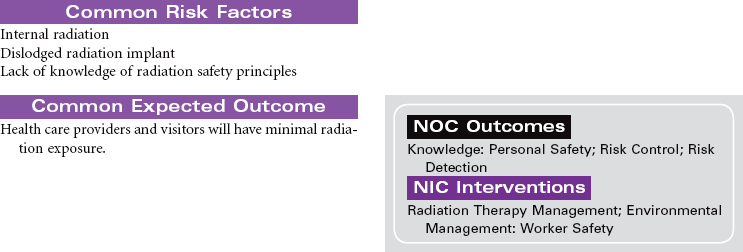
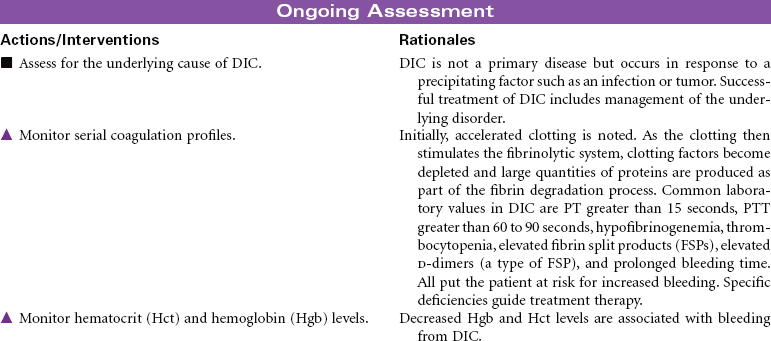
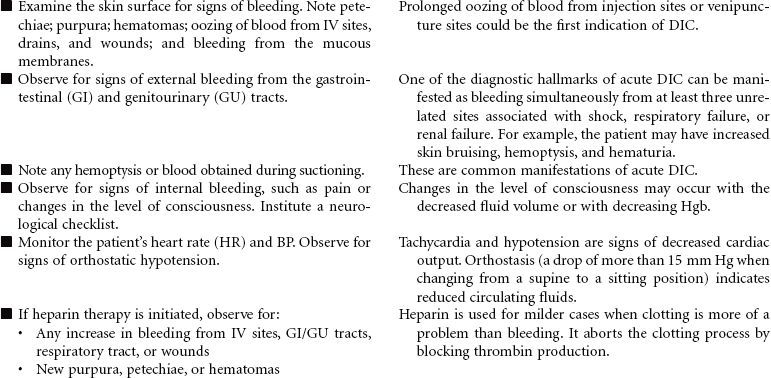
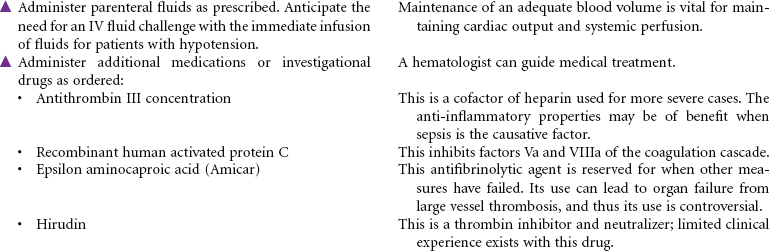
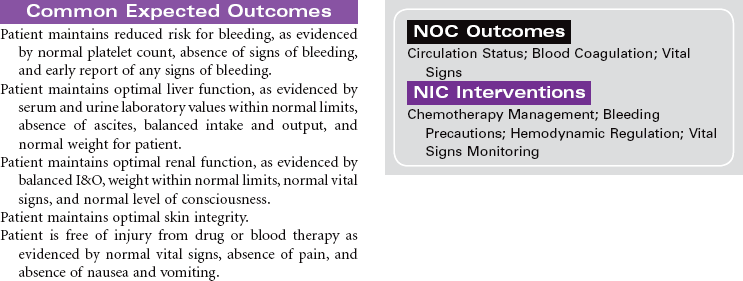
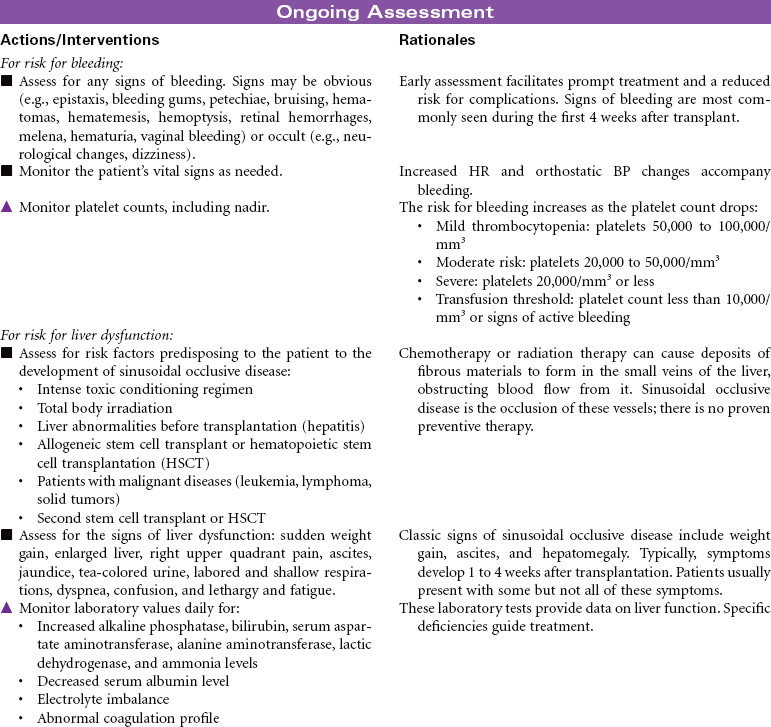
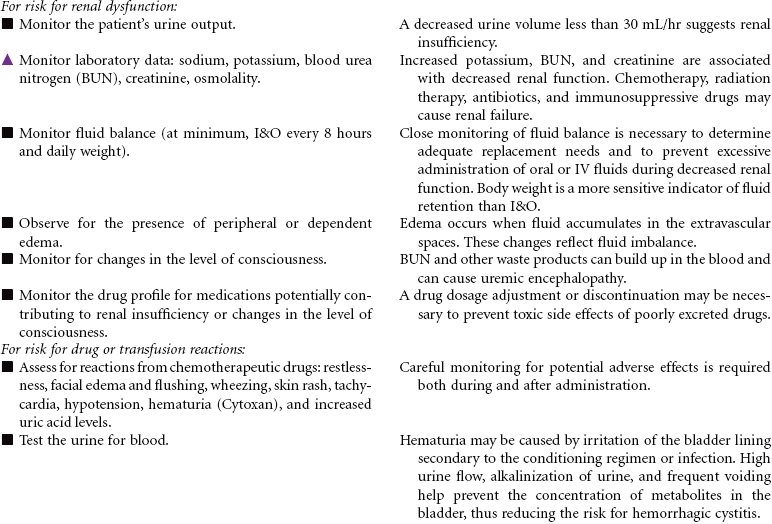
 Risk for Bleeding
Risk for Bleeding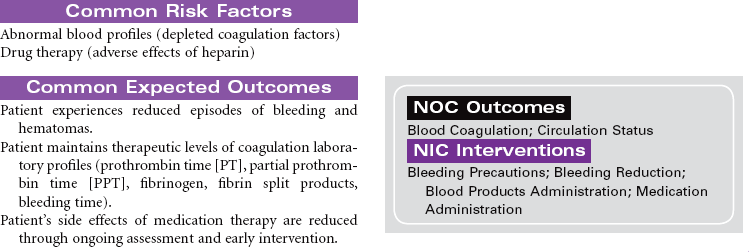
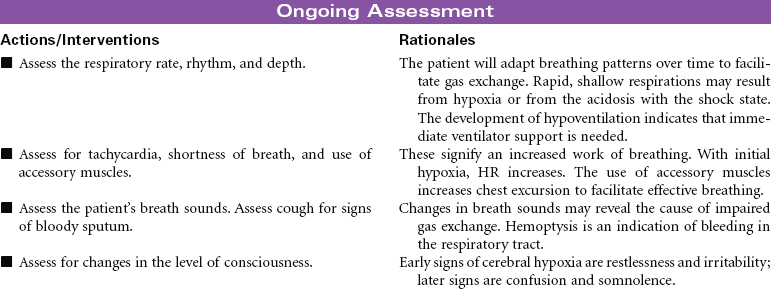
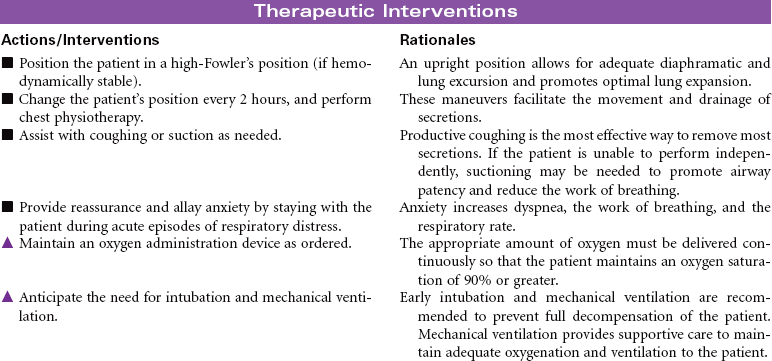
 Impaired Gas Exchange
Impaired Gas Exchange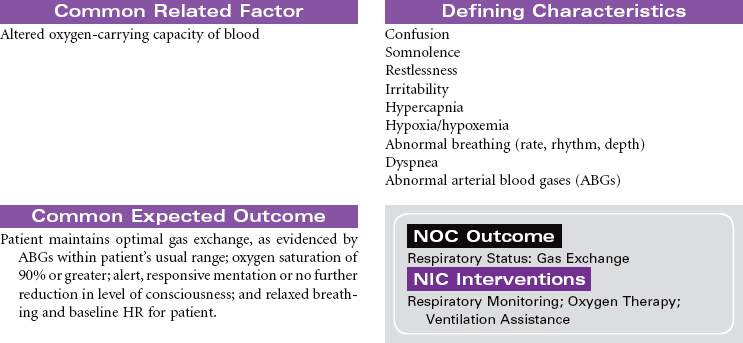

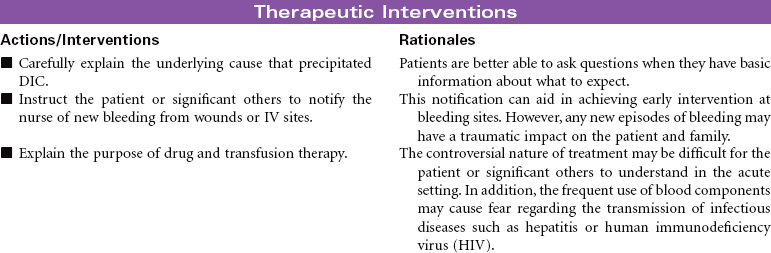
 Deficient Knowledge
Deficient Knowledge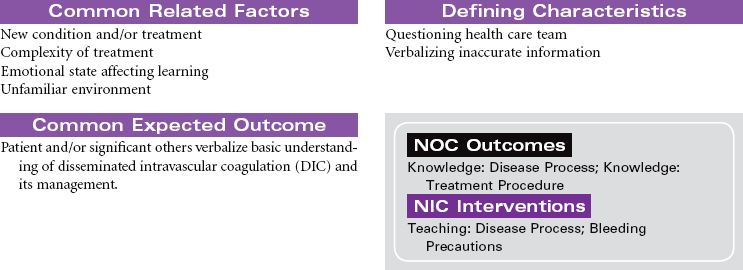

 Deficient Knowledge
Deficient Knowledge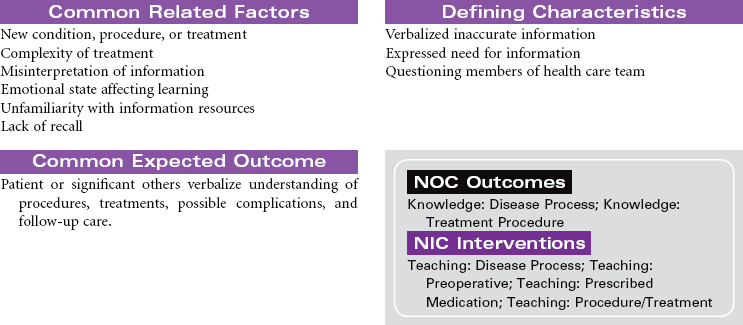


 Risk for Infection
Risk for Infection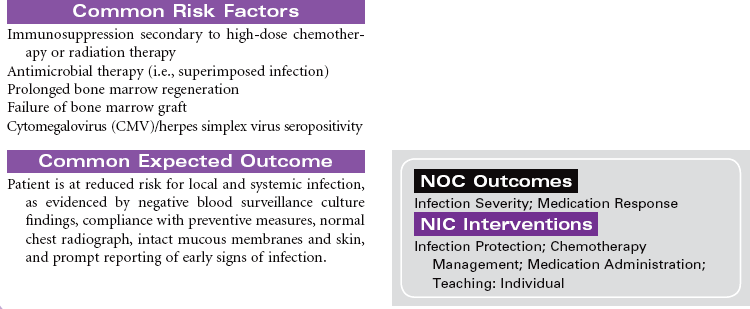
 Ineffective Protection
Ineffective Protection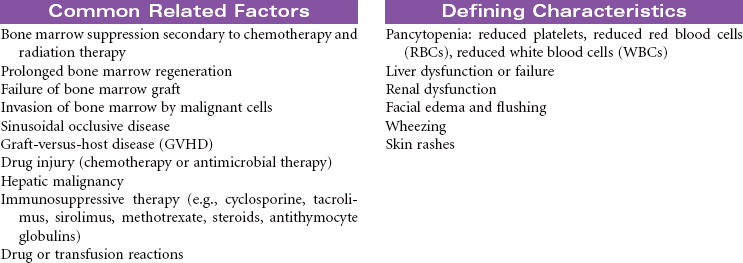
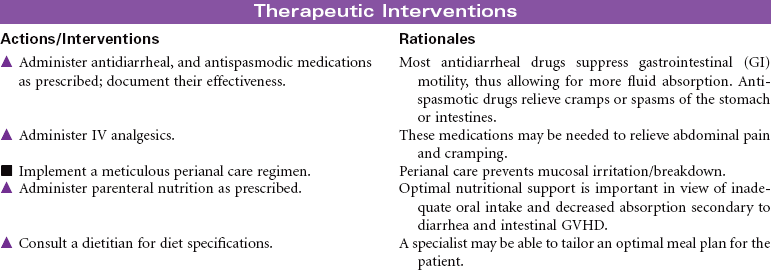
 Diarrhea
Diarrhea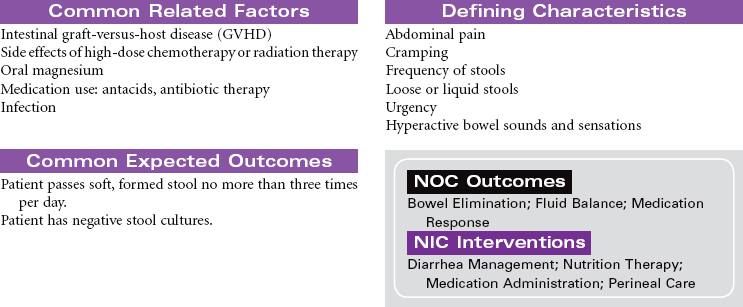


 Risk for Imbalanced Nutrition: Less Than Body Requirements
Risk for Imbalanced Nutrition: Less Than Body Requirements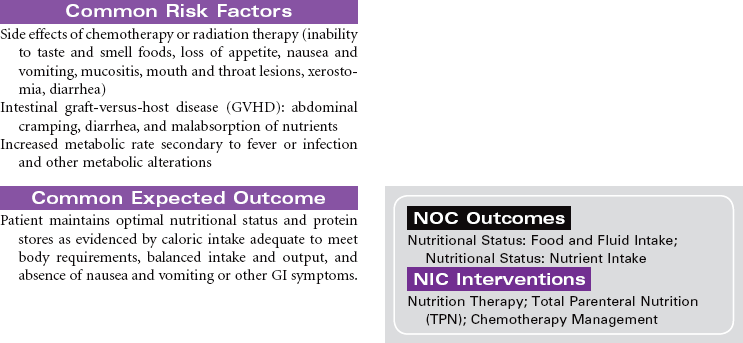
 Deficient Knowledge: Disease and Transmission
Deficient Knowledge: Disease and Transmission



Get Clinical Tree app for offline access
