Clients Experiencing Abuse and Violence
Please, Mom and Dad
My hands are small—I don’t mean to spill my milk.
My legs are short—please slow down so I can keep up with you.
Don’t slap my hands when I touch something bright and pretty—I don’t understand.
Please look at me when I talk to you—it lets me know you are really listening.
My feelings are tender—don’t nag me all day—let me make mistakes without feeling stupid.
Don’t expect the bed I make or the picture I draw to be perfect—just love me for trying.
Remember I am a child not a small adult—sometimes I don’t understand what you are saying.
I love you so much. Please love me just for being me—not just for the things I can do.
—J. Richardson & J. Richardson, Poster Funded by Health and Rehabilitative Services, State of Florida
Learning objectives
After studying this chapter, you should be able to:
Identify risk factors that create an environment in which the abuse of a child may occur.
Differentiate between child abuse and child neglect, and cite an example of each.
Recognize at least five common physical findings indicating physical abuse of a child.
Explain at least four causative factors related to domestic violence.
Discuss the dynamics of intimate partner or spousal abuse.
Differentiate among sexual harassment, sexual assault, rape, and statutory rape.
Articulate the dynamics of rape-trauma syndrome.
Explain ways in which elderly persons are abused.
Construct a profile of an individual who may become violent in the work setting.
Describe the emotional and behavioral reactions of the following victims of physical abuse or domestic violence: children, women, men, and the elderly.
Develop an assessment tool for the following clients: a victim of child abuse, an elderly victim of domestic violence, and a teen-aged victim of rape.
Key Terms
Abduction
Abuse
Attempted rape
Child abuse
Discipline
Domestic violence
Emotional abuse
Emotional neglect
Family violence
Hate crime
Incest
Intimate partner violence
Munchausen’s syndrome by proxy
Neglect
Rape
Rape-trauma syndrome
Sexual abuse
Sexual coercion
Sexual harassment
Sexual misuse of a child
Shaken baby syndrome
Silent rape syndrome
Sodomy
Stalking
Statutory rape
Violence
Workplace violence
Much has been written and a great deal of public concern has been expressed about the physical or sexual abuse of children, women, and the elderly. In addition, youth and workplace violence, as well as hate crimes, have been recognized as serious and widespread public health problems affecting individuals of all ethnic and socioeconomic backgrounds. Consider the following stories recently covered by the news media:
High school teacher accused of child abuse and pornography
Young minister killed by wife
KKK demonstration spurs riot
Estranged husband suspected of murder of wife, three children, and mother-in-law
Lacrosse players accused of gang rape of exotic dancer
Friends of 81-year-old female illegally withdrew $30,000 from her bank account
Angry postal worker kills fellow employees in mailroom
Abduction of 14-year-old female recorded on surveillance camera
Youth kills six and commits suicide at Minnesota house party
Although epidemiologic studies have shown that aggressive or abusive behavior may occur in adults with the diagnosis of schizophrenia, affective disorder, post-traumatic stress disorder, and personality disorders, recent research has shown that the vast majority of people who are abusive or who commit violent acts do not suffer from mental illness. A certain small subgroup of people, such as clients with neurologic impairment due to head injury; a disease such as Huntington’s chorea; or a psychotic disorder are at risk of becoming abusive or violent (eg, threatening, hitting, fighting, or otherwise hurting another person). However, the conditions likely to increase the risk of violence are the same whether a person has a mental illness or not (American Psychiatric Association [APA], 2003).
This chapter discusses the etiology of abuse and violence. General topics include child abuse, domestic violence or intimate partner violence, adult sexual abuse, elder abuse, youth violence, workplace violence, and hate crimes. Although the focus of domestic violence and sexual abuse is primarily on women, information about male victims is incorporated when appropriate. The chapter concludes with an application of the nursing process to victims of abuse and violence.
Abuse
The term abuse is used in psychiatric–mental health nursing to describe behaviors in which an individual misuses, attacks, or injures another individual. Abuse may be sexual, physical, or emotional. Neglect is also a form of abuse. The term violence is used to describe behaviors in which an individual displays an intensive destructive or uncontrolled force to injure a person (Sadock & Sadock, 2003; Shahrokh & Hales, 2003). Examples of abuse and violence were cited in the introduction to this chapter.
Elements of Abuse
Three elements generally create the environment for an incident of abuse to occur: the abuser or perpetrator, the abused, and a crisis.
The Abuser
A profile of abusive individuals has been described by several agencies such as the National Coalition Against Domestic Violence (NCADV) and the National Center for Injury Prevention and Control (NCIPC). The abuser, or perpetrator, is usually an individual who grew up in an abusive family. Research findings indicate that children
who observed or were victims of beatings and violence when young believe that abuse is normal behavior and will reenact these behaviors later as adults.
who observed or were victims of beatings and violence when young believe that abuse is normal behavior and will reenact these behaviors later as adults.
Statistically, abusive individuals usually are young and live in lower socioeconomic environments; however, those individuals who live in higher classes are not immune. Perpetrators of intimate partner abuse or domestic violence are generally male, whereas perpetrators of child abuse are generally female. Both male and female perpetrators abuse the elderly. Common characteristics of abusive individuals include low self-concept, immaturity, fear of authority, lack of skills to meet their own emotional needs, belief in harsh physical discipline, and poor impulse control. Abusers lack parenting or relationship skills and often use alcohol or other substances to cope with stress. In the event of child or elder abuse, the partner, who usually knows about the abuse, either ignores it or may even participate in it (NCADV, 2003; NCIPC, 2006a.)
The Abused
Abused individuals often demonstrate a pattern of learned helplessness, manifest characteristics of low-self esteem and shame, and often experience feelings of increased dependence, isolation, guilt, and entrapment (NCADV, 2003; Quillian, 1995).
A Crisis
A crisis (eg, loss of job, divorce, illness, death in the family) is usually the precipitating event that sets the abusive person into action. The individual overreacts because he or she is unable to cope with numerous or complex stressors. The person becomes frustrated and anxious and suddenly loses control. (Chapter 13 discusses crisis intervention.)
Child Abuse
The Child Abuse Prevention and Treatment Act (CAPTA), enacted in 1974, and reauthorized in 1996, provides federal funding to states to prevent, identify, and treat the abuse and neglect of children and adolescents. Child abuse, also referred to as maltreatment, is described as any recent act or failure to act, resulting in imminent risk of serious physical harm or death, emotional harm, sexual abuse, neglect, or exploitation of a child under the age of 18 years by a parent, caretaker, or other person (CAPTA, 2003). Bullying is the most common form of abuse children and adolescents experience. It is estimated that 160,000 students in American schools are absent every day because of fear of being bullied either physically or verbally (Voors, 2004). Child abuse is not to be confused with discipline. Discipline is a purposeful action to restrain or correct a child’s behavior. It is done to teach, not to punish, and it is not designed to hurt the child or result in injury. Neglect is an act of omission and refers to a parent’s or other person’s failure to meet a dependent’s basic needs such as proper food, clothing, shelter, medical care, schooling, or attention; provide safe living conditions; provide physical or emotional care; or provide supervision, thus leaving the child unattended or abandoning him or her.
Children are also victims of intimate partner or family violence (eg, one parent kills the other), school violence (eg, a child brings a gun to school and kills a teacher), or public violence (eg, the terrorist attack on the World Trade Center and Pentagon on September 11, 2001).
The World Health Organization, Regional Office for Africa (WHO/AFRO) estimates that 40 million children younger than 15 years fall victim to various forms of child abuse and violence each year. The WHO subcategorizes child abuse into physical abuse, physical neglect or abandonment, emotional abuse, and sexual abuse including commercial or other forms of exploitation that cause actual or potential harm to the child’s health, survival, development, or dignity (WHO/AFRO, 2002).
According to the NCIPC, an estimated 906,000 children in the United States experienced or were at risk for child abuse or violence in the year 2002, compared with 879,000 children in the year 2000. Of the 906,000 children:
61% experienced neglect
19% were physically abused
10% were sexually abused
5% were emotionally or psychologically abused.
Statistics provided by the NCIPC confirm that 1,500 children died from maltreatment: 36% from neglect, 28% from physical abuse, and 29% from multiple maltreatment types. In 2003, children younger than 4 years accounted for 79% of child maltreatment fatalities.
Etiology of Child Abuse
The etiology associated with child abuse is complex. Child abuse can occur mainly within the family, where the abusers are parents or parent substitutes; in the institutional setting, such as daycare centers, child-care
agencies, schools, welfare departments, correctional settings, and residential centers; in society, which allows children to live in poverty or to be denied the basic necessities of life; or as a result of war. In times of war, children are exposed to various forms of abuse and violence. They may experience traumas that can interrupt their development, trigger serious psychiatric disorders, or predispose them to delinquency and life-long crime (WHO/AFRO, 2002).
agencies, schools, welfare departments, correctional settings, and residential centers; in society, which allows children to live in poverty or to be denied the basic necessities of life; or as a result of war. In times of war, children are exposed to various forms of abuse and violence. They may experience traumas that can interrupt their development, trigger serious psychiatric disorders, or predispose them to delinquency and life-long crime (WHO/AFRO, 2002).
Anyone can abuse or neglect a child under certain circumstances, such as stress due to illness, marital problems, financial difficulties, or parent–child conflict. Parents or other persons may lose control of their feelings of anger or frustration and direct such feelings toward a child.
Characteristics of Potentially Abusive Parents
No physical characteristics automatically identify the potential child abuser. The person may be rich or poor, of any racial origin, male (40.7%) or female (59.3%), and living in a rural area, a suburb, or a city.
Box 33.1: Profile of Potentially Abusive Parents
Denial of pregnancy by a mother who has made no plans for the birth of the child and refuses to talk about the pregnancy
Depression during pregnancy
Fear of delivery
Lack of support from husband or family
Undue concern about the unborn child’s gender and how well it will perform
Fear that the child will be one of too many children
Birth of an unwanted child
Indifference or a negative attitude toward the child by the parent after delivery
Resentment toward the child by a jealous parent
Inability to tolerate the child’s crying; viewing child as being too demanding
Parents who are potentially abusive often display characteristic warning signs. However, evidence of these signs does not automatically imply that abuse will inevitably occur. Box 33-1 highlights some of the typical warning signs. Such characteristics displayed for a short time may indicate anxiety in a new mother or father. However, if the characteristics persist, the parent should seek help.
Characteristics of an Abused Child
The abused or neglected child is usually younger than 6 years, is more vulnerable to abuse than others, and may have a physical or mental handicap. Emotionally disturbed, temperamental, hyperactive, or adopted children also demonstrate a higher incidence of abuse. Children with congenital anomalies or chronic medical conditions are also at risk for abuse because of the demands of care placed on the parents or caretakers. The child, in an attempt to get attention, unintentionally may irritate the parent, leading to a loss of control in the parent and possible reactions with abuse.
Classifications of Child Abuse
Abuse of children usually is classified as physical abuse; child neglect; emotional abuse or neglect; and sexual abuse.
Physical Abuse of a Child
Physical abuse of a child involves the infliction of bodily injury that results from punching, beating, kicking, biting, burning, shaking, or otherwise harming a child. Indicators of actual or potential physical abuse have been categorized as physical, behavioral, and environmental, briefly discussed in the following sections (Figure 33-1).
Physical Indicators
The most common indicators of physical abuse of a child are bruises involving no breaks in skin integrity. The bruises are usually seen on the posterior side of the body or on the face, in unusual patterns or clusters, and in various stages of healing, making it difficult to determine the exact age of a bruise. Burns also are seen frequently, and usually are due to immersion in hot water, contact with cigarettes, tying with a rope, or the application of a hot iron. Common burned areas include the buttocks, palms of hands, soles of feet, wrists, ankles, or genitals. Lacerations, abrasions, welts, and scars may be noted on the lips, eyes, face, and external genitalia.
Other indicators of physical abuse include missing or loosened teeth; skeletal injuries such as fractured bones, epiphyseal separation, or stiff, swollen, enlarged
joints; head injuries; and internal injuries. Such bodily injuries must be evaluated with respect to the child’s medical history, developmental ability to injure self, and behavioral indicators (which are discussed later in this chapter).
joints; head injuries; and internal injuries. Such bodily injuries must be evaluated with respect to the child’s medical history, developmental ability to injure self, and behavioral indicators (which are discussed later in this chapter).
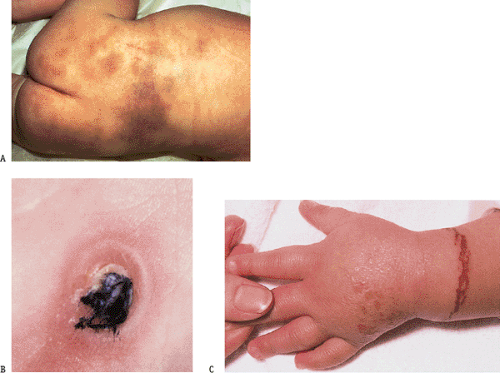 Figure 33.1 Examples of child abuse: (A) bruising on a child’s body, (B) cigarette burns, (C) rope burn. (Source: Pillitteri, A. [2003]. Maternal and child health nursing [4th ed.]. Philadelphia: Lippincott Williams & Wilkins. ) |
Munchausen’s Syndrome by Proxy
Munchausen’s syndrome by proxy is now a well-known phenomenon in which the biologic mother (90%), the biologic father (5%), or a female caregiver (5%) systematically fabricates—or deliberately causes—illness or injury in the child in order to gain sympathy or attention for themselves (Thomas, 2003). The perpetrators have well-developed plans and act with malevolent intent to satisfy craving for medical attention and psychological gain. Forms of fabricated or caused illnesses include poisonings, seizures, apparent bleeding from a variety of orifices, skin rashes, and pyrexia (Quisenberry, 2006; Skuse & Bentovim, 1994). Usually, the child is brought in for frequent and persistent medical examinations. However, when the child is separated from the parent, acute symptoms and the signs of illness cease. The perpetrator denies having any knowledge of the cause of the disorder. Comorbidity is a major problem because it is highly likely that the child will have more than one fabricated illness. Failure to thrive and nonaccidental injuries are also commonly noted. Approximately 21.8 months lapse from symptom presentation to definitive diagnosis. This
allows ample time for substantial morbidity to occur while unnecessary tests and surgical procedures take place. The average age of death is at 18.8 months (Quisenberry, 2006; Sheridan, 2003).
allows ample time for substantial morbidity to occur while unnecessary tests and surgical procedures take place. The average age of death is at 18.8 months (Quisenberry, 2006; Sheridan, 2003).
Shaken Baby Syndrome
Shaken baby syndrome is a form of child abuse affecting between 1,200 and 1,600 children every year and is the leading cause of brain injury to infants (NCIPC, 2006a). It occurs when an adult loses control and violently shakes a child who has been crying incessantly. This syndrome has been documented in children up to 5 years of age. An estimated 20% to 25% of infant victims die from their injuries. The physical findings usually include bruising from being grabbed firmly, and major head injury such as subdural hematoma or cerebral edema. Nonfatal consequences include blindness due to retinal hemorrhage, cerebral palsy, and cognitive impairment (Brasseur, 1995; NCIPC, 2001).
Behavioral and Environmental Indicators
Behav-ioral indicators of physical abuse depend on the age at which the child is abused, as well as the frequency and the severity of abuse. The behavioral profile of a physically abused child is presented in Box 33-2. If a child exhibits such behaviors, observation for bodily injuries is crucial.
Box 33.2: Behavioral Profile of a Physically Abused Child
Fear of parents and fear of physical contact with adults
Extremes in behavior such as passivity or aggressiveness, or crying very often or very seldom
Sudden onset of regressive behavior such as thumb sucking, enuresis, or encopresis
Learning problems that cannot be diagnosed
Truancy from school or tardiness
Fatigue causing the child to sleep in class
Inappropriate dress to hide burns, bruises, or other marks of abuse
Inappropriate dress, resulting in frostbite or illness due to exposure to inclement weather
Excessive compliance to avoid confrontation
Sporadic temper tantrums
Violence toward other children or animals
Demanding behavior
Clinical Example 33.1: The Physically Abused Child
KW, the 22-year-old boyfriend of JN, was accused of beating JN’s 5-year-old daughter severely enough to cause permanent brain damage. The child was beaten with a stick and forced to drink dishwashing liquid because she was “too sassy.” After the beating, the child was kept on the floor of the apartment because she appeared to be unconscious at times. JN force-fed her daughter oatmeal and bananas in an effort to revive her. Two days later, the child was taken to the hospital and was found to have burn marks on her buttocks, a head injury, and bruises on her body. JN was charged with child abuse, and KW was sentenced to 15 years in prison for aggravated child abuse.
Environmental indicators of potential physical abuse in children include severe parental or caretaker problems such as drug addiction, alcoholism, and mental illness; crisis; and geographic or social isolation of the family. See Clinical Example 33-1: The Physically Abused Child.
Child Neglect
Child neglect is the failure to provide for a child’s basic physical, medical, or educational needs. Examples of child neglect include withholding shelter, adequate nutrition, adequate clothing, access to education, and proper medical or dental care. Abandonment of a child or lack of adequate supervision also constitutes neglect. However, financial status, cultural values, and parental capacity must be considered before a parent or adult is accused of neglecting a child.
Physical Indicators
Potential physical indicators of child neglect may include weight loss resulting from inadequate nutrition, dental caries caused by lack of appropriate nutrition or dental care, or symptoms of an undiagnosed medical condition such as anemia or pneumonia. The child may also look unkempt and lack adequate clothing (eg, no shoes or adequate clothing for seasonal weather changes).
Behavioral and Environmental Indicators
Behavioral indicators of child neglect commonly seen include failure to thrive; learning difficulties caused by poor attention span, inability to concentrate, or autistic behavior; use of drugs or alcohol; delinquency; and sexual misconduct. Environmental indicators of child neglect by parents or caretakers include living in poverty; the presence of a large family with marital conflict; lack of material resources; or the lack of positive parental attitudes. Parents or caretakers may lack an adequate understanding of the developmental stages of childhood; fail to recognize physical or emotional needs of children; display a lack of interest in childhood activities; display poor parenting skills; or exhibit a lack of interest in personal hygiene. See Clinical Example 33-2: The Neglected Child.
Emotional Abuse or Neglect
Emotional abuse consists of verbal assaults or threats that provoke fear; poor communication that may send double messages; and blaming, confusing, or demeaning messages. Parents or caretakers who emotionally abuse children may tell the child that she or he is unwanted, unloved, or unworthy of care. The child may become the scapegoat of the family (ie, accused of causing family problems).
Conversely, emotional neglect, considered to be a form of child neglect discussed earlier, occurs when parents or other adults responsible for the child fail to provide an emotional climate that fosters feelings of love, belonging, recognition, and enhanced self-esteem. Examples of emotional neglect include ignoring the child, providing minimal human contact, and failing to provide opportunities to foster growth and development. Children who are emotionally abused or neglected may develop serious behavioral, cognitive, emotional, or mental disorders.
Clinical Example 33.2: The Neglected Child
FR, a young, single working mother, entrusted the care of her 1- and 2-year-old children to her 8-year old daughter while she worked as a waitress from approximately 7:00 PM to midnight. Before she left for work each evening, FR locked the younger children in their bedrooms and instructed the older daughter to stay indoors and “keep an eye on the children.” One evening, a fire began on the second floor of the apartment, killing the two younger children by smoke inhalation. The 8-year-old was able to escape the fire. FR told the authorities she made minimum wage and was unable to afford to pay a babysitter, so she worked at night while her older daughter was home.
Behavioral and Environmental Indicators
The emotionally abused or neglected child often develops a low self-concept as he or she hears negative comments such as “If it weren’t for your bad habits, Daddy wouldn’t leave us!,” “It’s all your fault we don’t have enough money. You’re sick all the time,” and “The family got along fine until you started to act so selfish.” Behavioral indicators of an emotionally abused or neglected child are listed in Box 33-3.
Examples of environmental indicators of emotional abuse or neglect of a child include inadequate parenting skills; rejection or immature behavior by parents or caretakers; continuous friction or conflict in the home; discriminatory treatment of the children in the family; and abuse of drugs or alcohol by the parents or caretaker.
Child Sexual Abuse
Sexual abuse of a child includes fondling of a child’s genitals, intercourse, incest, rape, sodomy, exhibitionism, and commercial exploitation through prostitution or the production of pornographic materials. Child
sexual abuse is four times higher among female than male victims (NCIPC, 2002).
sexual abuse is four times higher among female than male victims (NCIPC, 2002).
Box 33.3: Behavioral Indicators of an Emotionally Abused or Neglected Child
Stuttering
Enuresis or encopresis
Delinquency, truancy, or other disciplinary problems
Hypochondriasis
Autism or failure to thrive
Overeating
Childhood depression
Suicide attempts
According to a 2001 study funded in part by the U.S. Department of Justice, titled “The Commercial Exploitation of Children in the U.S., Canada, and Mexico,” approximately 300,000 to 400,000 U.S. children are victims of some type of sexual exploitation, particularly commercial sexual exploitation, every year (CNN.com, 2001). Sexual abuse has serious direct consequences such as emotional distress, behavioral problems, sexually transmitted diseases (STDs), unwanted pregnancies, and indirect consequences such as the development of a substance-use disorder, mood disorder, sexual deviance, or difficulty in establishing a satisfying intimate relationship later in life. Sexual abuse of a child is not easy to identify because the physical signs of abuse usually are not seen outside a clinical or medical setting. The child victim is usually reluctant to share information about the abuse because the child fears she or he may alienate or anger the person who provides food, shelter, and a family bond.
Children at high risk for sexual abuse include those who:
Are 3 years of age or younger
Suffer from a developmental delay
Live in a home where substance abuse occurs
Have adolescent parents or a single parent
Are in foster care
Have primary caretakers who were sexually abused themselves
Have primary caretakers who are mentally ill or who have a developmental delay
Classifications of Child Sexual Abuse
Episodes of childhood sexual abuse are classified as acute, subacute, or nonacute. Acute episodes include cases of sexual abuse that have occurred within the previous 72 hours of examination by a clinician. Evidence of moderate-to-severe injury, such as vaginal bleeding or genital lacerations, may be present. Subacute episodes involve sexual abuse cases that have occurred more than 72 hours before an examination by a clinician. Symptoms such as minor abrasions or dysuria may be present. Nonacute episodes also involve sexual abuse cases that occur more than 72 hours before a clinician’s examination; however, there are no significant injuries or symptoms.
Box 33-4 lists physical and behavioral indicators of a sexually abused child. Clinical Example 33-3 describes a case of sexual abuse by a father.
Box 33.4: Indicators of a Sexually Abused Child
Physical Indicators
Itching, pain, bruises, or bleeding in the external genitalia, vagina, or anal area
Edema of the cervix, vulva, or perineum
Torn, stained, or bloody undergarments
Stretched hymen at a very young age
Presence of semen or a sexually transmitted disease
Pregnancy in an older child
Bladder infections
Behavioral Indicators
Fear of being touched
Difficulty walking or sitting
Reluctance to participate in recreational or physical activities
Poor peer relationships
Delinquency, truancy, acting-out, or running away
Preoccupation with sexual organs of self or others (in younger children)
Sexual promiscuity or prostitution (in older children)
Change in sleeping patterns; nightmares; or sudden fear of falling asleep
Bed-wetting or thumb-sucking (inappropriate to age)
Use of drugs and alcohol
Terminology of Child Sexual Abuse
Three terms are frequently used to describe the sexual abuse of children: sexual misuse, rape, and incest. Sexual misuse of a child is defined as sexual activity that is inappropriate because of the child’s age, development, and role within the family unit. Examples include fondling, genital manipulation, voyeurism, or exhibitionism.
Rape refers to actual penetration of an orifice of a child’s body during sexual activity. Oral penetration is the most frequent type of penetration experienced by very young children.
Incest, defined as sexual intercourse or sexual behaviors that occur between family members who are so closely related as to be legally prohibited from marrying one another because of consanguinity (ie, they share the same ancestry and are referred to as “blood relatives”), is usually a well-guarded secret.
Approximately 100,000 cases of incest occur each year, but fewer than 25% are reported, according to statistics provided in the year 2000 by the American Academy of Child and Adolescent Psychiatry and the National Center on Child Abuse and Neglect. Victims of incest are usually very young. The average age of an incest victim is 11 years, although most child victims experience their first incestuous encounter between the ages of 5 and 8 years.
Approximately 100,000 cases of incest occur each year, but fewer than 25% are reported, according to statistics provided in the year 2000 by the American Academy of Child and Adolescent Psychiatry and the National Center on Child Abuse and Neglect. Victims of incest are usually very young. The average age of an incest victim is 11 years, although most child victims experience their first incestuous encounter between the ages of 5 and 8 years.
Clinical Example 33.3: The Sexually Abused Child
CB, a 6-year-old girl, daughter of a well-liked and respected member of the community, was forced by her father to have oral sex with him when her mother was away at club meetings. The sexual encounters lasted a few months and had a profound effect on CB, whose parents divorced when she was 14. She loved her father but also hated him and swore that she would never tell anyone about the incest. A few years after CB married, her deteriorating sexual relationship with her husband prompted her to admit the incest and to seek therapy.
Child Abduction
Abduction or kidnapping occurs whenever a person is taken or detained against his or her will. Statistics reported by the Department of Justice in 2002 indicate that every 40 seconds in the United States, a child is reported missing or abducted. That statistic translates to more than 2,000 missing children per day or 800,000 per year. Approximately 69,000 of the missing children are abducted (KidsFightingChance.com, 2006).
Approximately 82% of abductions are committed by family (primarily parents), occur more frequently to children under the age of 6 years, equally victimize children and adolescents of both sexes, and most often originate in the home. Non-family or acquaintance abduction accounts for 18% of reported cases, has the largest percentage of female and teen-aged victims, is more often associated with crimes such as sexual and physical assault, occurs at homes and residences, and has the highest percentage of injured victims. Stranger kidnapping accounts for 37% of non-family abductions, occurs primarily in outdoor locations, victimizes more female than male children and adolescents, is often associated with sexual assaults and robberies, and generally involves the use of a firearm (KidsFightingChance.com, 2006; Klass Kids Foundation, 2006).
Domestic or Intimate Partner Violence
Domestic violence, also referred to at times as intimate partner violence or family violence, is a public health problem of epidemic proportions that crosses racial/ethnic boundaries and socioeconomic strata. It is designed to manipulate, control, and dominate the partner to achieve compliance and dependence. Domestic violence may include repeated battering and injury, psychological abuse, sexual assault, progressive social isolation, stalking, deprivation, and intimidation. Someone (ie, spouse, ex-spouse, or significant other) who is or was involved in an intimate relationship with the victim perpetrates these behaviors.
Groups at Risk
Although 95% of domestic violence is directed at women who are emotionally involved with the batterer, children, the elderly, men, and same-sex couples are also at risk. As noted earlier, children who are raised in homes where domestic violence occurs are often victims. They are referred to as “silent victims” who are at risk for abuse and the development of emotional or behavioral problems later in life. Domestic violence between elder partners may manifest as a long-standing pattern of marital violence or originate as the result of stress that accompanies disability and changing family relationships. Studies demonstrate that when men are victims of domestic violence, women usually act out of self-defense, or the defense of their children. Statistics also indicate that domestic violence exists in same sex couples. Women living with female intimate partners experience less domestic violence than women living with men; however, men living with male intimate partners experience more domestic violence than do men who live with female intimate partners (Makar, 2000; Allen, 2006). Figure 33-2 depicts the annual national morbidity rate associated with domestic violence.
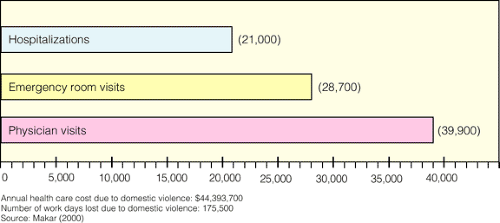 Figure 33.2 Annual national domestic violence morbidity rates reported by The National Crime Survey. |
Epidemiology
Domestic violence is the single greatest cause of injury to women. Although exact numbers of domestic violence incidents differ because this is such an underreported crime and a relatively new area of study, experts do agree on some statistics. The following statistics on domestic violence were compiled from the Journal of the American Medical Association, U.S. Department of Health and Human Services, Federal Bureau of Investigation (FBI), Medical College of Pennsylvania, and NCICP (NCIPC, 2006b; Women Against Abuse, 2003).
Nearly 5.3 million women and 3.2 million men are victims of domestic violence each year.
Approximately 1.5 million women and more than 800,000 men are raped or physically assaulted by an intimate partner.
20% of all emergency room visits by women are the result of domestic violence.
75% of women victims of domestic violence suffer additional injuries within a year.
Every 15 seconds, a woman in this country is beaten by her current or former husband or intimate partner.
In 2002, 76% of intimate partner homicide victims were female and 24% were male.
Approximately 33% of all women with children in homeless shelters cite domestic violence as the primary cause of their homelessness.
One of three teenagers reports having experienced violence in a dating relationship.
The rate of domestic violence in gay and lesbian communities is approximately 25%.
Supporting Evidence for Practice 33-1 highlights a study addressing the need for identifying potential victims of domestic violence.
Factors Contributing to Domestic Violence
Physical abuse during domestic violence involves a willful, nonaccidental attempt to injure a person by way of a direct, overtly aggressive attack. Examples of abuse during domestic violence include throwing objects at one’s husband, threatening to injure one’s wife, or physically beating a significant other. Men usually push, shove, grab, slap, hit repeatedly, torture, or threaten with a lethal object. Women hit or throw objects, use fists, kick, bite, or scratch.
Various disciplines describe factors that contribute to domestic violence toward partners, children, and elderly parents. Box 33-5 lists these identified factors.
Profiles of the Abuser and the Abused
Although perpetrators of domestic violence can be male or female, most studies focus on the male as the
abuser and the female as the abused. Professional staff who have worked with and studied men who physically abuse others have developed a profile of male abusers. Male abusers usually have low self-esteem, believing that a man should be the head of the household and have the final say in family decisions. Because of their insecurities and fears, batterers experience extreme jealousy. Because they grew up in violent homes, they have not developed positive ways to communicate feelings and needs, or the ability to compromise. They use force or violence to solve problems, typically blaming everyone and everything but themselves for their actions. Because batterers do not want to face the seriousness of their behavior and its consequences, denial is a common defense mechanism.
abuser and the female as the abused. Professional staff who have worked with and studied men who physically abuse others have developed a profile of male abusers. Male abusers usually have low self-esteem, believing that a man should be the head of the household and have the final say in family decisions. Because of their insecurities and fears, batterers experience extreme jealousy. Because they grew up in violent homes, they have not developed positive ways to communicate feelings and needs, or the ability to compromise. They use force or violence to solve problems, typically blaming everyone and everything but themselves for their actions. Because batterers do not want to face the seriousness of their behavior and its consequences, denial is a common defense mechanism.
Supporting Evidence for Practice 33.1: Identification of Potential Victims of Domestic Violence in the Primary Care Setting
Problem Under Investigation
What attitudes, beliefs, and practices regarding domestic violence do primary health care providers exhibit?
Summary of the Research
The sample consisted of 206 subjects including 33 medical students, 25 licensed practical nurses, 58 registered nurses, 6 nurse practitioners, 13 physician assistants, and 71 physicians recruited from five different primary care practices. Most of the participants were women (70%) and had been in health care for more than 10 years (72%). A self-administered questionnaire was administered and responses were grouped according to the type of clinician (eg, RN, NP, LPN). Results indicated that 10% of the sample had never identified a victim and 55% had never identified a batterer; 50% of the clinicians and 70% of the assistants believed domestic violence was rare or very rare in their practice; and 45.2% seldom or never asked about anxiety, depression, or chronic pelvic pain when evaluating an injured client. One fourth of the clinicians and approximately 50% of the assistants reported that they did not feel confident in asking about domestic violence. Few (23%) felt that they had strategies to aid victims or felt comfortable referring victims (16.2% assistants, 37.1% clinicians) or batterers (14.6% assistants, 22.4% clinicians).
Support for Practice
The identification, treatment, and referral of persons experiencing domestic violence is a priority for psychiatric–mental health nurses in any clinical setting. Furthermore, the nurse needs to develop techniques for effective management of the identified battered and batterer. Therefore, educational programs may be necessary to help nurses feel better equipped to identify potential victims and be more comfortable in asking about domestic violence. This study can serve as a guide as to the specific content that should be included in educational programs.
Source:
Sugg, N. K., Thompson, R. S., Thompson, D. C., Maiuro, R., & Rivars, R. P. (1999, Jul/Aug). Domestic violence and primary care: Attitudes, practices, and beliefs. Archives of Family Medicine, 8, 301–306.
The profile of an abused client (either male or female) includes a history of being raised in insecure living conditions, experience of abuse as a child, and getting married as a teenager. Abused women often exhibit a pattern of learned helplessness as well as characteristics of low self-esteem and shame. They may hold religious or cultural beliefs about the traditional gender roles of men and women.
Forms of Domestic Violence
Domestic violence takes many forms. In the Duluth, Minnesota, Minnesota Domestic Abuse Intervention Project, a power and control wheel was developed to serve as a teaching model for counseling groups of men who physically and emotionally abused their spouses or partners. Eight forms of abusive behavior were identified and described by women who lived with men who batter. These forms of behavior illustrate that domestic violence is part of a pattern of behavior, rather than isolated incidents of abuse or cyclical pent-up anger, frustration, or painful feelings experienced by the batterer (Medical Education Group Learning Systems, 1995). The behaviors of domestic violence include:
Intimidation (eg, using looks, action, or gestures to instill fear in the victim)
Threats (eg, threatening to do something harmful to the children, a pet, or self)
Sexual abuse (eg, forcing unwanted sexual activity on the victim)
Isolation (eg, controlling the victim’s contacts and activities)
Emotional abuse (eg, using put-downs or attacking the abused victim’s self-confidence)
Use of children (eg, using custody/visitation rights as a way to control or harass the victim)
Male privilege (eg, expecting to be waited on by the victim)
Economic abuse (eg, refusing to share money with or provide financial support for the victim)
Box 33.5: Factors Contributing to Domestic Violence
Individuals with neurologic impairments, agitated depression, antisocial or borderline behavior, or who abuse drugs and alcohol are often unable to control impulsive behavior due to increased frustration or anxiety. They are prone to committing acts of domestic violence when they are under the influence of substances.
Lack of nurturing and mothering during childhood results in the inability to nurture others as an adult.
Poor socioeconomic conditions resulting in increased stress, anxiety, or frustration may precipitate domestic violence within the family.
Poor communication skills may result in the use of verbal or physical abuse.
Specific behaviors learned during various developmental stages become part of a person’s interactions with spouse and family. For example, a child who lives in an environment in which spousal or parental abuse occurs probably will believe that domestic violence is normal unless intervention occurs to prohibit such behavior.
Domestic violence may increase after the death of a significant family member, the loss of a job, a geographic move, the onset of physical or mental illness, a developmental change, or a family change such as pregnancy or the birth of a child.
Dynamics of Domestic Violence
Three phases of domestic violence are described: the tension-building phase, the acute battering phase, and the loving phase. Domestic violence usually occurs as a result of the inability to cope with an increase in daily stressors.
Tension-Building Phase
During the tension-building phase, disagreements may occur within a couple as the battered person withdraws rather than making any attempts to display anger verbally or nonverbally. The batterer becomes possessive, jealous, and fearful, sensing the battered partner’s anger. As a result, emotional distancing occurs. The batterer rationalizes the battered partner’s nonassertiveness as acceptance and permission to vent tensions. Minor physically abusive incidents may cause the battered person to cope with abuse by somatizing, whereas the batterer attempts to reduce tension by taking drugs or drinking alcohol, further decreasing inhibitions and precipitating abusive episodes.
Acute Battering Phase
During the acute battering phase, the batterer loses control of behavior because of blind rage. The battered person also loses control and is unable to stop the physical abusiveness experienced. Both persons are in a state of shock immediately after the incident. The batterer is unable to recall his or her behavior; the battered person depersonalizes during the abusive incident and is unable to recall in detail what occurred.
Loving Phase
As both calm down, the batterer may exhibit feelings of remorse, beg forgiveness, promise not to abuse in the future, and state that he or she cannot live without the battered partner. During this loving phase, the abused person believes the batterer’s promises and forgives the batterer because the battered partner then feels less helpless. The batterer interprets such behavior as an act of love and acceptance by the battered partner.
Barriers to Leaving a Violent Relationship
According to the NCADV (2003), the reasons why women stay in a violent relationship fall into three major categories. They include lack of resources, lack of institutional responses, and traditional ideology.
Lack of Resources
Most victims of domestic violence have at least one dependent child and do not have the financial resources (eg, unemployed, lack access to cash or




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
Get Clinical Tree app for offline access
