Chapter 5
Cardiac and Vascular Care Plans
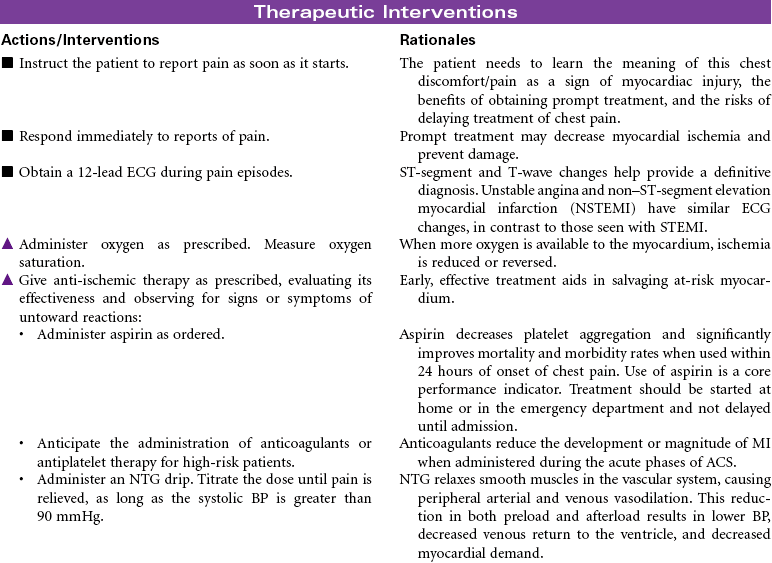
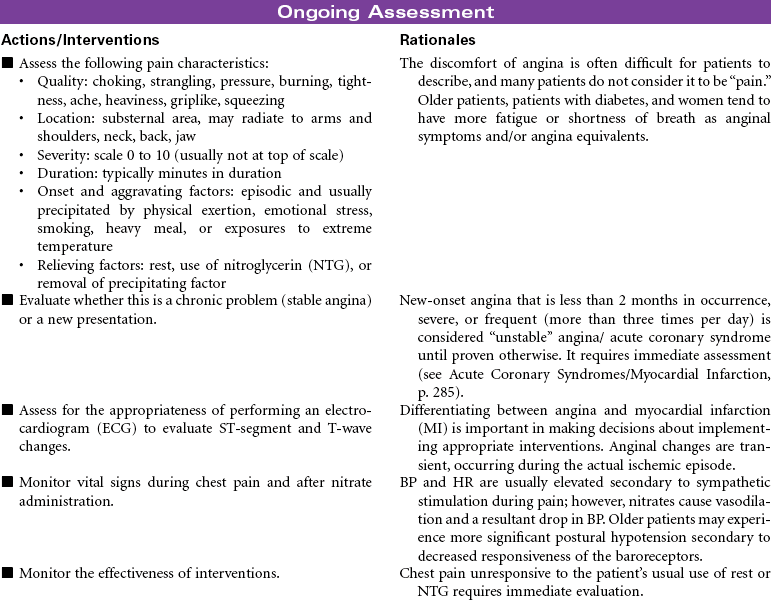
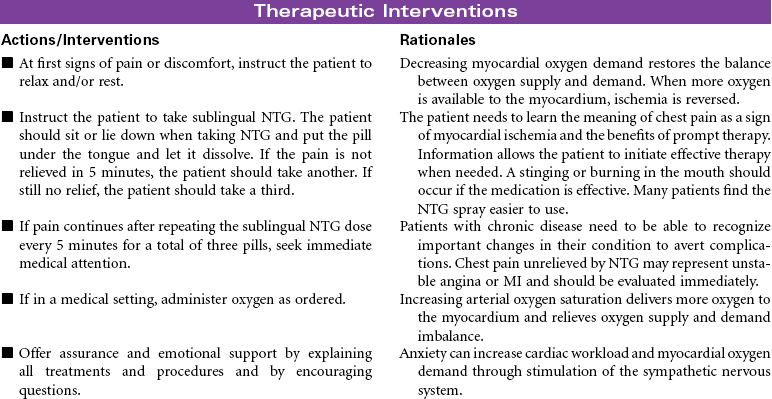
Acute Coronary Syndromes/Myocardial Infarction
 For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.
Nurse Key
Fastest Nurse Insight Engine
 = Independent
= Independent  = Collaborative
= Collaborative Acute Pain
Acute Pain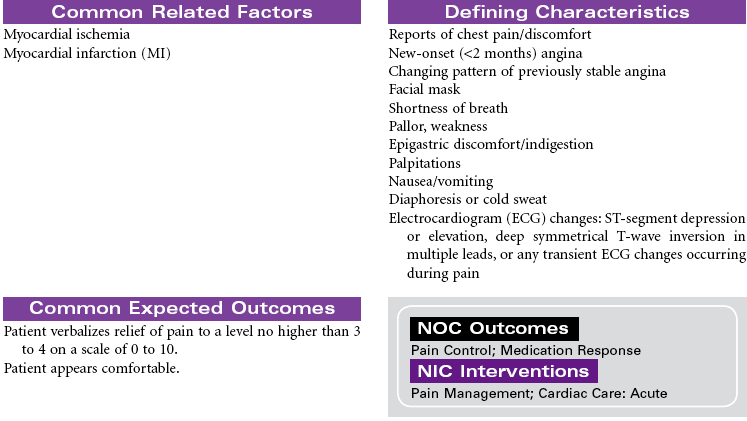
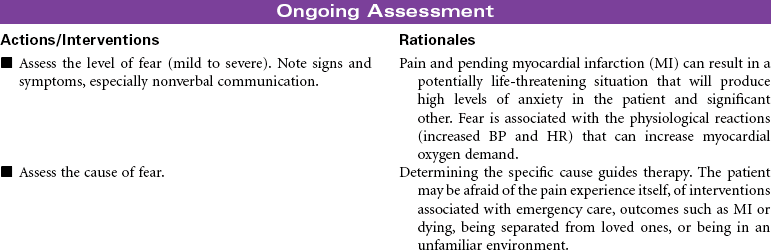
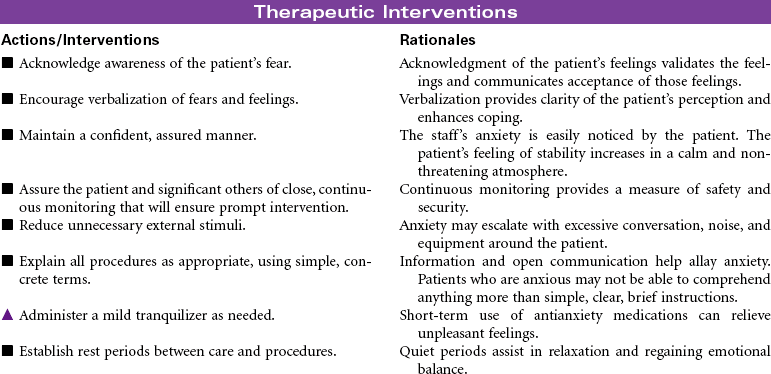
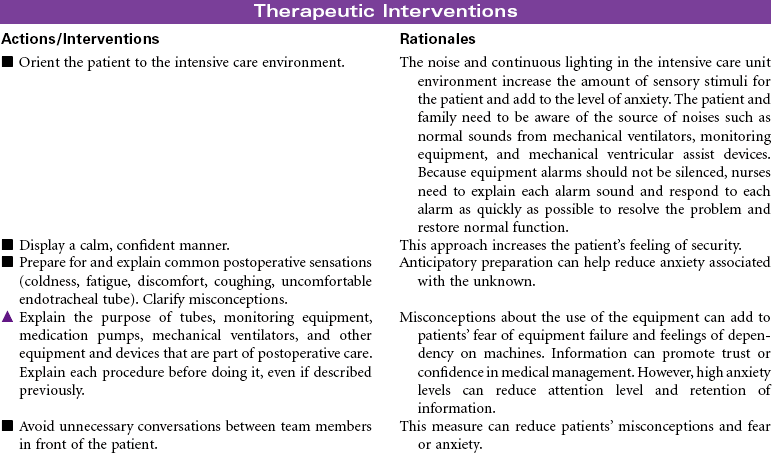
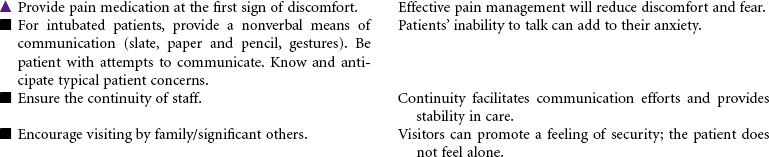
 Fear
Fear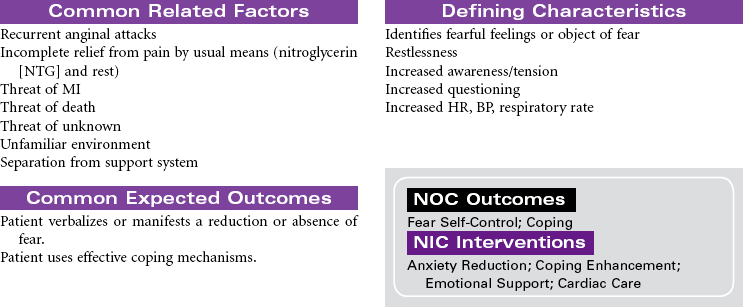
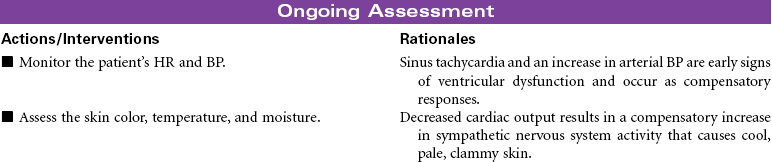
 Risk for Decreased Cardiac Output
Risk for Decreased Cardiac Output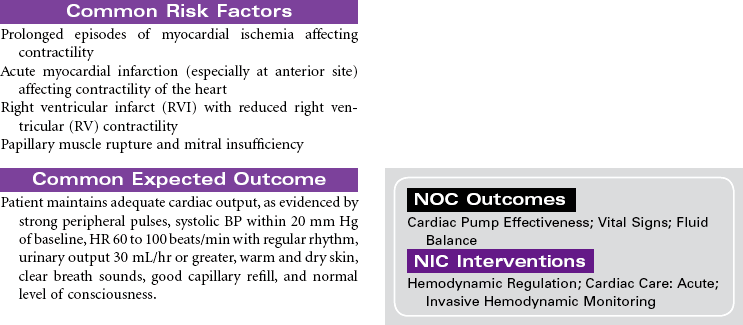

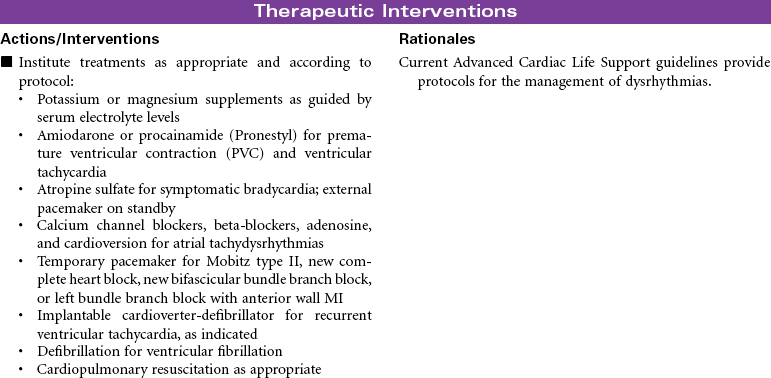
 Risk for Decreased Cardiac Output: Dysrhythmias
Risk for Decreased Cardiac Output: Dysrhythmias

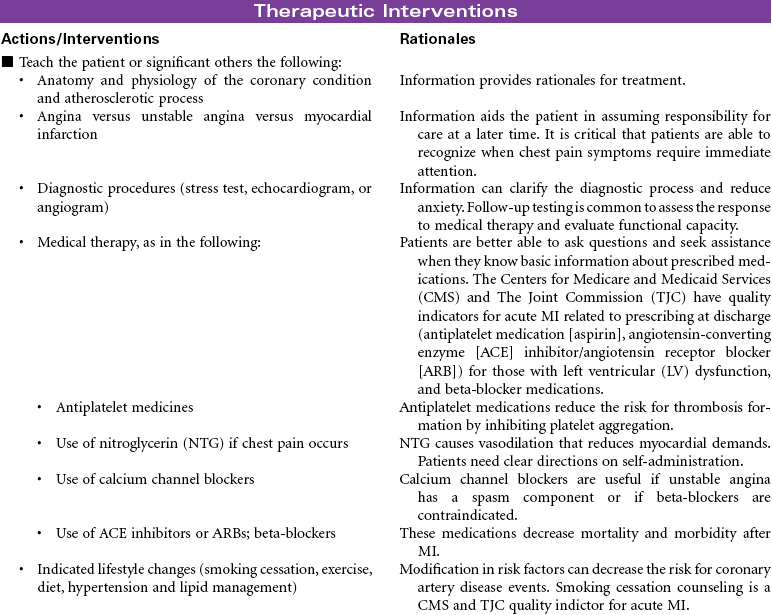
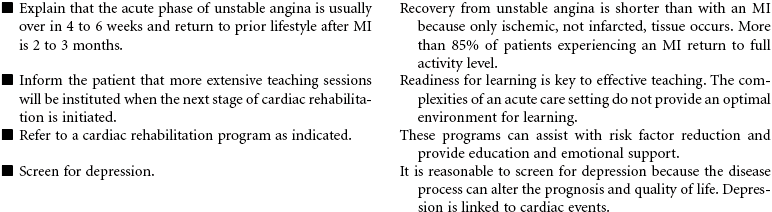
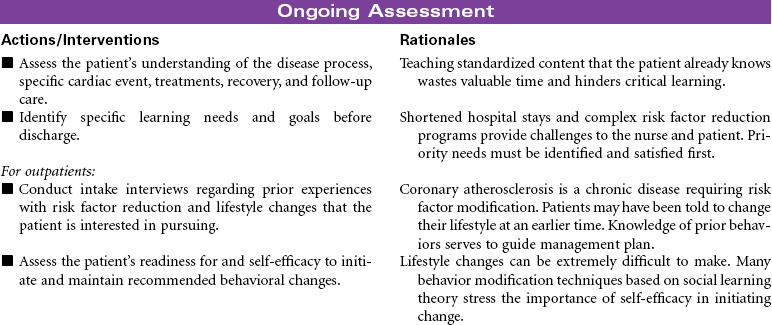
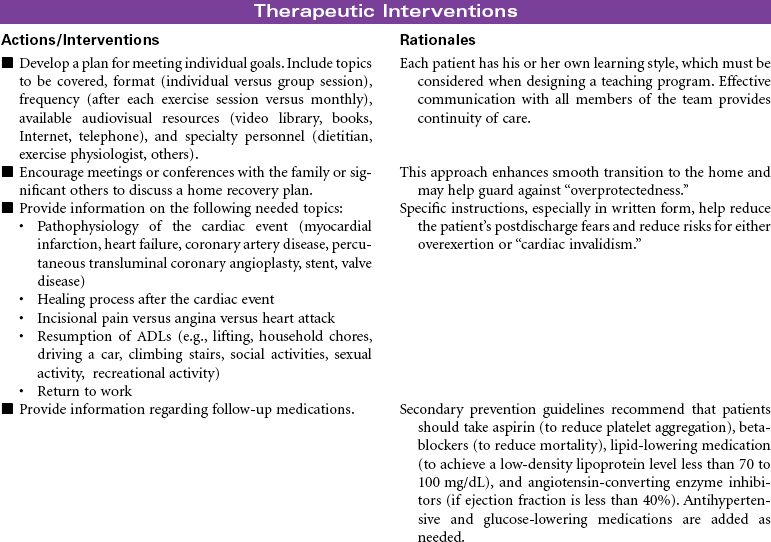
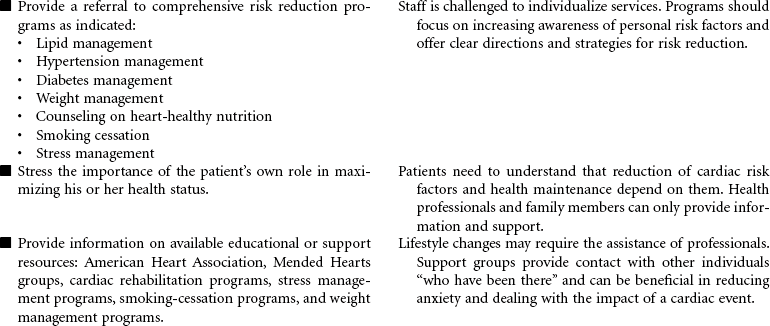
 Deficient Knowledge
Deficient Knowledge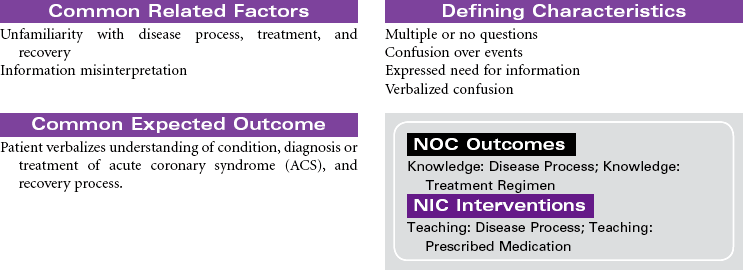



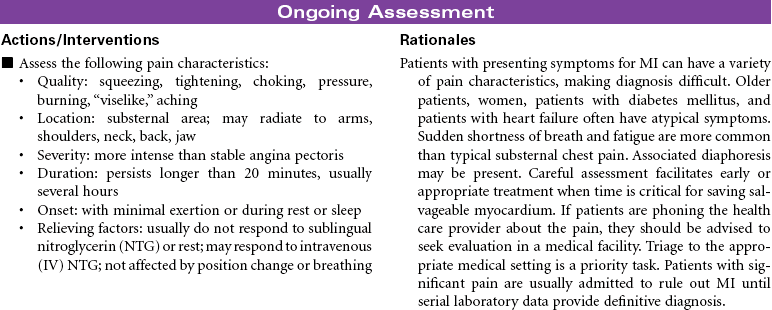
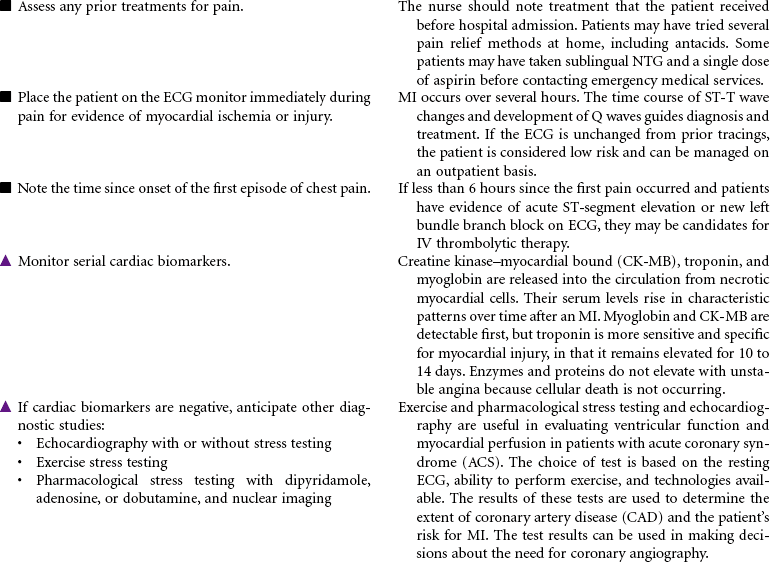
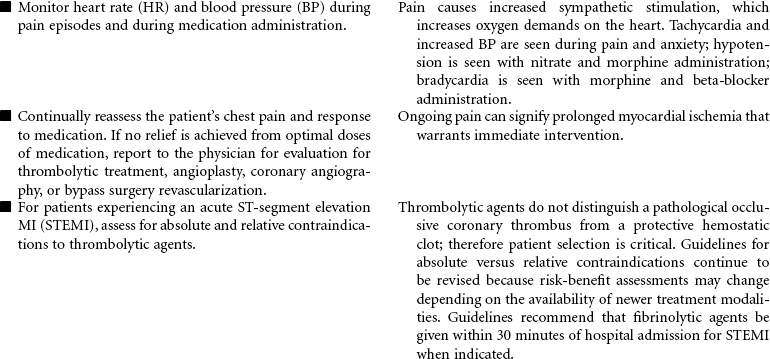
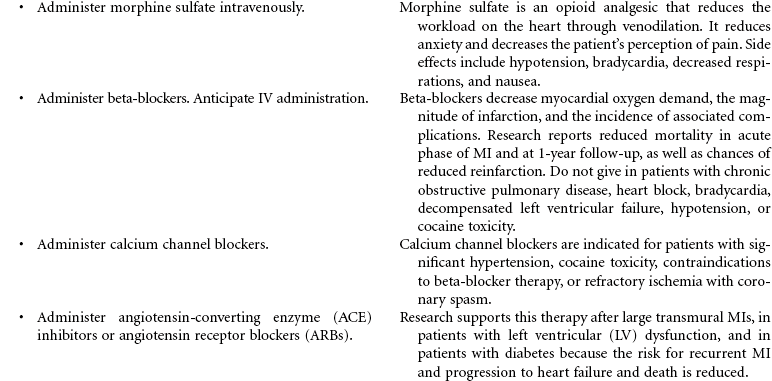
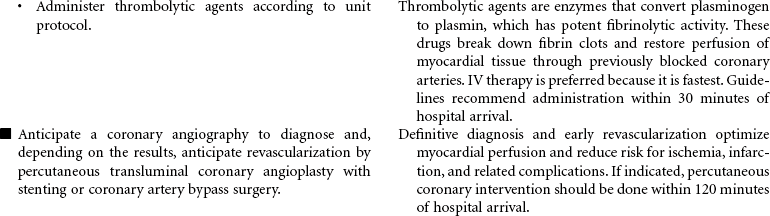
 Acute Pain
Acute Pain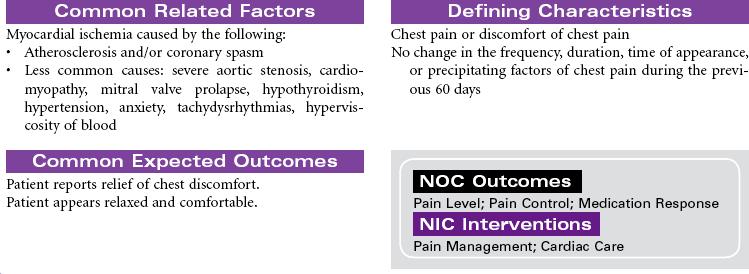
 Deficient Knowledge
Deficient Knowledge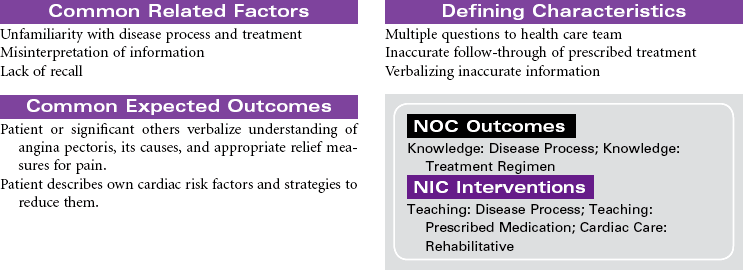

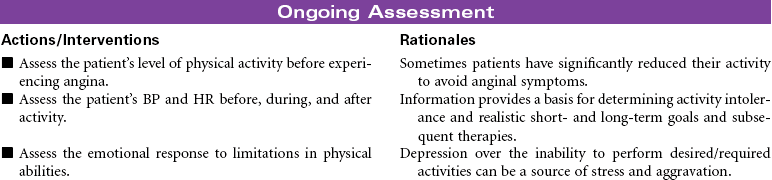
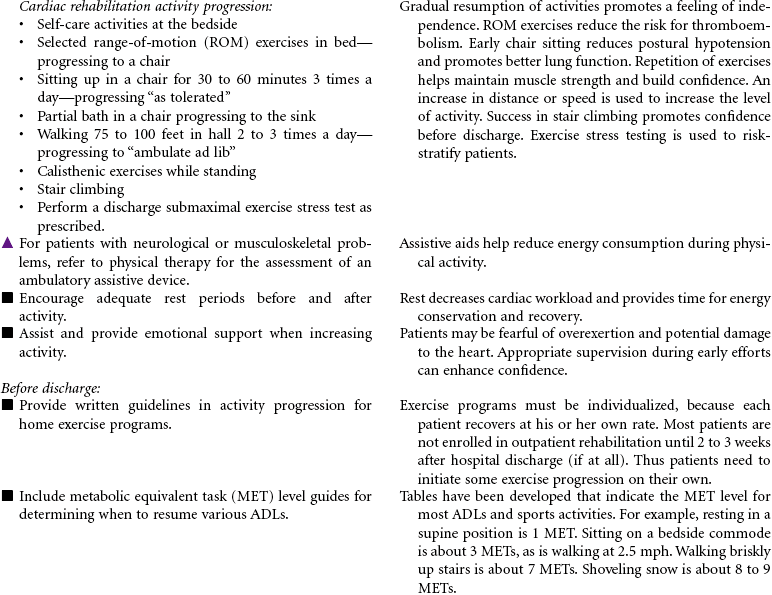
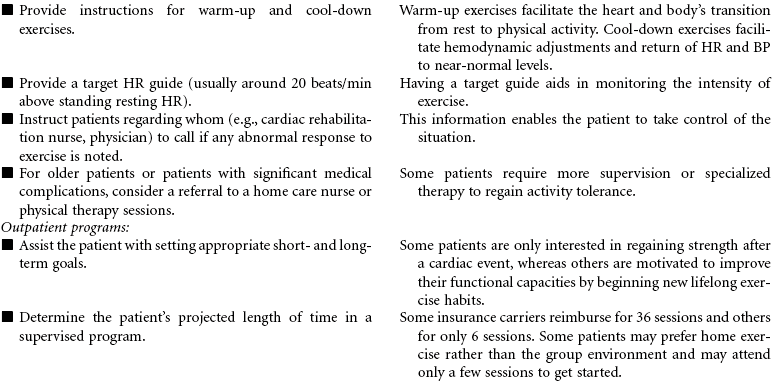
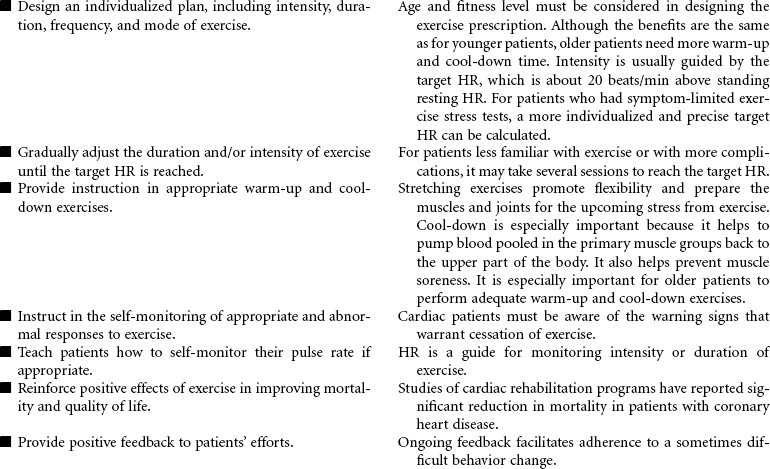
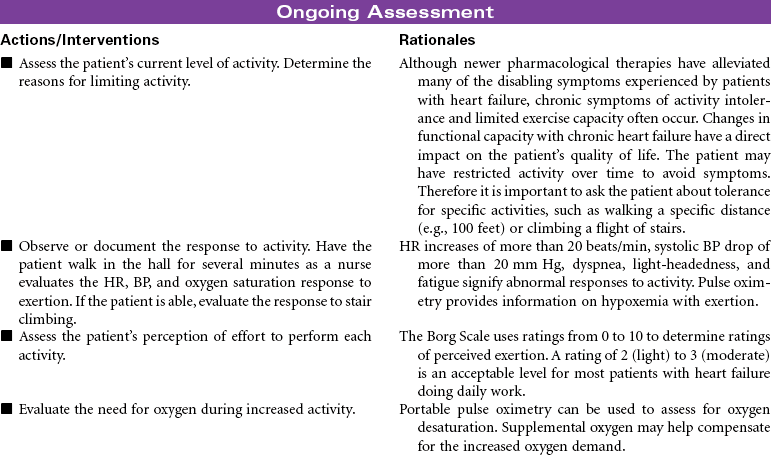
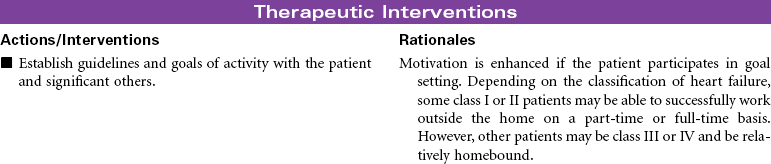
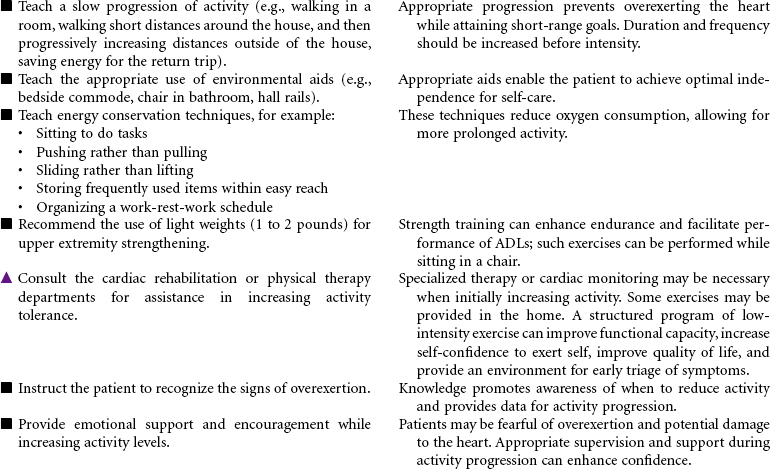
 Activity Intolerance
Activity Intolerance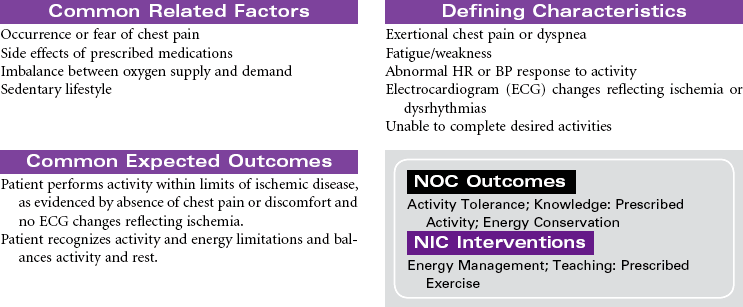

 Deficient Knowledge
Deficient Knowledge


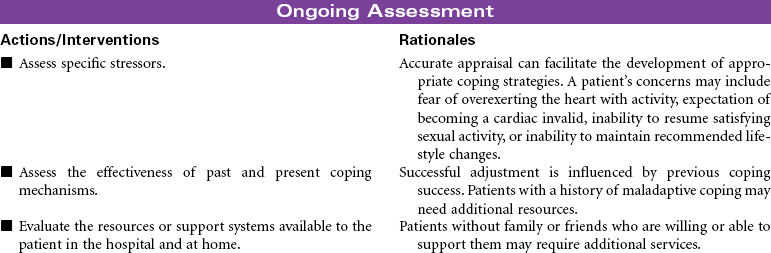
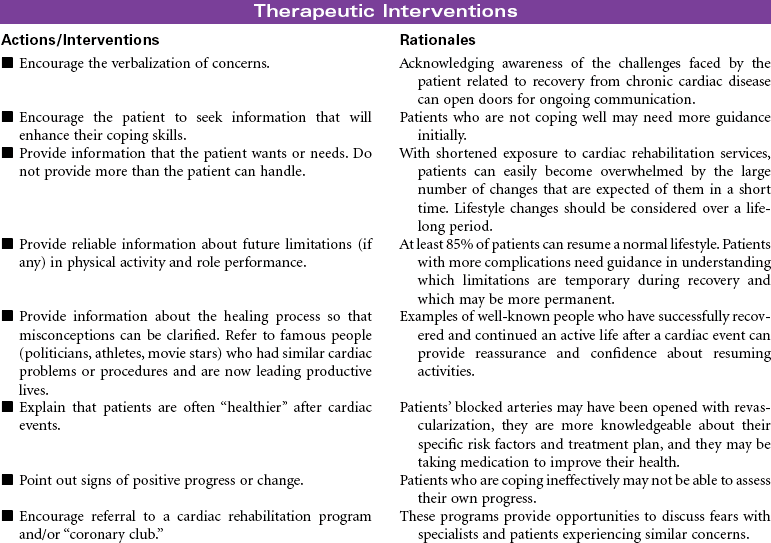
 Risk for Ineffective Coping
Risk for Ineffective Coping

 Activity Intolerance
Activity Intolerance
 Deficient Knowledge
Deficient Knowledge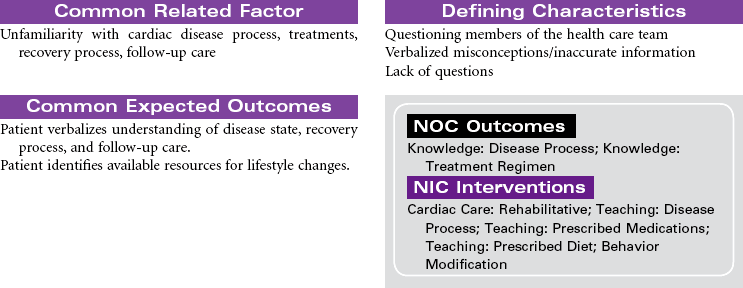
 Risk for Ineffective Coping
Risk for Ineffective Coping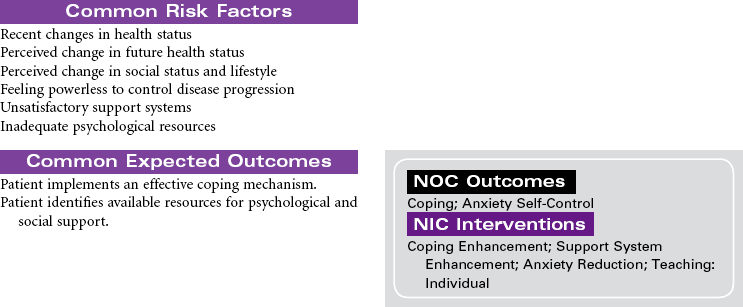
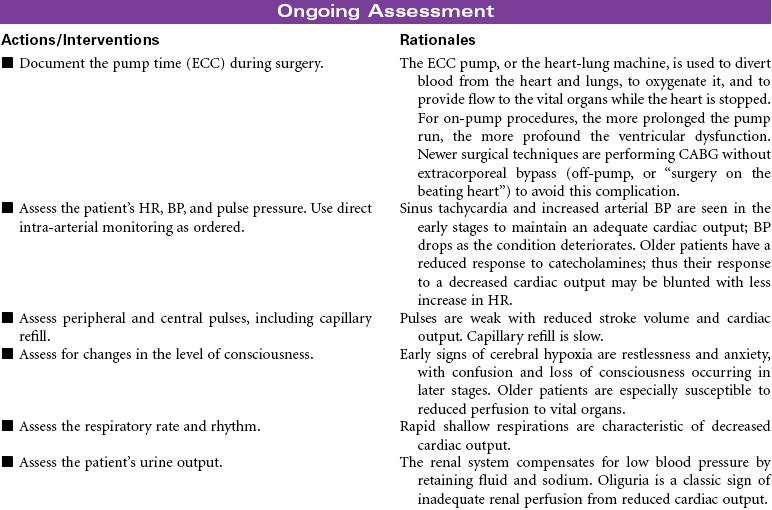
 Decreased Cardiac Output
Decreased Cardiac Output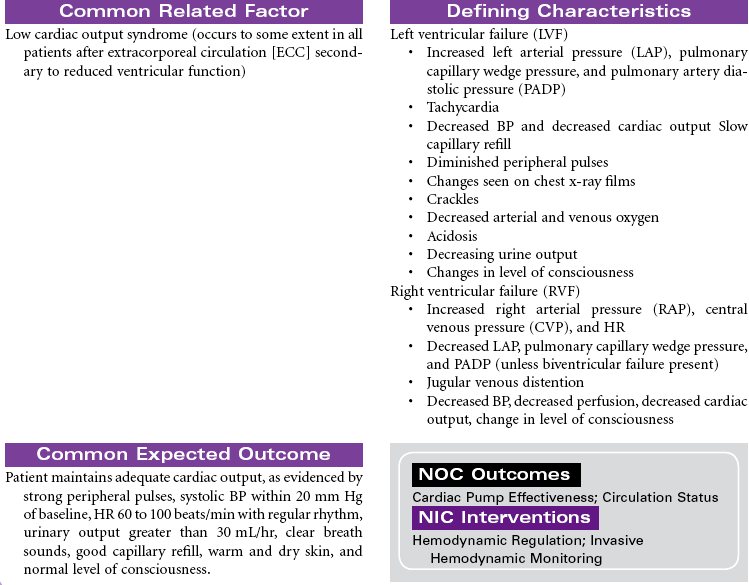
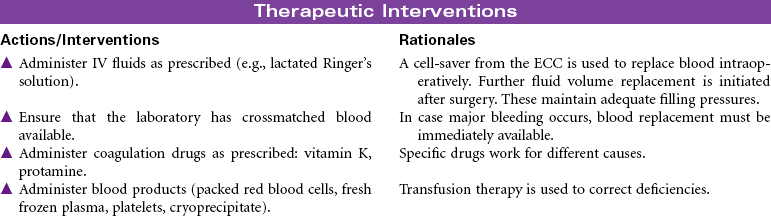
 Deficient Fluid Volume
Deficient Fluid Volume
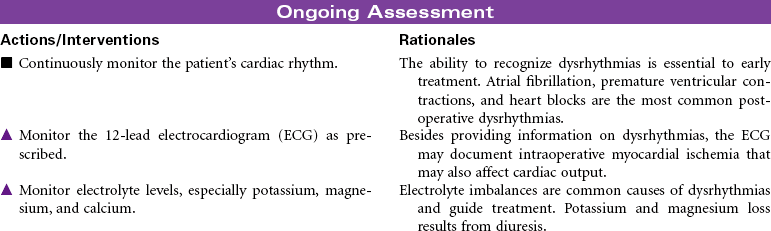
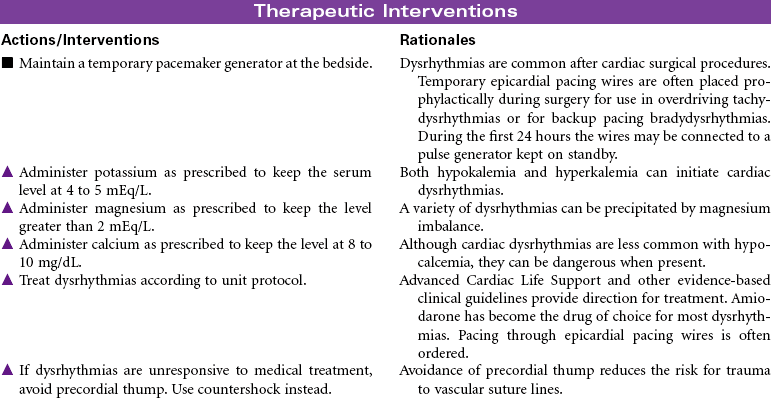
 Risk for Decreased Cardiac Output: Dysrhythmias
Risk for Decreased Cardiac Output: Dysrhythmias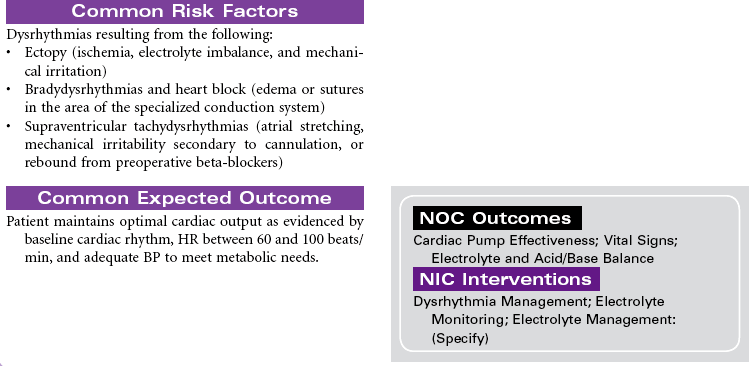
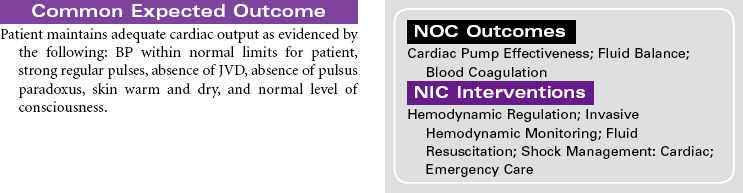
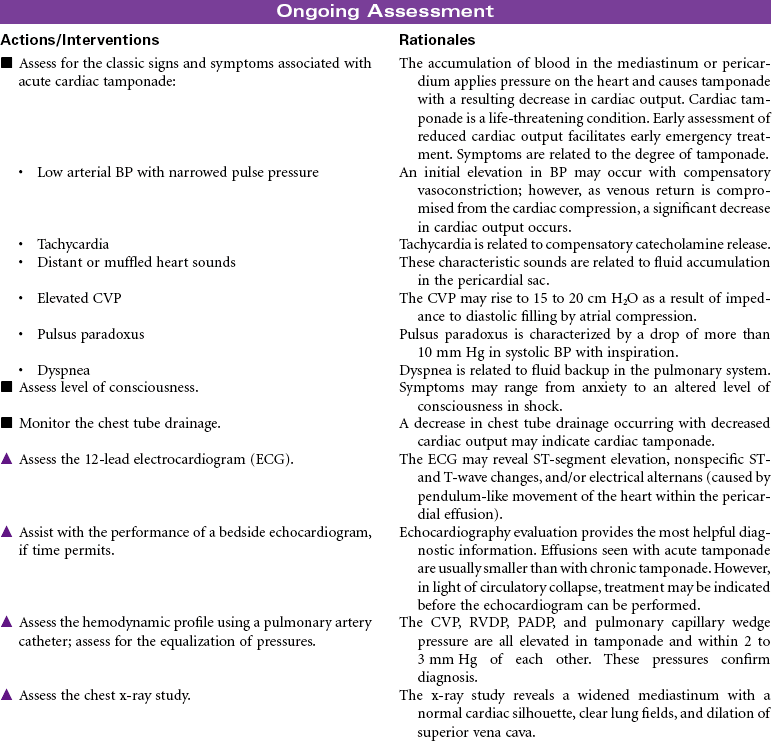
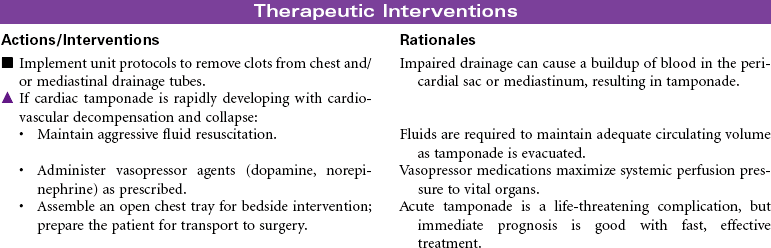
 Decreased Cardiac Output: Cardiac Tamponade
Decreased Cardiac Output: Cardiac Tamponade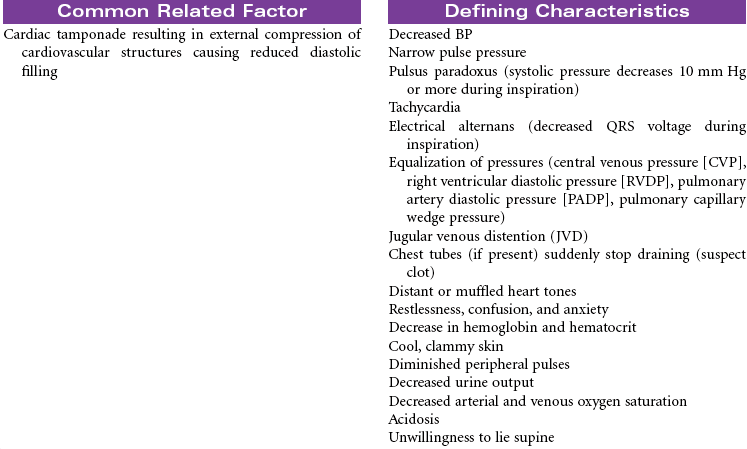
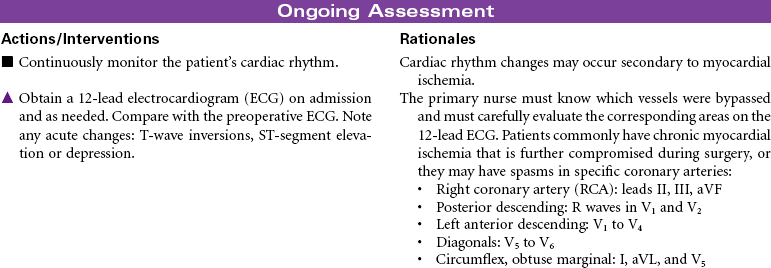
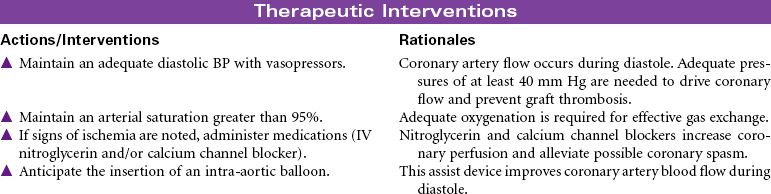
 Risk for Ineffective Myocardial Tissue Perfusion
Risk for Ineffective Myocardial Tissue Perfusion

 Risk for Electrolyte Imbalance
Risk for Electrolyte Imbalance


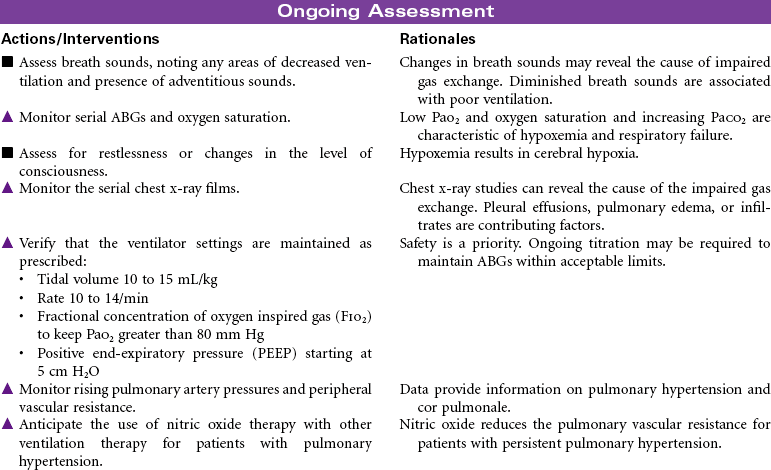
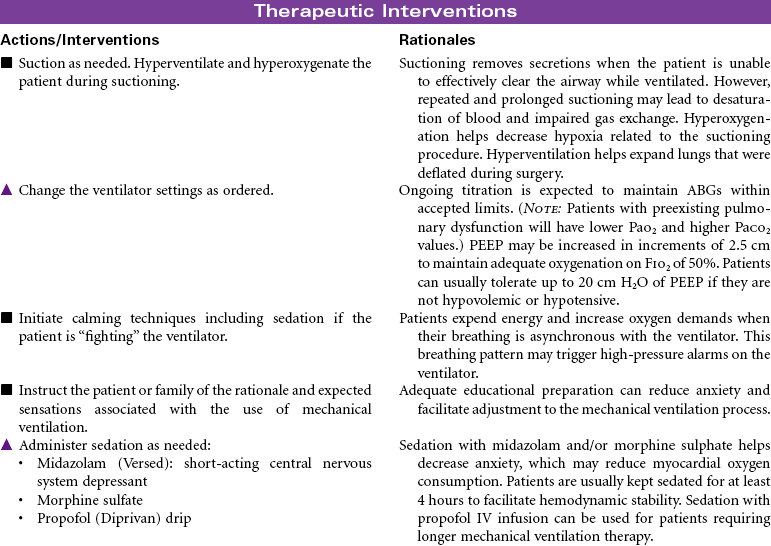
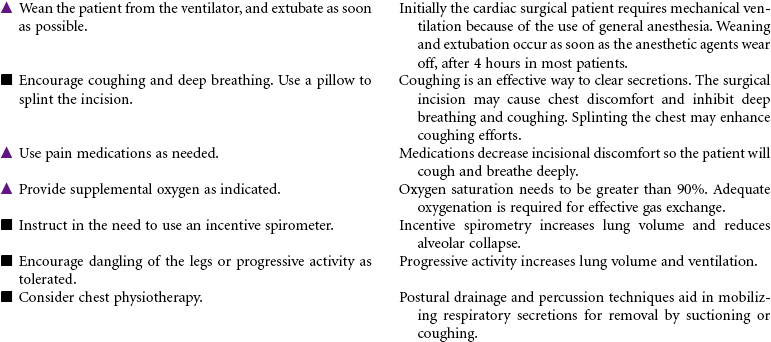
 Risk for Impaired Gas Exchange
Risk for Impaired Gas Exchange
 Fear
Fear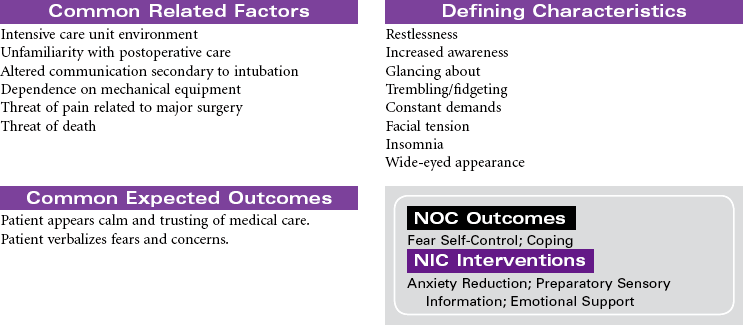


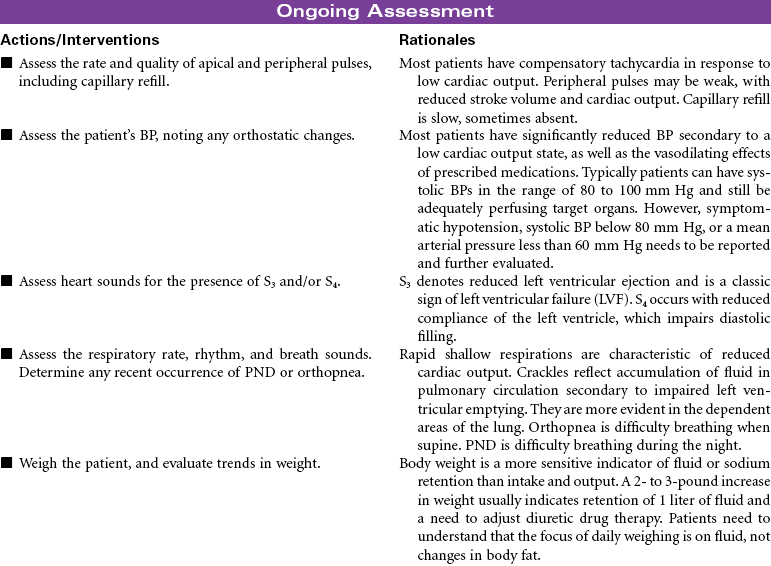
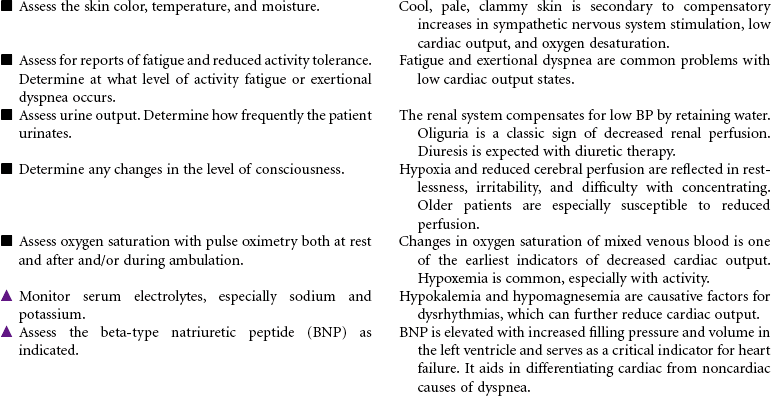
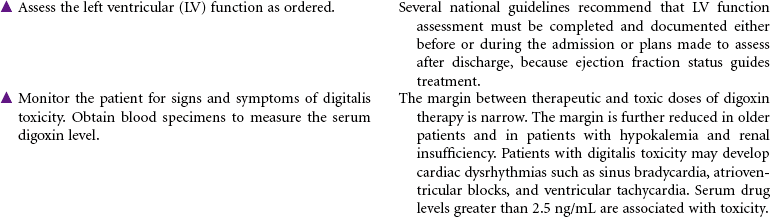
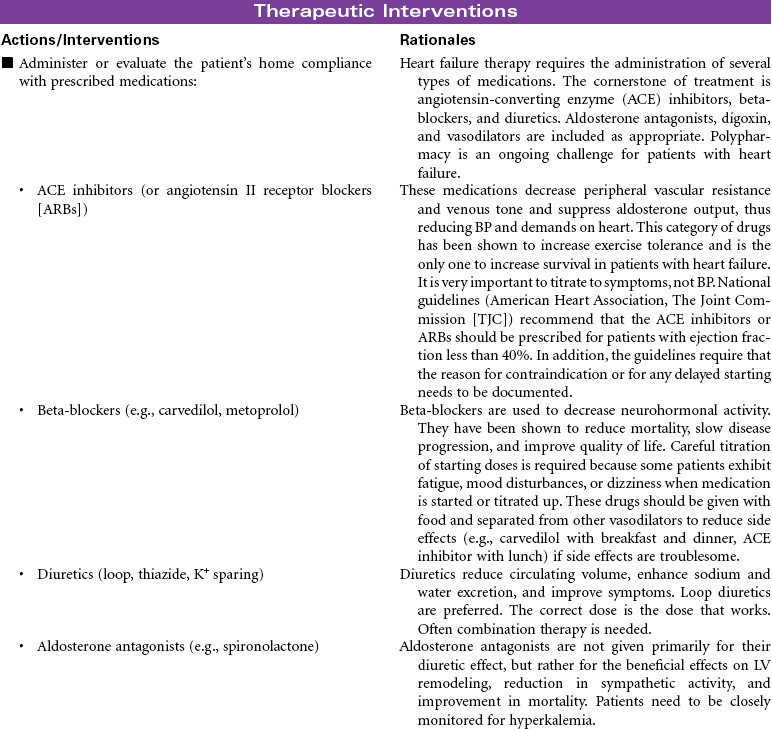
 Decreased Cardiac Output
Decreased Cardiac Output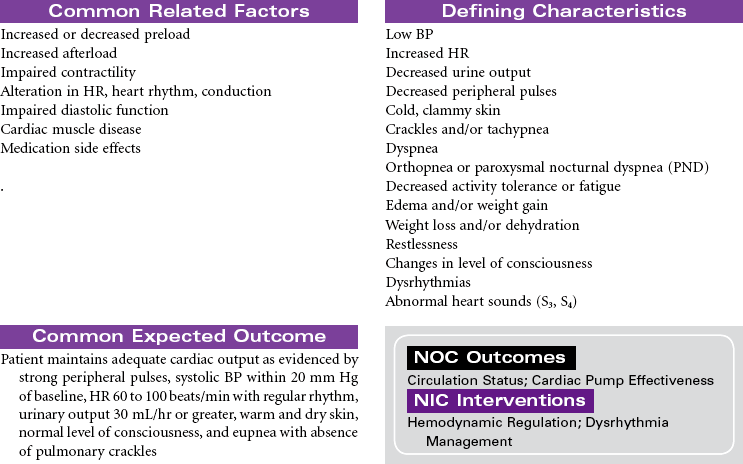
 Excess Fluid Volume
Excess Fluid Volume
 Activity Intolerance
Activity Intolerance
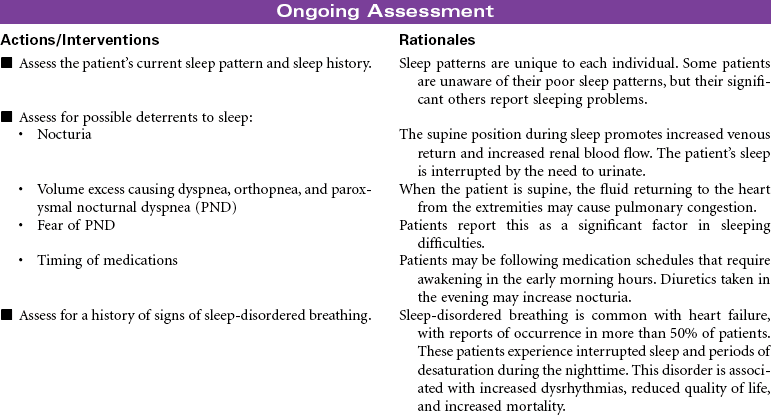
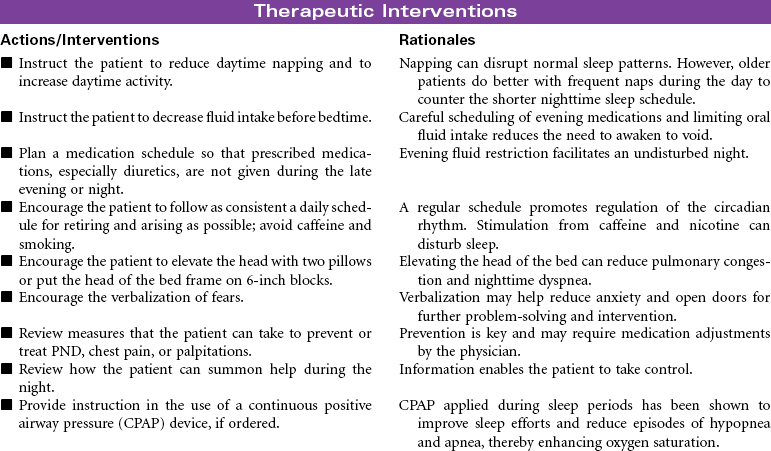
 Insomnia
Insomnia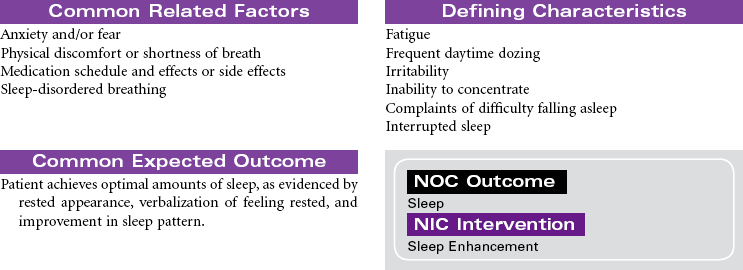
 Deficient Knowledge
Deficient Knowledge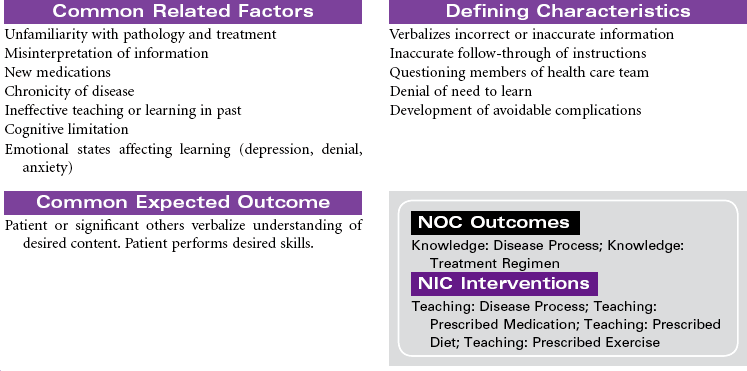




Get Clinical Tree app for offline access
