A Family Perspective in Community/Public Health Nursing
Claudia M. Smith*
Focus Questions
Why use a family perspective in community/public health nursing?
How do families differ? How are they the same?
What different family approaches have been proposed in the past?
How can these approaches be integrated?
How is the family perspective used in the practice of community/public health nursing?
Key Terms
Anxiety
Appraisal
Boundary
Coping
Developmental tasks
Double-bind communication
Dysfunctional
Family
Function
Hierarchy
Interactional style
Level of differentiation
Metacommunication
Needs
Process
Resilience
Resources
Roles
Stages
Strengths
Structure
Style
Subsystems
Transition
Triangle
Values
A family perspective
All nurses can and should practice family nursing. People are born into and grow, live, and die within their families. Everyone has a family. Families have different structures and sizes, have different levels of connection and ways of operating with each other, and may be geographically close or distant. Families can offer support and love and can also bring their members disappointment and grief. People grow older, may move away, or may sometimes try to pretend that they do not have a family; but ultimately, the person that one becomes is a reflection of the family from which one came.
Family as Client
The family as a unit of care has been a focus in community/public health nursing since its beginning (Whall, 1993). Nurses and other workers in the community recognized that the family was a major source of support and influence in many situations. The community/public health nurse learned to include the family in nursing care whether the issue was a family member with an illness, a change in the family (e.g., birth, death), or health promotion and disease prevention. People’s lifestyles and, consequently, their health are intimately tied to the culture, values, beliefs, practices, and socioeconomic status they share with their families.
Appreciation of the family as a unit of care evolved naturally as community/public health nurses worked within the community. With this work came a recognition that not all families are able to provide all their members with what they need to reach optimal levels of health. Community/public health nurses have a unique position because they are broadly educated and able to integrate different perspectives that contribute to an understanding of family functioning. Nurses also have a unique role within the community that offers them access to family situations. Focusing on the family is a helpful step to take in working toward a broader perspective of caring for the individual, the family, and the entire community.
Can a difference be found in using a family rather than an individual perspective? Consider the following example.
The opportunity to look at a bigger picture gives a perspective that is very different from the one presented by an individual view of Michelle. Viewing the situation solely as Michelle’s problem is difficult. The community/public health nurse may still choose to focus only on Michelle’s difficulties but realizes that these difficulties are connected to other issues and to the health of other people. Not only is Michelle’s health a concern, but the health of other family members and the entire family is also at risk. The family can either be supportive of Michelle or block attempted interventions. Community/public health nursing recognizes the importance of the family and defines the entire family as the unit of treatment. Michelle will be involved, but the whole family will become the focus for nursing care.
A problem can be viewed in many ways. In the past, science has often used a cause-and-effect way of thinking: Germ A causes sickness B. Applying medicine C cures the sickness. This example is a type of cause-and-effect thinking that became popular in the medical field after medications and inoculations proved to be successful in combating specific infectious illnesses.
Real life, however, is more complex than what simple cause-and-effect thinking implies. Not every person exposed to a certain pathogen becomes ill. Becoming infected depends on variables such as general level of health, stress level at the time, previous antibody development, and genetic susceptibility. Many different events occur at the same time. When the organism confronts these events while various factors are in balance, health is usually maintained. When imbalance exists, illness or dysfunction may occur—not because of any one event but because of a combination of factors. This recognition of the complexity and interconnectedness of a living organism is a systemic, rather than a cause-and-effect, way of thinking.
Individuals in a family can be thought of as a living system. Each person is one of the elements that are interrelated with one another. A boundary or imaginary wall exists around the family, similar to the thin membrane of a cell wall. This boundary can vary; it can be rigid and impenetrable, or it can be a permeable membrane that allows exchange in and out of the system. Each member, although only a part of the system, has the potential to change the patterns and organization of the entire system. Together, the individuals within the family make up something new that is different from and greater than the simple sum of its members.
Living systems have parts that undergo growth and change. At any given point in time, the individuals in the family will be undergoing change themselves. The members are growing, developing, learning, and changing, usually on trajectories or paths that are recognizable as part of the life cycle. Thus, the family as a living system is constantly changing.
The boundaries of the system permit some exchange of information between the inside and the outside. The family is one system; the community outside the family is another. Bronfenbrenner (1979), while studying children in families, proposed the idea of different levels of systems that constitute broader and broader environmental contexts in which the child will grow. A phenomenon can be viewed from genetic, biochemical, individual, family, community, and societal perspectives. These various levels of analysis can be used when thinking about family nursing care. Note that family is not the only perspective but is one piece in an ever-broader ecological context of conceptualizing the appropriate target of intervention.
Why Choose a Family Perspective?
• The family assumes a crucial role in maintaining health. Such a strong relationship exists between the family and health care that the role of the family becomes paramount in maintaining health. Health beliefs, values, and behaviors are learned and supported in the family. Health promotion activities are taught and implemented. Denham (2003) developed the Family Health Model after finding that the mother plays a key role in transmitting health beliefs about issues such as food choice and preparation, exercise, rest, and sleep patterns to children. The family is also a critical resource in the delivery of health care. How decisions are made about when to seek care, how health care is paid for, and how the recommended treatment regimens are carried out are all enacted within the family. The family is sometimes the primary care provider for its members who are ill and dependent. Changes in lifestyle are often required of the whole family if the level of wellness of one of the members is affected. Research evaluating the effectiveness of service delivery validates a family-centered approach. Families that form a partnership with care providers who recognize the parents as experts on their children’s needs have more positive outcomes for their children (Law et al., 2003). This approach is considered as the best practice for families with children with disabilities (King et al., 2002).
• The unique goals of family nursing—individual health, supportive interpersonal relationships, and an effective family unit—can be achieved only by using a family perspective. Hanson (2005) suggests that family is the umbrella under which all other nursing should be practiced. Family nursing is a movement in nursing that is coming into its own identity. By definition, all nursing practice is oriented toward achieving goals that are beneficial to the health and well-being of individuals within society. The goals that are put forth in family nursing—goals for individuals, relationships, and the family unit—can be addressed only by using a family perspective.
What is a family?
Definition of Family
Thus far, this text has talked about families as if all families are alike and as if everyone understands what is meant when the word family is used. In the United States, as in other parts of the world, many different kinds of families exist. Community/public health nurses need a definition broad enough to encompass the many ways they will be interacting with families. Box 12-1 presents various definitions that have been proposed by family theorists and experts. The definition of the term family must not ignore the atypical or nontraditional family forms that are often encountered in current communities. The definition should also provide some structure to the way nurses think about families to establish a framework for intervention. The definition adopted by this text is as follows: a family is an open and developing system of interacting personalities with a structure and process enacted in relationships among the individual members, regulated by resources and stressors, and existing within the larger community.
How Are Families Alike and Different?
All living systems need some sort of organization and pattern to function. Families also have this organization. Many people use a framework of structure, process, and function to describe the complex nature of families.
Structure
Structure refers to the elements of the family and the organization of these elements within the family. Over the life of a family, structure does not remain exactly the same, but a certain continuity of structure is maintained. Structure is defined in several ways. Some people define structure anthropologically, using family types defined in terms of lineage and power. For example, families may be matriarchal or patriarchal. Other people look at the arrangement of members within the system in terms of subsystems, coalitions, and other structures that have hierarchies and boundaries; this is explored in more depth in the structural–functional approach discussed later in this chapter. Still other persons believe that structure means the diversity of family forms.
Family Forms
Some type of family exists in all societies, although there is a wide diversity of forms. Variations may even exist among classes within the same society. In the past, in Greece and America, for example, slaves were prevented by law from forming legal families. Even so, the family in some form (although not necessarily the traditional nuclear family) is an ideal that most people try to attain.
Family structures have changed across societies and over time. Our idea of the traditional American family living in a household with extended family members such as grandparents is actually a myth that has been popularized through the years (Hareven, 1982). Current family types are varied and changing. Of all the households in the United States, only 67.1% were families, defined by the census as two or more persons related by birth or marriage and living together under one roof (U.S. Bureau of the Census, 2010). Nonfamily households, including single people living alone, nonrelatives living together, and cohabiting couples, now comprise 32.9% of the population (Figure 12-1). One-third of all households has members under 18 years of age. Among single parent households, 85% are headed by mothers. Two-thirds of children live with both parents, 23% live with mother only and 3% live with father only (Child Trends Data Bank, 2011).
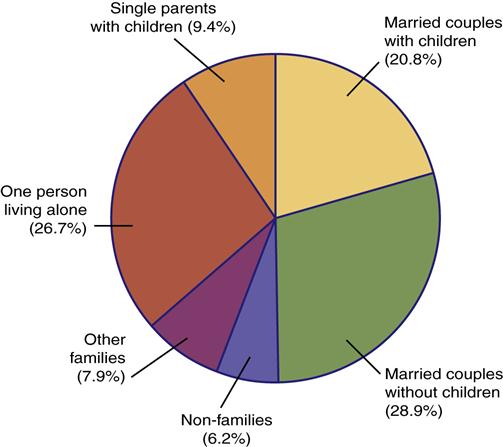
N = 117.5 million households. (Data from U.S. Bureau of the Census. [2010]. America’s families and living arrangements: 2010: Tables FG10 and H2. Retrieved September 10, 2011 from http://www.census.gov/population/www/socdemo/hh-fam/cps/ 2010.html.)
Households have changed since 2000. “Other” family households have almost doubled; these include householders with adult child(ren), householders with a parent, and grandparent householders with grandchild(ren) under 18 years of age (U.S. Bureau of the Census, 2010). The recent economic recession has contributed to more young adult children and adult children living with their parents. Over 40% of births in 2009 were to unmarried women, although half of these women were in cohabitating unions (Child Trends Data Bank, 2011). Box 12-2 presents some different family forms.
Process
A process is a phenomenon that occurs over time. Families, individuals, and society go through processes of growth, development, and change. The term implies change, but within every change, some pattern and connectedness with previous and future patterns is often found.
Family process can be defined as predictable and repetitive interaction patterns within families. For example, mom always watches Johnnie’s behavior very closely. Johnnie gets upset by this and complains to dad. Dad goes to mom and complains that she is too harsh with Johnnie. Mom backs off for a while but soon resumes her attention. Such interaction can be observed in dyads (two-person groups), or in interconnecting triangles (three-person groups) within the family.
Families also seem to have a characteristic way of interacting as a unit in relation to the outside world. This process can be open or closed, separate or connected. Families may allow information from the environment to help them problem-solve or close themselves off from outside influence. Families may act together in a cohesive manner, withdraw from each other, or even split apart. The behavior of the family may be random and chaotic or rigid and predictable.
Strengths
When one is discussing families or focusing on health needs, weaknesses or deficits of families frequently jump to the forefront. Focusing on family strengths not only helps us bring to light qualities that are sometimes forgotten but also reminds us of the incredible power and support families continue to offer. Family strengths are present in many areas of family functioning. All families, especially families at risk, have some strengths that are working or have worked in the past to maintain some level of health for their members.

Otto (1973) is one of the earliest authors to identify family strengths. The author’s framework for assessing family strengths is presented in Box 12-3. Curran (1983) also identifies family strengths such as teaching respect for others, displaying a sense of play and humor, teaching children a sense of right and wrong, having a shared religious core, sharing leisure time, respecting privacy, and developing shared rituals and traditions. Many researchers studying family stress and coping have started to focus on family strengths—as well as strains and stressors—that affect families (Bomar, 2004; Feeley & Gottlieb, 2000). Some of the tools and assessment strategies for these ideas are presented in Chapter 13.
Function
In the past, some who wrote about the family used the term functioning to describe the activities the family provided for the well-being of its members. In this text, the term family function is used to describe results or the effectiveness of families. Does the family operate in a way that successfully provides for the needs of its members? Successful functioning is a measure of normality or health. Examining how well individual family members care for self and others is a way of assessing that family’s level of health. Unhealthy families are called dysfunctional.
Family functioning is best viewed as a continuum. When the words functional and dysfunctional are used, family functioning can be considered good or bad. There is no such thing as a good family or a bad family. All families fall somewhere along a continuum from minimal functioning to optimal functioning in which all members benefit. Many different means can be used to assess families, according to different views of optimal family functioning. Bowen (1978) describes families as more or less healthy according to (1) their ability to separate thinking from feeling and (2) the amount of anxiety that is present in the family. Tapia (1997) defines levels of family functioning from chaotic to adult, according to the family’s degree of emotional maturity. Olson and McCubbin (1982) suggest that families should have moderate degrees of cohesion, coordination, and adaptability for healthy family functioning.
For optimal family functioning, the structure and process must combine in a way that allows the family to be effective. Understanding the particular stresses and history that have shaped a specific family’s current way of operating helps the nurse understand that family. Conversely, the typical level of functioning of a family may determine its developing processes and structure (e.g., divorce, single parenthood, the arrangement of subsystems). Structure, process, and function are interrelated, and all of these aspects must be considered when assessing a family. However, no one structure, process, or type of function is proposed here as the right one. Many variations exist within these dimensions that can lead to healthy families. See Chapter 10 for a further discussion of diversity and cultural differences.
Historical frameworks
The study of family does not fit neatly into any one field, be it genetics, physiology, anthropology, sociology, or psychology; many disciplines have contributed to the understanding of family functioning. The study of family is interdisciplinary, and theories of family have been broadly adapted and used. However, most frameworks used to study family have been drawn from family sociology or family therapy.
Sociologists have studied families since the nineteenth and early twentieth centuries because of the need to solve emerging social problems. The 1950s saw the development of conceptual frameworks in family theory. Around that time, interest in the family as a unit of treatment emerged in the field of psychiatry. Family therapists began focusing on pathological factors within families. Relatively recent trends have included the formulation of family theories attempting to describe the characteristics of healthy families, the development of theories of family coping with stressful situations, and the emergence of frameworks for family nursing.
Family approaches can be separated into several areas that provide different viewpoints that describe the complexity of the family. Families develop, interact, communicate, have structures, cope with stress, develop identity, and operate as systems. The following sections describe these approaches in more detail.
Family Development
The family development approach attempts to track change over time in a family. Families and individuals are engaged in a developmental process of growth, aging, and change over the life span. In this approach, a longitudinal view of the family classifies and predicts differences in families as they develop. The assumption is that both individuals in the family and the family as a whole need to accomplish certain tasks at specific times in their life cycles. As the family confronts various stages of the life cycle, developmental tasks must be achieved if the stage is to be negotiated successfully. These tasks carry certain role expectations. If the tasks are not achieved at specific times as a result of stress, crises, lack of resources, or unhealthy family structure and process, they may never be completely achieved. The better equipped a family is to help each member complete his or her developmental tasks and help the family meet its group tasks, the more successful the development of the family will be. The theory assumes that commonalities exist for all families.
Duvall (1977) adapted this approach from the theory of individual developmental tasks proposed by Havighurst. Duvall defined nine ever-changing family developmental tasks that span the family life cycle and outlined eight stages of the family life cycle and specific tasks for each stage (Table 12-1). Family stages are defined by the age of the oldest child. For example, a family that has two children aged 7 and 2 years would be considered “a school-aged family” rather than “a preschool family.”
Table 12-1
| Stage | Tasks | |
| Establishing | Marital couple | |
| Early childbearing | Adding an infant | |
| Preschool | Children (3–5 years old) | < div class='tao-gold-member'> Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|