Exercise and activity
Objectives
• Define the key terms and key abbreviations listed in this chapter.
• Explain how to prevent the complications from bedrest.
• Describe the devices used to support and maintain body alignment.
• Explain the purpose of a trapeze.
• Describe range-of-motion exercises.
• Perform the procedures described in this chapter.
Key terms
abduction Moving a body part away from the midline of the body
adduction Moving a body part toward the midline of the body
ambulation The act of walking
atrophy The decrease in size or the wasting away of tissue
contracture The lack of joint mobility caused by abnormal shortening of a muscle
deconditioning The loss of muscle strength from inactivity
dorsiflexion Bending the toes and foot up at the ankle
extension Straightening a body part
external rotation Turning the joint outward
flexion Bending a body part
footdrop The foot falls down at the ankle; permanent plantar flexion
hyperextension Excessive straightening of a body part
internal rotation Turning the joint inward
orthostatic hypotension Abnormally low (hypo) blood pressure when the person suddenly stands up (ortho and static); postural hypotension
plantar flexion The foot (plantar) is bent (flexion); bending the foot down at the ankle
postural hypotension See “orthostatic hypotension”
pronation Turning the joint downward
range of motion (ROM) The movement of a joint to the extent possible without causing pain
rotation Turning the joint
supination Turning the joint upward
syncope A brief loss of consciousness; fainting
KEY ABBREVIATIONS
| ADL | Activities of daily living |
| CMS | Centers for Medicare & Medicaid Services |
| ID | Identification |
| OBRA | Omnibus Budget Reconciliation Act of 1987 |
| PT | Physical therapist |
| ROM | Range of motion |
Being active is important for physical and mental well-being. Most people move about and function without help. Illness, surgery, injury, pain, and aging cause weakness and some activity limits. Some people are in bed for a long time. Some are paralyzed. Some disorders worsen over time. They cause decreases in activity. Examples include arthritis and nervous system and muscular disorders (Chapter 39). Inactivity, whether mild or severe, affects every body system. It also affects mental well-being.
Deconditioning is the loss of muscle strength from inactivity. When not active, older persons become deconditioned quickly. Nurses use the nursing process to promote exercise and activity in all persons to the extent possible. The care plan and your assignment sheet include the person’s activity level and needed exercises.
See Residents With Dementia: Exercise and Activity.
Bedrest
The doctor orders bedrest to treat a health problem. It may be a nursing measure if the person’s condition changes. Generally bedrest is ordered to:
These types of bedrest are common:
• Strict bedrest. Everything is done for the person. No activities of daily living (ADL) are allowed.
• Bedrest with commode privileges. The person uses the commode for elimination.
• Bedrest with bathroom privileges (bedrest with BRP). The person uses the bathroom for elimination.
The person’s care plan and your assignment sheet tell you the activities allowed. Always ask the nurse what bedrest means for each person. Check with the nurse if you have questions about a person’s activity limits.
Complications from bedrest
Bedrest and lack of exercise and activity can cause serious complications. Every system is affected. Pressure ulcers, constipation, and fecal impaction can result. Urinary tract infections and renal calculi (kidney stones) can occur. So can blood clots (thrombi) and pneumonia (inflammation and infection of the lung).
The musculo-skeletal system is affected by lack of exercise and activity. These complications must be prevented to maintain normal movement:
• A contracture is the lack of joint mobility caused by abnormal shortening of a muscle. The contracted muscle is fixed into position, is deformed, and cannot stretch (Fig. 26-1, p. 416). Common sites are the fingers, wrists, elbows, toes, ankles, knees, and hips. They can also occur in the neck and spine. The person is permanently deformed and disabled.
• Atrophy is the decrease in size or the wasting away of tissue. Tissues shrink in size. Muscle atrophy is a decrease in size or a wasting away of muscle (Fig. 26-2, p. 416).


Orthostatic hypotension and blood clots (Chapter 35) occur in the circulatory system. Orthostatic hypotension is abnormally low (hypo) blood pressure when the person suddenly stands up (ortho and static). When a person moves from lying or sitting to a standing position, the blood pressure drops. The person is dizzy and weak and has spots before the eyes. Syncope can occur. Syncope (fainting) is a brief loss of consciousness. (Syncope comes from the Greek word synkoptein. It means to cut short.) Orthostatic hypotension also is called postural hypotension. (Postural relates to posture or standing.) Box 26-1 lists the measures that prevent orthostatic hypotension. Slowly changing positions is key.
Good nursing care prevents complications from bedrest. Good alignment, range-of-motion exercises (p. 419), and frequent position changes are important measures. These are part of the care plan.
See Focus on Communication: Complications of Bedrest.
Positioning
Body alignment and positioning were discussed in Chapter 16. Supportive devices are often used to support and maintain the person in a certain position:
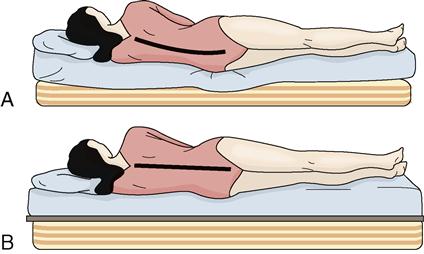
• Bed-boards—are placed under the mattress. They prevent the mattress from sagging (Fig. 26-3). Usually made of plywood, they are covered with canvas or other material. There are two sections so the head of the bed can be raised. One section is for the head of the bed. The other is for the foot of the bed.
• Foot-boards—are placed at the foot of mattresses (Fig. 26-4). They prevent plantar flexion that can lead to footdrop. In plantar flexion, the foot (plantar) is bent (flexion). Footdrop is when the foot falls down at the ankle (permanent plantar flexion). The foot-board is placed so the soles of the feet are flush against it. The feet are in good alignment as when standing. Foot-boards also serve as bed cradles. They prevent pressure ulcers by keeping top linens off the feet and toes.
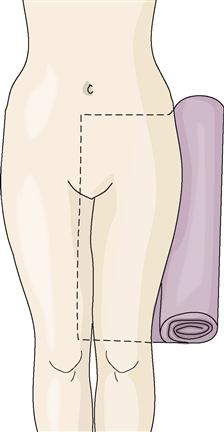
• Trochanter rolls—prevent the hips and legs from turning outward (external rotation) (Fig. 26-5). A bath blanket is folded to the desired length and rolled up. The loose end is placed under the person from the hip to the knee. Then the roll is tucked alongside the body. Pillows or sandbags also keep the hips and knees in alignment.
• Hip abduction wedges—keep the hips abducted (apart) (Fig. 26-6). The wedge is placed between the person’s legs. These are common after hip replacement surgery.
• Hand rolls or hand grips—prevent contractures of the thumb, fingers, and wrist (Fig. 26-7, p. 418). Foam rubber sponges, rubber balls, and finger cushions (Fig. 26-8, p. 418) also are used.
• Splints—keep the elbows, wrists, thumbs, fingers, ankles, and knees in normal position. They are usually secured in place with Velcro (Fig. 26-9, p. 418).
• Bed cradles—keep the weight of top linens off the feet and toes (Fig. 26-10, p. 418). The weight of top linens can cause footdrop and pressure ulcers.





Exercise
Exercise helps prevent contractures, muscle atrophy, and other complications from bedrest. Some exercise occurs with ADL and when turning and moving in bed without help. Other exercises are needed for muscles and joints. (See “Range-of-Motion Exercises” and “Ambulation,” p. 424.)
A trapeze is used for exercises to strengthen arm muscles. The trapeze hangs from an overbed frame (Fig. 26-11). The person grasps the bar with both hands to lift the trunk off the bed. The trapeze is also used to move up and turn in bed.

See Focus on Rehabilitation: Exercise.
 Range-of-motion exercises
Range-of-motion exercises
The movement of a joint to the extent possible without causing pain is the range of motion (ROM) of that joint. Range-of-motion exercises involve moving the joints through their complete range of motion (Box 26-2). They are usually done at least 2 times a day.
• Active range-of-motion exercises—are done by the person himself or herself.
• Passive range-of-motion exercises—you move the joints through their range of motion.
• Active-assistive range-of-motion exercises—the person does the exercises with some help.
 PERFORMING RANGE-OF-MOTION EXERCISES
PERFORMING RANGE-OF-MOTION EXERCISES



Quality of life
Remember to:
Pre-procedure
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


