The resident’s unit
Objectives
• Define the key terms and key abbreviations listed in this chapter.
• Identify the room temperatures required by OBRA and the CMS.
• Describe how to protect the person from drafts.
• List ways to prevent or reduce odors and noise.
• Explain how lighting affects comfort.
• Describe the basic bed positions.
• Identify the persons at risk for entrapment in the hospital bed system.
• Identify hospital bed system entrapment zones.
• Explain how to use the furniture and equipment in the person’s unit.
• Describe how a bathroom is equipped for the person’s use.
• Describe how to provide for safety, privacy, and comfort in the person’s unit.
• Explain how to maintain the person’s unit.
• Describe OBRA and CMS requirements for resident rooms.
Key terms
Fowler’s position A semi-sitting position; the head of the bed is raised between 45 and 60 degrees
full visual privacy Having the means to be completely free from public view while in bed
high-Fowler’s position A semi-sitting position, the head of the bed is raised 60 to 90 degrees
resident unit The personal space, furniture, and equipment provided for the person by the nursing center
reverse Trendelenburg’s position The head of the bed is raised and the foot of the bed is lowered
semi-Fowler’s position The head of the bed is raised 30 degrees; or the head of the bed is raised 30 degrees and the knee portion is raised 15 degrees
Trendelenburg’s position The head of the bed is lowered and the foot of the bed is raised
KEY ABBREVIATIONS
| CMS | Centers for Medicare & Medicaid Services |
| F | Fahrenheit |
| FDA | Food and Drug Administration |
| OBRA | Omnibus Budget Reconciliation Act of 1987 |
Nursing centers are designed to provide comfort, safety, and privacy. The intent is to have resident units as personal and home-like as possible. A resident unit is the personal space, furniture, and equipment provided for the person by the nursing center (Fig. 18-1).

Some residents have private rooms. Others share a room with another person. This area is private. It is treated like the person’s home.
Residents bring some furniture and personal items from home. As space allows, the person chooses where to place personal items. This promotes dignity and self-esteem. However, a resident cannot take or use another person’s space. Doing so violates the other person’s rights.
Comfort
Age, illness, and activity affect comfort. So do temperature, ventilation, noise, odors, and lighting. These factors are controlled to meet the person’s needs.
Temperature and ventilation
Heating and air conditioning systems maintain a comfortable temperature. Most healthy people are comfortable when the temperature is 68° F (Fahrenheit) to 74° F. This range may be too hot or too cold for others. Older persons and those who are ill may need higher temperatures for comfort.  Nursing centers maintain a temperature range of 71° F to 81° F. This is a requirement of the Omnibus Budget Reconciliation Act of 1987 (OBRA) and the Centers for Medicare & Medicaid Services (CMS).
Nursing centers maintain a temperature range of 71° F to 81° F. This is a requirement of the Omnibus Budget Reconciliation Act of 1987 (OBRA) and the Centers for Medicare & Medicaid Services (CMS).
Persons who are less active usually do not like cool areas. Nor do those who need help moving about. They must be dressed warmly. They also need warm room temperatures. You may find the rooms rather warm.
Stale room air and lingering odors affect comfort and rest. Ventilation systems provide fresh air and move room air. Drafts occur as air moves. Older persons and those who are ill are sensitive to drafts. To protect them from drafts:
Odors
Many odors occur in nursing centers. Food aromas and flower scents are pleasant. Bowel movements and urine have embarrassing odors. So do draining wounds and vomitus. Body, breath, and smoking odors may offend others.
Some people are very sensitive to odors. They may become nauseated. Good nursing care, ventilation, and housekeeping practices help prevent odors. To reduce odors:
• Empty, clean, and disinfect bedpans, urinals, commodes, and kidney basins promptly.
• Check to make sure toilets are flushed.
• Check incontinent persons often (Chapters 22 and 23).
• Clean persons who are wet or soiled from urine, feces, vomitus, or wound drainage.
• Change wet or soiled linens and clothing promptly.
• Keep laundry containers closed.
• Follow center policy for wet or soiled linens and clothing.
• Dispose of incontinence and ostomy products promptly (Chapters 22 and 23).
• Provide good hygiene to prevent body and breath odors (Chapter 20).
Smoke odors present special problems. Residents, visitors, and staff smoke only in the areas allowed. If you smoke, follow the center’s policy. Practice hand washing after handling smoking materials and before giving care. Give careful attention to your uniforms, hair, and breath because of smoke odors.
The center is the person’s home. Keep it free of unpleasant odors.
Noise
 The CMS requires comfortable sound levels. A “comfortable” sound level:
The CMS requires comfortable sound levels. A “comfortable” sound level:
Many older and ill persons are sensitive to noises and sounds. Common health care sounds may disturb them. Examples include:
• The clatter of dishes and meal trays
• Loud voices, TVs, radios, and so on
• Intercom systems and signal lights
• Wheels on stretchers, wheelchairs, carts, and other items needing oil
Loud talking and laughter in hallways and at the nurses’ station are common. Residents may think that the staff are talking and laughing about them.
People want to know the cause and meaning of new sounds. This relates to safety and security needs. Residents may find sounds dangerous, frightening, or irritating. They may become upset, anxious, and uncomfortable. What is noise to one person may not be noise to another. For example, a teenager enjoys loud music. It may bother adults.
Nursing centers are designed to reduce noise. Window coverings, carpets, and acoustical tiles absorb noise. Plastic items make less noise than metal equipment (bedpans, urinals, wash basins). To decrease noise:
See Residents With Dementia: Noise.
See Focus on Communication: Noise.
Lighting
 The CMS requires comfortable lighting. Such lighting:
The CMS requires comfortable lighting. Such lighting:
• Allows the resident to control the intensity, location, and direction of light
• Allows persons who are visually impaired to maintain or increase independent functioning
Good lighting is needed for safety and comfort. Glares, shadows, and dull lighting can cause falls, headaches, and eyestrain. A bright room is cheerful. Dim light is better for relaxing and rest.
Adjust lighting to meet the person’s changing needs. Window coverings are adjusted as needed. The overbed light can provide soft, medium, or bright lighting. Some centers have ceiling lights. They provide soft to very bright light.
Persons with poor vision need bright light. This is very important at mealtime and when moving about in the room and center. Bright lighting also helps the staff perform procedures.
Always keep light controls within the person’s reach. This protects the right to personal choice.
See Residents With Dementia: Lighting.
Room furniture and equipment
Rooms are furnished and equipped to meet basic needs. The room has furniture and equipment for comfort, sleep, elimination, nutrition, hygiene, and activity. There is equipment to communicate with staff, family, and friends. The right to privacy is considered.
The bed
Beds have electrical or manual controls. Beds are raised horizontally to give care. This reduces bending and reaching. The lowest horizontal position lets the person get out of bed with ease (Fig. 18-2). The head of the bed is flat or raised varying degrees.

Electric beds are common. Controls are on a side panel, bed rail, or the foot-board (Fig. 18-3, A). Some controls are hand-held devices (Fig. 18-3, B). Alert and oriented residents are taught to use the controls safely. They are warned not to raise the bed to the high position or to adjust the bed to harmful positions. They are told of any position limits or restrictions.

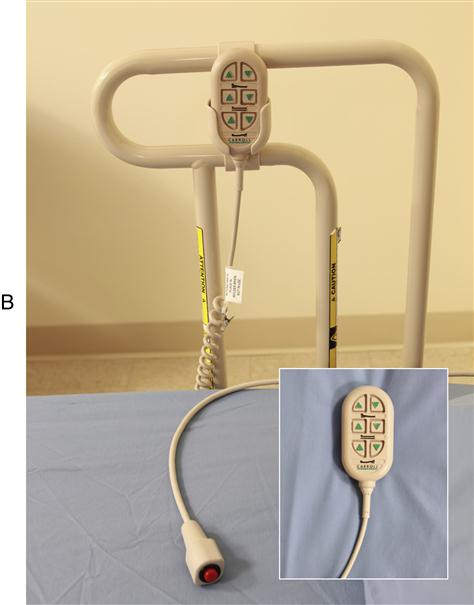
Most electric beds “lock” into any position by the staff. The person cannot adjust the bed to unsafe positions. Persons restricted to certain positions may need their beds locked. So may persons with confusion or dementia.
Manual beds have cranks at the foot of the bed (Fig. 18-4):
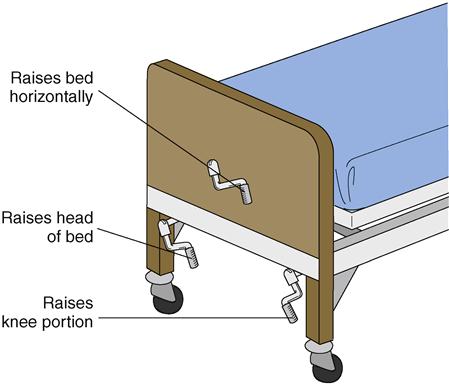
The cranks are pulled up for use. They are kept down at all other times. Cranks in the “up” position are safety hazards. Anyone walking past may bump into them.
See Promoting Safety and Comfort: The Bed.
PROMOTING SAFETY AND COMFORT
The Bed
Safety
Beds have bed rails and wheels. Bed wheels (Chapter 12) are locked at all times except when moving the bed. They must be locked when you:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


