Restraint alternatives and safe restraint use
Objectives
• Define the key terms and key abbreviations listed in this chapter.
• Describe the purpose of restraints.
• Identify the complications from restraint use.
• Identify restraint alternatives.
• Explain the legal aspects of restraint use.
• Explain how to use restraints safely.
• Perform the procedure described in this chapter.
Key terms
chemical restraint Any drug that is used for discipline or convenience and not required to treat medical symptoms
freedom of movement Any change in place or position of the body or any part of the body that the person is physically able to control
medical symptom An indication or characteristic of a physical or psychological condition
KEY ABBREVIATIONS
| CMS | Centers for Medicare & Medicaid Services |
| FDA | Food and Drug Administration |
| OBRA | Omnibus Budget Reconciliation Act of 1987 |
| TJC | The Joint Commission |
Chapters 12 and 13 have many safety measures. However, some persons need extra protection. They may present dangers to themselves or others (including staff). For example:
• Mrs. Perez forgets to call for help when getting up and with walking. Falling is a risk.
• Mrs. Wilson tries to pull out her feeding tube. The tube is part of her treatment.
• Ms. Walsh scratches and picks at a wound. This can damage her skin or the wound.
• Mr. Winters tries to hit, pinch, and bite the staff. They are at risk for harm.
 The Centers for Medicare & Medicaid Services (CMS) have rules for using restraints. Like the Omnibus Budget Reconciliation Act of 1987 (OBRA), CMS rules protect the person’s rights and safety. This includes the right to be free from restraint or seclusion. Restraints may only be used to treat a medical symptom or for the immediate physical safety of the person or others. Restraints may only be used when less restrictive measures fail to protect the person or others. They must be discontinued at the earliest possible time.
The Centers for Medicare & Medicaid Services (CMS) have rules for using restraints. Like the Omnibus Budget Reconciliation Act of 1987 (OBRA), CMS rules protect the person’s rights and safety. This includes the right to be free from restraint or seclusion. Restraints may only be used to treat a medical symptom or for the immediate physical safety of the person or others. Restraints may only be used when less restrictive measures fail to protect the person or others. They must be discontinued at the earliest possible time.
To meet the person’s safety needs, a resident care conference is held. The health team reviews and updates the person’s care plan. Every attempt is made to protect the person without using restraints. Sometimes they are needed. Restraints are used only as a last resort to protect persons from harming themselves or others.
History of restraint use
Restraints were once thought to prevent falls. Research shows that restraints cause falls. Falls occur when persons try to get free of the restraints. Injuries are more serious from falls in restrained persons than in those not restrained.
Restraints also were used to prevent wandering or interfering with treatment. They were often used for persons who showed confusion, poor judgment, or behavior problems. Older persons were restrained more often than younger persons were. Restraints were viewed as necessary devices to protect a person. However, they can cause serious harm (Box 14-1). They can even cause death.
Besides the CMS, the Food and Drug Administration (FDA), state agencies, and The Joint Commission (TJC—an accrediting agency) have guidelines for the use of restraints. They do not forbid the use of restraints. However, they require considering or trying all other appropriate alternatives first.
Every center has policies and procedures about restraints. They include identifying persons at risk for harm, harmful behaviors, restraint alternatives, and proper restraint use. Staff training is required.
Restraint alternatives
Often there are causes and reasons for harmful behaviors. Knowing and treating the cause can prevent restraint use. The nurse tries to find out what the behavior means. This is very important for persons who have speech or cognitive problems. The focus is on these questions:
• Is the person in pain, ill, or injured?
• Is the person short of breath? Are cells getting enough oxygen (Chapter 28)?
• Is the person afraid in a new setting?
• Does the person need to use the bathroom?
• Is a dressing tight or causing other discomfort (Chapter 35)?
• Is clothing tight or causing other discomfort?
• Is the person’s position uncomfortable?
• Are body fluids, secretions, or excretions causing skin irritation?
• Is the person too hot or too cold?
• Is the person hungry or thirsty?
• What are the person’s life-long habits at this time of day?
• Does the person have problems communicating?
• Is the person seeing, hearing, or feeling things that are not real (Chapter 43)?
• Is the person confused or disoriented (Chapter 44)?
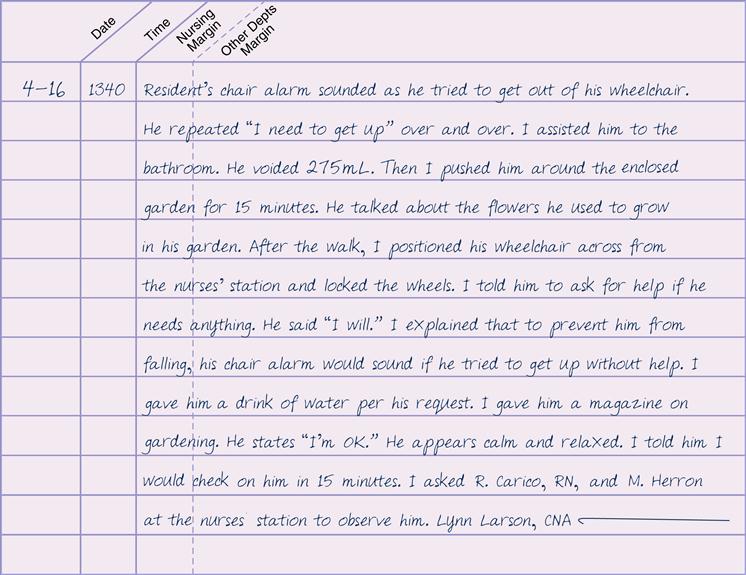
Restraint alternatives for the person are identified (Box 14-2). They become part of the care plan. Care plan changes are made as needed. Restraint alternatives may not protect the person. The doctor may need to order restraints. See Figure 14-3.
Box 14-2
• Diversion is provided—TV, videos, music, games, relaxation tapes, and so on.
• Family and friends make videos of themselves for the person to watch.
• Videos are made of visits with family and friends for the person to watch.
• Time is spent in supervised areas (dining room, lounge, near the nurses’ station).
• Pillows, wedge cushions, and posture and positioning aids are used.
• The signal light is within reach.
• Signal lights are answered promptly.
• Food, fluid, hygiene, and elimination needs are met.
• The bedpan, urinal, or commode is within the person’s reach.
• Family, friends, and volunteers visit.
• The person has companions or sitters.
• Time is spent with the person.
• Extra time is spent with a person who is restless.
• Reminiscing is done with the person.
• A calm, quiet setting is provided.
• The person wanders in safe areas.
• Exercise programs are provided.
• Outdoor time is planned during nice weather.
• The person does jobs or tasks he or she consents to.
• Warning devices are used on beds, chairs, and doors.
• Knob guards are used on doors.
• Padded hip protectors are worn under clothing (Fig. 14-1).
• Floor cushions are placed next to beds (Chapter 13).
• Roll guards are attached to the bed frame (Fig. 14-2).
• Falls are prevented (Chapter 13).
• The person’s furniture meets his or her needs (lower bed, reclining chair, rocking chair).
• Walls and furniture corners are padded.
• Observations and visits are made at least every 15 minutes. Or as often as noted in the care plan.
• The person is moved to a room close to the nurses’ station.
• Procedures and care measures are explained.
• Frequent explanations are given about equipment or devices.
• Confused persons are oriented to person, time, and place. Calendars and clocks are provided.
• Light is adjusted to meet the person’s basic needs and preferences.
• Staff assignments are consistent.


Safe restraint use
Restraints can cause serious injury and even death.  CMS, OBRA, FDA, and TJC guidelines are followed. So are state laws. They are part of your center’s policies and procedures for restraint use.
CMS, OBRA, FDA, and TJC guidelines are followed. So are state laws. They are part of your center’s policies and procedures for restraint use.
 Restraints are not used to discipline a person. They are not used for staff convenience. Discipline is any action that punishes or penalizes a person. Convenience is any action that:
Restraints are not used to discipline a person. They are not used for staff convenience. Discipline is any action that punishes or penalizes a person. Convenience is any action that:
• Controls or manages the person’s behavior
• Requires less effort by the center
• Is not in the person’s best interests
Restraints are used only when necessary to treat a person’s medical symptoms. The CMS defines a medical symptom as an indication or characteristic of a physical or psychological condition. Symptoms may relate to physical, emotional, or behavioral problems. Sometimes restraints are needed to protect the person or others. That is, a person may have violent or aggressive behaviors that are harmful to self or others.
Physical and chemical restraints
 According to the CMS, physical restraints include these points:
According to the CMS, physical restraints include these points:
• May be any manual method, physical or mechanical device, material, or equipment
• Is attached to or next to the person’s body
• Cannot be easily removed by the person
• Restricts freedom of movement or normal access to one’s body
Physical restraints are applied to the chest, waist, elbows, wrists, hands, or ankles. They confine the person to a bed or chair. Or they prevent movement of a body part. Some furniture or barriers also prevent freedom of movement:
• A device used with a chair that the person cannot remove easily. The device prevents the person from rising. Trays, tables, bars, and belts are examples (Fig. 14-4).
• Any chair that prevents the person from rising.
• Any bed or chair placed so close to the wall that the person cannot get out of the bed or chair.
• Bed rails (Chapter 13) that prevent the person from getting out of bed. For example, four half-length bed rails are raised. They are restraints if the person cannot lower them.

Drugs or drug dosages are chemical restraints if they:
Drugs cannot be used for discipline or staff convenience. They cannot be used if not required for the person’s treatment. They cannot be used if they affect physical or mental function.
Sometimes drugs can help persons who are confused or disoriented. They may be anxious, agitated, or aggressive. The doctor may order drugs to control these behaviors. The drugs should not make the person sleepy and unable to function at his or her highest level.
Complications of restraint use
Box 14-1 lists the many complications from restraints. Injuries occur as the person tries to get free of the restraint. Injuries also occur from using the wrong restraint, applying it wrong, or keeping it on too long. Cuts, bruises, and fractures are common. The most serious risk is death from strangulation.
There are also mental effects. Restraints affect dignity and self-esteem. See Box 14-1.
Restraints are medical devices. The Safe Medical Device Act applies if a restraint causes illness, injury, or death.  Also, CMS requires the reporting of any death that occurs:
Also, CMS requires the reporting of any death that occurs:
Legal aspects
Laws applying to restraint use must be followed. Remember the following:
 Restraints must protect the person. They are not used for staff convenience or to discipline a person. Restraining someone is not easier than properly supervising and observing the person. A restrained person requires more staff time for care, supervision, and observation. A restraint is used only when it is the best safety measure for the person. Restraints are not used to punish or penalize uncooperative persons.
Restraints must protect the person. They are not used for staff convenience or to discipline a person. Restraining someone is not easier than properly supervising and observing the person. A restrained person requires more staff time for care, supervision, and observation. A restraint is used only when it is the best safety measure for the person. Restraints are not used to punish or penalize uncooperative persons. A doctor’s order is required. OBRA, CMS, state laws, FDA warnings, TJC, and other accrediting agencies protect persons from unnecessary restraint. If restraints are needed for medical reasons, a doctor’s order is required. The doctor gives the reason for the restraint, what body part to restrain, what to use, and how long to use it. This information is on the care plan and your assignment sheet. In an emergency, the nurse can decide to apply restraints before getting a doctor’s order.
A doctor’s order is required. OBRA, CMS, state laws, FDA warnings, TJC, and other accrediting agencies protect persons from unnecessary restraint. If restraints are needed for medical reasons, a doctor’s order is required. The doctor gives the reason for the restraint, what body part to restrain, what to use, and how long to use it. This information is on the care plan and your assignment sheet. In an emergency, the nurse can decide to apply restraints before getting a doctor’s order. The least restrictive method is used. It allows the greatest amount of movement or body access possible. Some restraints attach to the person’s body and to a fixed (non-movable) object. It restricts freedom of movement or body access. Vest, jacket, ankle, wrist, hand, and some belt restraints are examples. Other restraints are near but not directly attached to the person’s body (bed rails or wedge cushions). They do not totally restrict freedom of movement. They allow access to certain body parts and are the least restrictive.
The least restrictive method is used. It allows the greatest amount of movement or body access possible. Some restraints attach to the person’s body and to a fixed (non-movable) object. It restricts freedom of movement or body access. Vest, jacket, ankle, wrist, hand, and some belt restraints are examples. Other restraints are near but not directly attached to the person’s body (bed rails or wedge cushions). They do not totally restrict freedom of movement. They allow access to certain body parts and are the least restrictive.• Restraints are used only after other measures fail to protect the person (see Box 14-2). Some people can harm themselves or others. The care plan must include measures to protect the person and prevent harm to others. Many fall prevention measures are restraint alternatives (Chapter 13).
• Unnecessary restraint is false imprisonment (Chapter 4). You must clearly understand the reason for the restraint and its risk. If not, politely ask about its use. If you apply an unneeded restraint, you could face false imprisonment charges.
 Informed consent is required. The person must understand the reason for the restraint. The person is told how the restraint will help the planned medical treatment. The person is told about the risks of restraint use. If the person cannot give consent, his or her legal representative is given the information. Either the person or the legal representative must give consent before a restraint can be used. The doctor or nurse provides the necessary information and obtains the consent.
Informed consent is required. The person must understand the reason for the restraint. The person is told how the restraint will help the planned medical treatment. The person is told about the risks of restraint use. If the person cannot give consent, his or her legal representative is given the information. Either the person or the legal representative must give consent before a restraint can be used. The doctor or nurse provides the necessary information and obtains the consent.See Focus on Communication: Legal Aspects.
FOCUS ON COMMUNICATION
Legal Aspects
You may not know the reason for a restraint. If so, politely ask the nurse why it is needed. For example:
• “Why does Mr. Reed need a restraint?”
• “I don’t understand. Why did the doctor order the restraint?”
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


