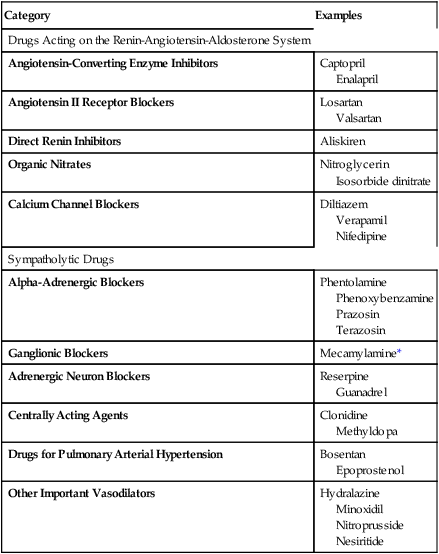
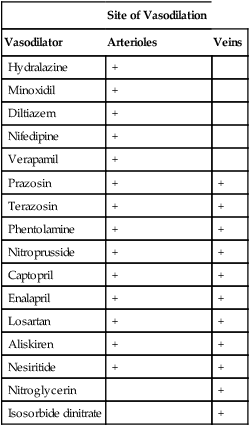
CHAPTER 46 Vasodilation can be produced with a variety of drugs. The major classes of vasodilators, along with representative agents, are listed in Table 46–1. Some of these drugs act primarily on arterioles, some act primarily on veins, and some act on both types of vessel. The vasodilators are widely used, with indications ranging from hypertension to angina pectoris to heart failure. Many of the vasodilators have been discussed in previous chapters. Three agents—hydralazine, minoxidil, and nitroprusside—are introduced here. TABLE 46–1 Vasodilators differ from one another with respect to the types of blood vessels they affect. Some agents (eg, hydralazine) produce selective dilation of arterioles. Others (eg, nitroglycerin) produce selective dilation of veins. Still others (eg, prazosin) dilate arterioles and veins. The selectivity of some important vasodilators is summarized in Table 46–2. TABLE 46–2 Because hemodynamic responses to dilation of arterioles and veins differ, the selectivity of a vasodilator is a major determinant of its effects, both therapeutic and undesired. Undesired effects related to selective dilation of arterioles and veins are discussed below. Therapeutic implications of selective dilation are discussed in Chapters 47, 48, 51, 53, and 107—the chapters in which the primary uses of the vasodilators are presented.
Vasodilators

Category
Examples
Drugs Acting on the Renin-Angiotensin-Aldosterone System
Angiotensin-Converting Enzyme Inhibitors
Captopril
Enalapril
Angiotensin II Receptor Blockers
Losartan
Valsartan
Direct Renin Inhibitors
Aliskiren
Organic Nitrates
Nitroglycerin
Isosorbide dinitrate
Calcium Channel Blockers
Diltiazem
Verapamil
Nifedipine
Sympatholytic Drugs
Alpha-Adrenergic Blockers
Phentolamine
Phenoxybenzamine
Prazosin
Terazosin
Ganglionic Blockers
Mecamylamine*
Adrenergic Neuron Blockers
Reserpine
Guanadrel
Centrally Acting Agents
Clonidine
Methyldopa
Drugs for Pulmonary Arterial Hypertension
Bosentan
Epoprostenol
Other Important Vasodilators
Hydralazine
Minoxidil
Nitroprusside
Nesiritide
Basic concepts in vasodilator pharmacology
Selectivity of vasodilatory effects

Site of Vasodilation
Vasodilator
Arterioles
Veins
Hydralazine
+
Minoxidil
+
Diltiazem
+
Nifedipine
+
Verapamil
+
Prazosin
+
+
Terazosin
+
+
Phentolamine
+
+
Nitroprusside
+
+
Captopril
+
+
Enalapril
+
+
Losartan
+
+
Aliskiren
+
+
Nesiritide
+
+
Nitroglycerin
+
Isosorbide dinitrate
+
Vasodilators



Get Clinical Tree app for offline access
