Toxicology
Objectives
After completing this chapter you should be able to:
Fundamental Concepts
1. List the most common illicit drugs used in the United States.
2. Describe the widely used and abused legal drug ethanol (alcohol).
3. Identify the types of specimens commonly used for drug testing.
4. Explain why urine specimens are so good for drug screening tests.
CLIA-Waived Immunology Tests
Advanced Concepts
1. Define and elaborate on therapeutic drug monitoring.
2. List examples of therapeutic drugs that may require monitoring.
3. Describe the five steps in pharmacokinetics.
4. Discuss the meaning of “drug half-life.”
5. List the most common poisonous metals, and cite a source for each.
Key Terms
absorption passage of a substance through the surface of the body into body fluids and tissues
buprenorphine an FDA-approved drug for treating opioid drug addiction
cannabinoid marijuana
distribution the blood then carries the drug through the body
idiosyncrasy an abnormal susceptibility to a drug or other agent that is peculiar to the individual
liberation the release of a prescribed drug from its dosage
metabolite a substance produced by the metabolism of a drug in the body
opiates methadone and morphine
pharmacokinetics the movement of drugs through the body from the time of introduction to elimination
qualitative drug screening a measurement that determines if a substance is present or absent
quantitative drug screening a precise measurement of the amount of a substance present in the specimen
toxicity the level at which a drug becomes poisonous in the body
 FUNDAMENTAL CONCEPTS
FUNDAMENTAL CONCEPTS
Overview of Toxicology
The toxicology department in the medical laboratory tests the levels of both therapeutic drugs and drugs of abuse to determine their presence and/or their harmful or “toxic” effect on the body. These departments may also test for other poisons, such as lead. In the toxicology laboratory, tests are generally performed using blood or urine specimens and sometimes saliva, sweat, or stomach contents. A toxicology test may be for one specific drug or more than 20 drugs.
Drugs may be accidentally or deliberately injected, inhaled, swallowed, or absorbed through the skin or mucous membranes. Toxicity is the level at which a drug becomes poisonous in the body.
The medical assistant may be responsible for collecting the urine or blood specimen, which is then sent to the toxicology lab, also for testing the specimen for screening or monitoring purposes. The following are common reasons for performing drug screening tests:
The fundamental concepts section of this chapter includes an overview of the common drugs of abuse that can become toxic and/or addictive when taken incorrectly. It then describes proper collection of urine and blood specimens used for drug testing. When testing for drugs of abuse, the medical assistant must ensure that collection of the specimen adheres to the legal “chain of custody” guidelines certifying that the collection of the specimen was witnessed and there was no opportunity for the specimen to be tampered with in any way.
The CLIA-waived section presents in-office drug screening tests and the procedure for monitoring patients on buprenorphine (a Food and Drug Administration [FDA]–approved drug for treating drug addiction).
The advanced concepts section presents the principles of therapeutic drug monitoring and collecting a blood specimen for lead poisoning.
Drugs of Abuse
There are thousands of drugs available worldwide. Over-the-counter (OTC) drugs fill the shelves of pharmacies and are useful for many minor medical conditions. Unfortunately, these drugs may have toxic effects on the body if taken incorrectly. Three causes of drug toxicity with OTCs are overdosage, interactions with other drugs, or idiosyncrasy (an abnormal susceptibility to a drug or other agent that is peculiar to the individual). The medical assistant should be mindful of these possibilities and faithfully record any OTC drugs that are being taken.
Any drug can be abused, but “drugs of abuse” are considered to be those that are illegally obtained for recreational purposes or to satisfy an addiction. Some therapeutic drugs may be misused or become addictive over time. Table 9-1 lists the 13 most common illicit or addictive drugs of abuse. Note the number of these drugs that also have medical uses when taken appropriately.
TABLE 9-1
Common Drugs of Abuse Detected on Multiple Drug Urine Screening Tests∗
| Drug and (Test Code) | Street Name | Source/Route | Medical Use/Brand Names | Side Effects, Risks/Overdose |
| 1. Cocaine (COC) | Rock, crack, coke, blow, nose nachos, hooter, yeyo | Coca bush leaves refined/Nasal administration, smoked | Topical anesthetic, natural stimulant, anesthetic, vasoconstrictor, painkiller, appetite suppressant, altitude sickness/Less addictive derivatives for anesthesia: Benzocaine, Lidocaine, Cepacol, Dermaplast, Lanocane | Perforation of nasal septum, renal failure, hyperthermia, cardiac arrest, seizures, dermatitis, tetany, septicemia, respiratory arrest, dehydration, sleep disorders, depression, impulsiveness, hostility, impaired memory/Overdose: fever, unresponsiveness, difficulty breathing, unconsciousness, stroke, death |
| 2. Amphetamine (AMP) | Black beauties, Christmas trees, dexies, speed, double trouble, gaggler, beanies | Made in illegal laboratories/Smoked, injected, snorted | Appetite suppressant, central nervous system stimulant/Adderall, Citramine, Dexalone, Tamphetamin, Zamitam | Dependence, increased blood pressure, increased respiration, dilated pupils, sweating, tremors/Overdose: seizures, cardiac arrest |
| 3. Methamphetamine (mAMP) | Cat, crank, glass, speed, ice, love, | Made in illegal laboratories/Oral, powder inhalant, crystals smoked, | Nasal decongestant/Desoxyn, | Dependence, psychosis, decreased appetite, restlessness, anxiety, heart failure, extreme fatigue, hunger, mental depression, dysrhythmias, lethargy, skin pallor, fits of rage/Overdose: seizures, cardiac arrest |
| Ecstasy XTC (MDMA) | Disco biscuits, Molly | No medical use | ||
| 4. Marijuana (THC) | Pot, weed, joint, reefer, roach, dope | Cannabis sativa, hemp plant flowers and leaves/Smoked, eaten, injected | Pain relief (colitis), treatment of glaucoma, appetite stimulant, reduction of nausea from chemotherapy, euphoria, detachment, relaxation/Marinol, Dronabinol | Talkativeness, slowed time perception, inappropriate hilarity, paranoia, confusion, anxiety, short-term memory loss, impaired lung structure, chromosomal mutation, micronucleic white blood cells, cancer, lack of motivation |
| Hashish | Hashish, hash oil, ganja | |||
| 5. Methadone (MTD) | Fizzies, chocolate chip cookies, juice, wafer | Laboratory manufactured/Oral, injection, powder | Treatment for narcotic addiction, pain/Methadose, Dolophine | Also addictive/can result in respiratory and cardiac arrest and death if stopped suddenly |
| 6. Opiates (OPI 2000) (also see MOP 300) | Smack, horse, chiva, junk, black tar, gunpowder, courage pills, bomb | Poppy refined/nasal, oral, intravenous injection, dermal patch | Potent painkiller, heroin, morphine, codeine, fentanyl/Demerol, Darvon, Vicodin, Dilaudid | Addiction in hospitals, constipation, dermatitis, malnutrition, hypoglycemia, dental caries, amenorrhea, acquired immunodeficiency syndrome (from sharing needles) |
| 7. Oxycodone (OXY) | Oxy, OC, blues, killers, kickers hillbilly percs | Semisynthetic similar to codeine/Oral, injection | Moderate to heavy pain relief/OxyContin, Percodan, Percocet | Addiction in patients on long-term pain therapy |
| 8. Barbiturates (BAR) | Barbs, pinks, blockbusters, Christmas trees, goofballs, red devils, reds and blues, yellowjackets | Laboratory manufactured/Oral, intravenous injection | Depressant, sedative, hypnotic, anticonvulsant/Seconal, Amytal, Nembutal | Dullness, apathy, dependence/Overdose: respiratory arrest, coma, death |
| 9. Benzodiazepines (BZO) | Roofies, downers, tranks, benzos | Laboratory manufactured/Oral, injection | Treatment for anxiety, seizures, sleeplessness, muscle relaxant/Valium, Xanax, Restoril, Versed | Carefree, detached, sleepy, disoriented, unconsciousness, amnesia, diminished reflexes/Overdose: coma, can be lethal when combined with alcohol |
| 10. Buprenorphine (BUP) | Bupe, Subs | Laboratory manufactured | Analgesic, treatment for opioid addiction/Buprenex, Suboxone, Subutix | Euphoria, respiratory depression, sedation/Causes severe respiratory depression when combined with benzodiazepines |
| 11. Tricyclic antidepressants (TCA) | Yellow | Laboratory manufactured/Oral, injection | Treatment for depression, attention-deficit/hyperactivity disorder, migraines/Adapin, Norpramin, Anafranil, Pamelor, Tofranil, Elavil | Blurred vision, constipation and dry mouth, anxiety, restlessness, difficulty urinating, weight gain, drowsiness, muscle twitches, weakness, sweating, nausea, dizziness, cognitive and memory difficulties, increased heart rate, irregular heart rhythms, panic attacks, hostile/angry feelings, impulsive actions, severe restlessness, very rapid speech |
| 12. Lysergic acid diethylamide (LSD) | Acid, the Beast, California sunshine | Illicit laboratories, peyote (mescaline), psilocybin mexicana (mushroom), fungus on grains/Ingested orally | No medical use | Hallucinations, anxiety, depression, confusion, paranoia, panic attacks, impaired memory, inability to reason, flashbacks, increased blood pressure, high temperature, dilated pupils, increased heart rate, psychosis, flashbacks |
| 13. Phencyclidine (PCP) | Angel dust, peace pill, rocket fuel, wack, ozone, fry | Illegal laboratories/Oral, intravenous, sniffed, smoked | No medical use | Hallucinations, acute anxiety, dulled thinking, poor memory, depression, severe brain damage, hepatitis, respiratory arrest, panic reaction, confusion, blurred vision, high blood pressure/Overdose: violence, psychoses, self-injurious behavior, suicide |
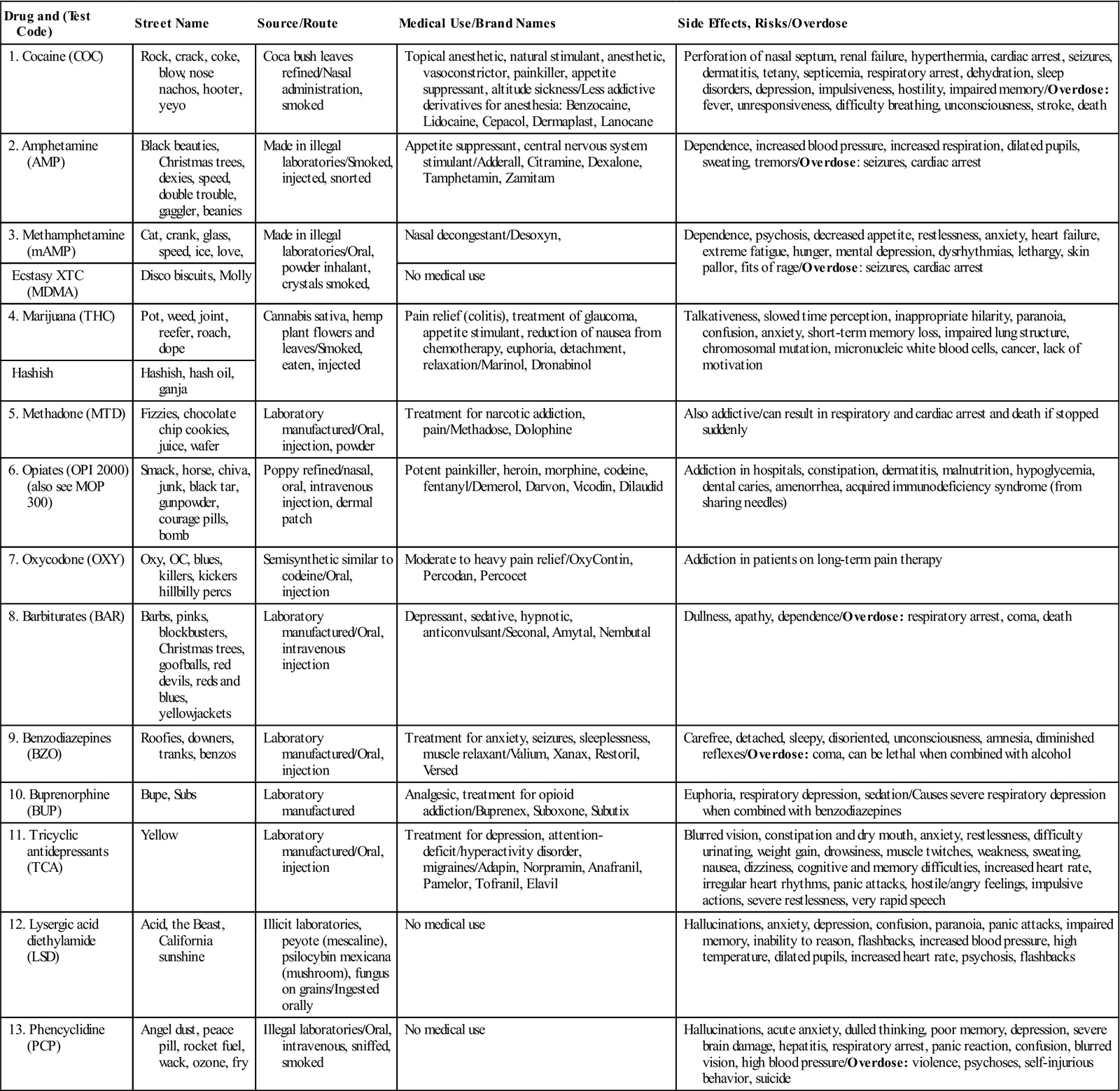
∗Numbers 1 through 9 are the screened drugs for patients on Number 10, buprenorphine therapy (see Procedure 1–9).
Each of the drugs in Table 9-1 produces a specific metabolite, the substance produced by metabolism (breaking down) of the drug in the body. The metabolite is then excreted in the urine. These metabolites can be tested qualitatively in the same way that the urine dipstick tested for various analytes (e.g., glucose, protein). Urine is generally the specimen of choice for screening drugs of abuse because it is easily obtained and it is relatively simple to perform multiple drug tests at the same time. Table 9-2 lists the time intervals for detecting various drugs in urine. Also, see Procedure 9-1, located at the end of this section.
TABLE 9-2
Typical Time Intervals for Detecting Drugs in Urine
| Drug | Time Found in Urine |
| Alcohol | 6 hours to 1 day |
| Amphetamines | 4 hours |
| Barbiturates | 24 hours to 4 days |
| Benzodiazepines | Short-term therapeutic use: 3 days; long-term chronic use: 4 to 6 weeks |
| Cannabinoids | 1 hour to 3 days |
| Cocaine | 2 to 3 days |
| Codeine | 4 hours |
| LSD | 1 to 4 days |
| Marijuana (THC) | Casual use: up to 7 days; chronic use: up to 30 days or longer |
| MDMA (Ecstasy) | 1 to 4 days |
| Methadone | 1 to 7 days |
| Methamphetamine | 1 to 4 days |
| Opiates | 1 to 4 days |
| PCP | Casual use: up to 7 days; chronic use: up to 30 days |
| Tricyclic antidepressants | 1 to 9 days |
Modified from Stepp CA, Woods M: Laboratory procedures for medical office personnel, Philadelphia, 1998, Saunders.
If a quantitative result is necessary to determine the amount of the drug that is in the patient, a blood specimen would also be used because its dilution stays constant. The dilution of the drug in the urine volume varies depending on water intake and output. The blood specimen is commonly ordered by law enforcement officials who need to know the actual amount of a specific illicit drug after it has tested positive in the urine.
The most common legal drug of abuse in America is ethanol, also known as grain alcohol. It is found in beer, wine, and distilled liquors. Table 9-3 lists the approximate ethanol content in alcoholic beverages. Ethanol depresses the central nervous system and may lead to coma, progressing to death at the following “panic” levels:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


