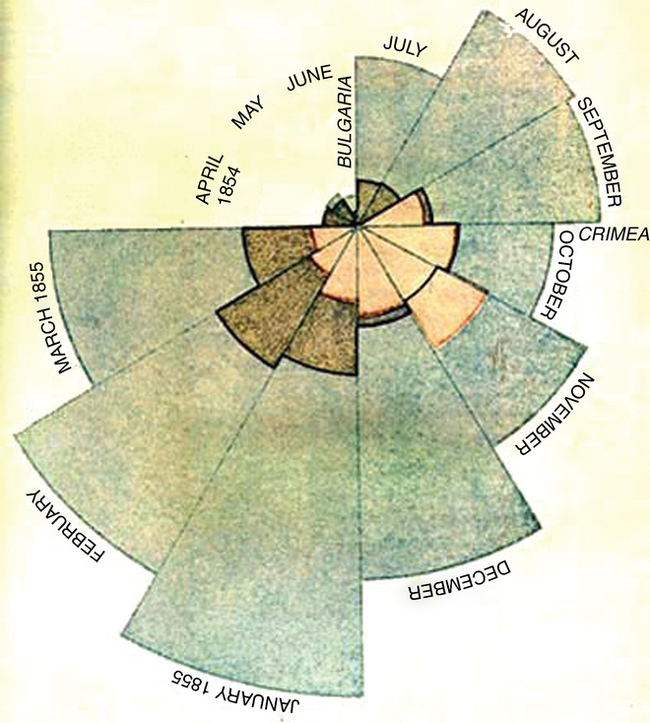
After studying this chapter, students will be able to: • Differentiate among bench, clinical, and translational science. • Describe the historical development of the scientific method. • Give examples of inductive and deductive reasoning. • Discuss the limitations of the scientific method when applied to nursing. • Differentiate between problem solving and research. • List the steps in the research process. • Discuss contributions nursing research has made to nursing practice and to health care. • Describe the relationship of nursing research to nursing theory and practice. • Identify sources of support for nursing research. • Discuss the roles of nurses in research at various levels of education. To enhance your understanding of this chapter, try the Student Exercises on the Evolve site at http://evolve. elsevier.com/Black/professional. Chapter opening photo from istockphoto.com. Mature professions have a strong scientific base, which both defines and is defined by the purposes of a profession. Florence Nightingale, whose work is detailed in Chapter 2, advanced the practice of nursing by both defining it clearly and providing scientific evidence of the outcomes of excellent nursing care in the Crimea. Figure 11-1 shows her careful documentation of the improvement in morbidity and mortality among soldiers in Bulgaria and the Crimea over a course of a year. In the mid-twentieth century, scholars and researchers realized that nursing could achieve a high level of professional status only to the extent that the discipline was based on a scientific body of knowledge unique to nursing. As a result, nursing researchers began developing knowledge unique to nursing, and nursing theorists began developing theories and testing them. Theory and research are the foundations of scientifically based nursing practice. At the same time, nurses realized that professionalization of patient care practices was also needed. Until that time, nurses relied on traditional techniques to manage common patient problems. More unusual problems were often managed by trial and error or intuition. However, these were no longer acceptable ways to care for patients. The impetus toward evidenced-based practice was emerging, which required nurses to base their care and activities on research-based knowledge. This necessitates a strong link between the work of nurse researchers and nurses in practice. The development of the nursing process became a means of adapting a scientific framework to the management of patient care so that nurses were no longer depending on hit-or-miss techniques but were shaping care in direct response to the individual needs of the patient. The nursing process is presented in depth in Chapter 8. Furthermore, the American Nurses Credentialing Center (ANCC) Magnet Recognition Program, described in Chapters 3 and 10, includes in its Magnet Model a component “New Knowledge, Innovation, and Improvements” (www.nursecredentialing.org/MagnetModel.aspx). Inclusion of this requirement for hospitals seeking to attain Magnet status underscores the importance for nursing to be responsible for the development, maintenance, and application of its own professional scientific knowledge base. The Magnet Model requires that initiatives and leadership for nursing research reside with clinical nurses, not nurse managers or others in administrative positions. Science is research based on one or more past scientific achievements or accomplishments that are acknowledged by the scientific (academic) community as providing a foundation for further study or practice (Kuhn, 1970). Good science—that which contributes to the knowledge bases of a discipline—requires that research be based on the previous work of others in the same academic discipline or be related to work of others from other disciplines. This is a safeguard that ensures that knowledge development is based on sound principles and theory rather than simply the product of a creative idea that is not based on any known science. Sound science and creativity are not mutually exclusive; creativity has led to many interesting and useful research developments that in turn guide nursing practice. Conclusions drawn through deductive processes are called valid rather than true. “Valid” is a term meaning “soundly founded,” whereas “true” means “in accordance with the fact or reality” (Flexner, Stein, Su, 1980). It is possible for a conclusion to be solidly founded without being true for everyone. There is a subtle but real difference between the words “valid” and “true.” For example, the premise that women benefit from centering care may be valid; this is soundly founded in the original findings of the researcher who interviewed 25 women. What is not true, however, is that all women benefit from centering care. The premise is valid but not true in all cases. The traditional scientific method used by quantitative researchers has considerable value, and it has been used by nurse researchers to address a wide range of nursing problems (Polit and Beck, 2004). However, the scientific method as implemented exclusively with quantitative techniques has limitations when applied to phenomena of interest to nursing. 1. A conceptual framework exists or can be constructed from research that already has been done; that is, the researcher’s ideas about the problem fit logically and align with what is already known about the topic. 2. The proposed research project is based on related research findings published in professional peer-reviewed journals or is supported by similar ongoing research in other settings or disciplines, thereby building nursing knowledge. 3. The proposed research is carefully designed so that the results will be applicable in similar situations or will generate hypotheses for further research and testing. Thus although nursing research may be broadly defined as anything that interests nurses and helps them provide better care, controversy exists over what can legitimately be included. When considering a research question, the wise nurse researcher considers the practical issues of background and financial support. An important source of funding and support for nursing research is the NIH’s National Institute for Nursing Research (NINR), created in 1992 from what had previously been known as the National Center for Nursing Research. NINR states its goal is to “advance nursing science by supporting research on the science of health, which focuses on the promotion of health and quality of life” (NINR, 2011). To advance the science of health, NINR has identified five strategic areas in which it will invest. These areas, in addition to NINR’s mission statement, are included in Box 11-1. Mrs. Abney’s case is an example of problem solving, an effective intervention in one set of circumstances that has immediate application. However, the solution that worked for Mrs. Abney may not work for all confused patients. In fact, it may not continue to work for Mrs. Abney if her cognitive abilities decline further. Remember that nursing research was developed in response to the professional and scientific mandate that nursing care be based in evidence and not simply on trial and error. Occasionally, creative problem solving such as that of Mrs. Abney’s nurse is required on a per-case, situational basis. But this sort of trial-and-error problem-solving approach is not adequate to base one’s professional practice in a substantial and sustained way. Table 11-1 contrasts research and problem solving. TABLE 11-1 COMPARISON OF RESEARCH AND PROBLEM SOLVING
The science of nursing and evidence-based practice

Science and the scientific method
Inductive and deductive reasoning
Limitations of the strict definition of scientific method in nursing
What is nursing research?
CHARACTERISTIC
RESEARCH
PROBLEM SOLVING
Type of problems addressed
Significant number of people affected or significant impact on smaller number of people
Situation-specific
Conceptual basis
Theoretical framework; keys to researching the problem found in previous research
Often none; trial and error
Knowledge base needed
Extensive review of literature to determine latest thinking and research
Practical knowledge, common sense, and experience
Scope of application
Generalizable or transferable to similar situations
Useful in immediate situation; may or may not be useful in other situations ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The science of nursing and evidence-based practice
Get Clinical Tree app for offline access
