Chapter 6
The Head and Neck
A lady, aged twenty, became affected with some symptoms which were supposed to be hysterical. … After she had been in this nervous state about three months it was observed that her pulse had become singularly rapid. … She next complained of weakness on exertion and began to look pale and thin. … It was observed that the eyes assumed a singular appearance, for the eyeballs were apparently enlarged. In a few months … a tumour, of a horseshoe shape, appeared on the front of the throat and exactly in the situation of the thyroid gland.
Robert James Graves (1796–1853)
General Considerations
The appearance of the head and face, their contours and texture, often provides the first insight into the nature of illness. Sunken cheeks, wasting of the temporal muscles, and flushing of the face are important visible clues of systemic illness. Some facial appearances are pathognomonic of disease. The pale, puffy face of nephritis, the startled expression of hyperthyroidism, and the immobile stare of parkinsonism are examples of classic facies.
The appearance of the patient’s face may also provide information regarding psychologic makeup: is the person happy, sad, angry, or anxious?
Thyroid disease takes many forms. The World Health Organization estimates that more than 200 million people in the world have enlarged thyroid glands, a condition known as goiter. Asians first described goiter around 1500 BCE. Even at that time, they recognized that seaweed in the diet tended to make goiters smaller. Iodine was not discovered until the nineteenth century, but it is now believed that those goiters were related to an iodine deficiency that was partially corrected by the iodine in the seaweed.
The ancient Greeks and Romans recognized that when a thin thread tied around the neck of a newly married woman broke, she was pregnant. This was caused by an increase in the size of the thyroid during pregnancy.
Thyroid cancer is the most common endocrine cancer, and its incidence has increased by approximately 3% per 100,000 people per year. In 2011, there were 48,020 new cases of thyroid cancer. Of these new cases, approximately 11,470 occurred in men and 36,550 occurred in women. Thyroid is the fifth leading site of new cancers in women. The incidence rate of thyroid cancer has been increasing sharply since the mid-1990s, and it is the fastest increasing cancer in both men and women. There were 1740 deaths in 2011 from thyroid cancer: 760 in men and 980 in women. The death rate for thyroid cancer has been increasing in men and stable in women. Risk factors include radiation exposure related to medical treatment during childhood. The 5-year survival rate for all thyroid cancer patients is 97%. Survival, however, varies markedly by stage, age of diagnosis, and disease subtype. The 5-year survival rate approaches 100% for localized disease, is 97% for regional stage disease, and 58% for distant stage disease.
In the United States, cancer of the head and neck constitutes approximately 5% of all malignancies in men and 3% in women. Head and neck cancer includes cancers of the mouth, nose, sinuses, salivary glands, throat, and lymph nodes in the neck. Most begin in the moist tissues that line the mouth, nose, and throat. Symptoms include a lump or sore in the mouth that does not heal, a persistent sore throat, trouble swallowing, or a change or hoarseness in the voice. Using tobacco or alcohol increases the risk of developing head and neck cancer. In fact, 85% of all head and neck cancers are linked to tobacco use. If found early, these cancers may be curable. Treatment can include surgery, radiation therapy, chemotherapy, or a combination, but these treatments may affect eating, speaking, or even breathing.
In 2011, there were 39,400 (27,710 men and 11,690 women) new cases of head and neck cancer and 7900 related deaths. It has been estimated that nearly 90% of these cases are associated with poor dental hygiene, tobacco use, exposure to nickel, and alcohol use. Tobacco, whether chewed, smoked, or simply kept in the buccal pouch, predisposes an individual to tumors of the upper aerodigestive tract. Pipe smokers and tobacco chewers are at risk for tumors of the oral cavity, and the Chinese are at risk for nasopharyngeal carcinomas. On the basis of rates from 2002 to 2004, it is estimated that 1.02% of both sexes born in 2007 in the United States will receive diagnoses of cancer of the oral cavity and pharynx at some time during their lifetime.
Structure and Physiology
The Head
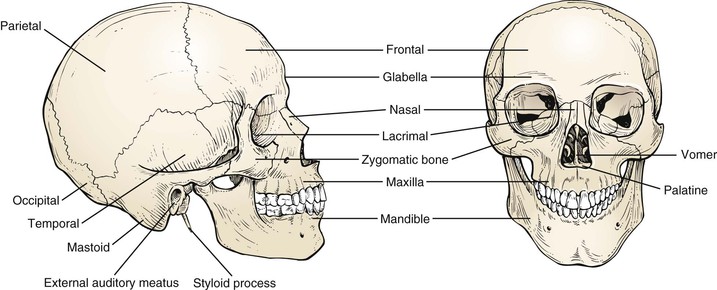
The skull is composed of 22 bones, 14 in the face alone. This bony structure acts as a support and protection for the softer tissues within.
The facial skeleton is composed of the mandible; the maxilla; and the nasal, palatine, lacrimal, and vomer bones. The unpaired mandible forms the lower jaw. The maxilla is an irregular bone and forms the upper jaw on each side. The nasal bones form the bridge of the nose. The other bones are not relevant to this discussion.
The main bones of the cranial skeleton include the frontal, temporal, parietal, and occipital bones. The frontal bones form the forehead. The temporal bones form the anterolateral walls of the brain. The mastoid process, which is part of the temporal bone, is particularly important in ear disease and is discussed in Chapter 8, The Ear and Nose. The parietal bones form the top and posterolateral portions of the skull. The occipital bones form the posterior portion of the skull. The bones of the face and skull are shown in Figure 6-1.
The orbicularis oculi muscle surrounds the eye. Its function is to close the eyelids. This muscle and its action are further discussed in Chapter 7, The Eye.
The platysma is a thin, superficial muscle of the neck, crossing the outer border of the mandible and extending over the lower anterior portion of the face. The main action of the platysma is to pull the mandible downward and backward, which results in a mournful facial expression.
The muscles of mastication include the masseter, pterygoid, and temporalis. These muscles insert on the mandible and effect chewing. The masseter is strong and thick and is one of the most powerful muscles of the face. The action of the masseter is to close the jaw by elevating and drawing the mandible backward. Tension in the masseter may be felt by clenching the jaw. Although important to jaw function, the other muscles of mastication are not clinically relevant to physical diagnosis and are not discussed here. The locations of these muscles are shown in Figure 6-2.
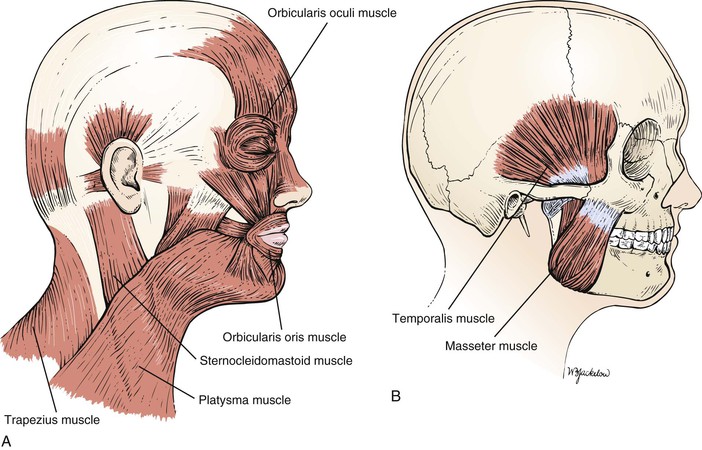
Figure 6–2 Muscles of the face and skull. A, The more superficial muscles. B, The underlying muscles.
The trigeminal, or fifth cranial, nerve carries sensory fibers from the face, oral cavity, and teeth and carries efferent motor fibers to the muscles of mastication. The major divisions of this nerve are discussed in subsequent chapters.
The Neck
The neck is divided by the sternocleidomastoid muscle into the anterior, or medial, triangle and the posterior, or lateral, triangle. These are illustrated in Figure 6-3.
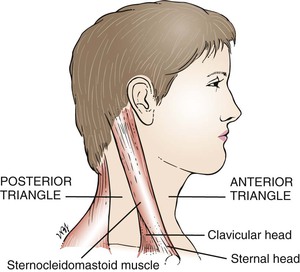
The sternocleidomastoid is a strong muscle that serves to raise the sternum during respiration. The sternocleidomastoid has two heads: The sternal head arises from the manubrium sterni, and the clavicular head originates on the sternal end of the clavicle. The two heads unite and insert on the lateral aspect of the mastoid process. The sternocleidomastoid is innervated by the spinal accessory, or eleventh cranial, nerve.
The thyroid gland envelops the upper trachea and consists of two lobes connected by an isthmus. It is the largest endocrine gland in the body. As seen from the front, the thyroid is butterfly-shaped and wraps around the anterior and lateral portions of the larynx and trachea, as shown in Figure 6-4.
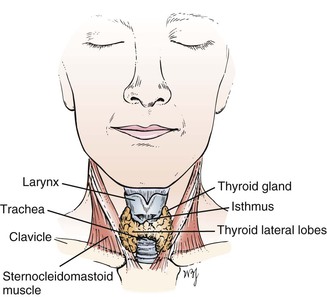
The thyroid isthmus lies across the trachea just below the cricoid cartilage of the larynx. The lateral lobes extend along both sides of the larynx, reaching the middle of the thyroid cartilage of the larynx. On occasion, the thyroid gland may extend downward and enlarge within the thorax, producing a substernal goiter. The function of the thyroid gland is to produce thyroid hormone in accordance with the needs of the body.
The pharynx and larynx are discussed in Chapter 9, The Oral Cavity and Pharynx.
The sternocleidomastoid muscle overlies the carotid sheath. The carotid sheath lies lateral to the larynx. This sheath contains the common carotid artery, the internal jugular vein, and the vagus nerve.
Posterior to the sternocleidomastoid is the posterior triangle. This is bounded by the trapezius muscle posteriorly and by the clavicle inferiorly. The posterior triangle also contains lymph nodes.
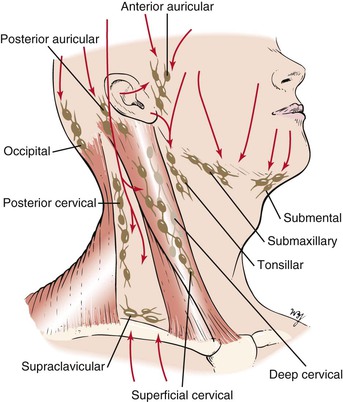
It has been estimated that the neck contains more than 75 lymph nodes on each side. The chains of these lymph nodes are named for their location. Starting posteriorly, they are the occipital, posterior auricular, posterior cervical, superficial and deep cervical (adjacent to the sternocleidomastoid muscle), tonsillar, submaxillary, submental (at the tip of the jaw in the midline), anterior auricular, and supraclavicular (above the clavicle) chains. Knowledge of lymphatic drainage is important because the presence of an enlarged lymph node may signal disease in the area draining into it. The main groups of lymph nodes and their drainage areas are shown in Figure 6-5.
Neck Mass
The most common symptom is a lump or swelling in the neck. Once a patient complains of a neck lump, ask the following questions:
“When did you first notice the lump?”
“Does the lump change in size?”
“Have you had any ear infections? Infections in your mouth?”
“Has there been hoarseness associated with the mass?”
“Is there a family history of thyroid cancer?”
“Is there a history of prior neck or thyroid gland radiation?”
If there is associated pain with a mass in the neck, an acute infection is likely. Masses that have been present for only a few days are commonly inflammatory, whereas those present for months are more likely to be neoplastic. A mass that has been present for months to years without any change in size often turns out to be a benign or congenital lesion. Blockage of a salivary gland duct may produce a mass that fluctuates in size while the patient eats.
The age of the patient is relevant in the assessment of a neck mass. A lump in the neck of a patient younger than 20 years of age may be an enlarged tonsillar lymph node or a congenital mass. If the mass is in the midline, it is most likely to be a thyroglossal cyst.1
From the ages of 20 to 40 years, thyroid disease is more common, although lymphoma must always be considered. When a patient is older than 40 years of age, a neck mass must be considered malignant until proved otherwise.
The location of the mass is also important. Midline masses tend to be benign or congenital lesions, such as thyroglossal cysts or dermoid cysts. Lateral masses are frequently neoplastic. Masses located in the lateral upper neck may be metastatic lesions from tumors of the head and neck, whereas masses in the lateral lower neck may be metastatic from tumors of the breast and stomach. One benign lateral neck mass is a branchial cleft cyst, which may manifest as a painless neck mass near the anterior upper third border of the sternocleidomastoid muscle.
Hoarseness associated with a thyroid nodule is suggestive of vocal cord paralysis resulting from impingement of the recurrent laryngeal nerve by tumor.
Neck Stiffness
If a patient complains of a stiff neck, ask the following questions:
“How long have you had the stiff neck?”
“Have you done any strenuous activity recently?”
“Are you aware of sleeping differently before the stiff neck occurred?”
“Do you have a headache associated with the stiff neck?”
“Have you had recent nausea or vomiting?”
“Have you noted unusual sleepiness?”
A stiff neck is typically characterized by soreness and difficulty moving the neck, especially when trying to turn the head to the side. A stiff neck may also be accompanied by a headache, neck pain, shoulder pain, or arm pain, and, in severe cases, may cause the individual to turn the entire body as opposed to the neck when trying to look sideways or backwards. By far the most common cause of a stiff neck is a muscle sprain or muscle strain, particularly to the levator scapula muscle. Located at the back and side of the neck, the levator scapula muscle connects the cervical spine (the neck) with the shoulder. This muscle is controlled by the third and fourth cervical nerves (C3, C4).
The levator scapula muscle may be strained or sprained throughout the course of many common activities, such as sleeping in a position that strains the neck muscles, sports injuries, rapid swimming, poor posture, stress, or holding the neck in an abnormal position for a long period.
The sudden occurrence of stiff neck, high fever, nausea, vomiting, sleepiness, or headache should raise suspicion of possible meningeal irritation. Any time a stiff neck is accompanied by a fever it is advisable to seek medical evaluation.
Neck pain may be associated with referred pain from the chest. Patients with angina or a myocardial infarction may complain of neck pain or neck stiffness.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


