Respiratory Support and Therapies
Objectives
• Define the key terms and key abbreviations in this chapter.
• Explain how to assist in the care of persons with artificial airways.
• Describe the principles and safety measures for suctioning.
• Explain how to assist in the care of persons on mechanical ventilation.
• Explain how to assist in the care of persons with chest tubes.
• Explain how to promote PRIDE in the person, the family, and yourself.
Key Terms
Some persons have serious problems affecting the respiratory system. They need complex procedures and equipment. The nurse may ask you to assist in their care.
See Body Structure and Function Review: The Respiratory System (Chapter 39).
See Promoting Safety and Comfort: Respiratory Support and Therapies.
Artificial Airways
Artificial airways keep the airway patent (open and unblocked). They are needed:
• When disease, injury, secretions, or aspiration obstructs the airway.
• For mechanical ventilation (p. 662)
• By some persons who are semi-conscious or unconscious
Intubation means inserting an artificial airway. Such airways are usually plastic and disposable. They come in various sizes.
• Oro-pharyngeal airway—inserted through the mouth and into the pharynx (Fig. 40-1, A). A nurse or respiratory therapist (RT) inserts the airway.
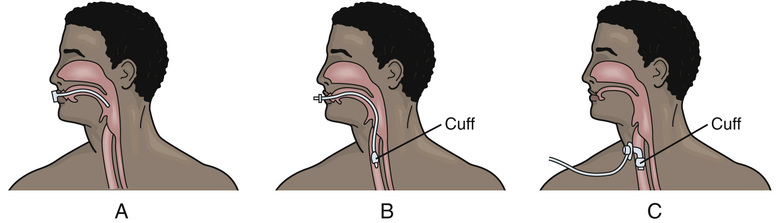
• Endotracheal (ET) tube—inserted through the mouth or nose into the trachea (Fig. 40-1, B). A doctor inserts it using a lighted scope. Some registered nurses (RNs) and RTs are trained to insert ET tubes.
• Tracheostomy tube—inserted through a surgically created opening (stomy) into the trachea (tracheo) (Fig. 40-1, C ). Cuffed tubes are common. Doctors perform tracheostomies.
Vital signs and pulse oximetry are measured often. Observe for hypoxia and other signs and symptoms of respiratory distress. If an airway comes out or is dislodged, tell the nurse at once. Frequent oral hygiene is needed. Follow the care plan.
Gagging and choking feelings are common. Imagine something in your mouth, nose, or throat. Comfort and reassure the person. Remind the person that the airway helps breathing. Use touch to show you care.
See Focus on Communication: Artificial Airways.
Tracheostomies
A tracheostomy is a surgically created opening (stomy) into the trachea (tracheo). Tracheostomies are often temporary. When no longer needed, the stoma is allowed to heal or is closed surgically.
Tracheostomies are permanent when the larynx is surgically removed. Cancer, airway injuries, long-term coma, spinal cord injuries, and diseases causing weakness or paralysis of the respiratory muscles may require a permanent tracheostomy.
A tracheostomy tube has 3 parts (Fig. 40-2).
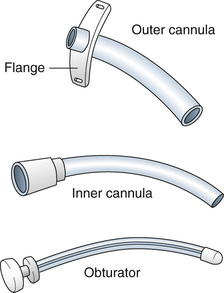
The cuffed tracheostomy tube provides a seal between the cannula and the trachea (see Fig. 40-1, C ). This prevents air from leaking around the tube and aspiration. A nurse or RT inflates and deflates the cuff.
The tube must not come out (extubation). If not secure, it could come out with coughing or if pulled on. A loose tube moves up and down, damaging the trachea. The tube must remain patent. If able, the person coughs up secretions. Otherwise suctioning is needed (p. 660). Call for the nurse at once if you note signs and symptoms of hypoxia or respiratory distress.
Safety Measures.
Nothing must enter the stoma. Otherwise the person can aspirate. These safety measures are needed.
• Dressings do not have loose gauze or lint.
• The person is assisted with shampooing. Water must not enter the stoma.
• The stoma is covered when shaving.
• Swimming is not allowed. Water will enter the tube or stoma.
• Medical-alert jewelry is worn. The person carries a medical-alert ID (identification) card.
Assisting With Tracheostomy Care.
The nurse may ask you to assist with tracheostomy care (trach care). Trach care is done daily or every 8 to 12 hours to prevent infection, promote healing, and promote comfort. It also is done as needed for excess secretions, soiled ties or collar, or soiled or moist dressings. The nurse tells you what supplies are needed. Assist as directed.
Trach care involves:
• Cleaning the stoma to prevent infection and skin breakdown.
• Applying clean ties or a Velcro collar. Clean ties are applied before removing the used ones. Hold the outer cannula in place until the nurse secures the new ties or collar. The ties or collar must be secure but not tight. For an adult, a finger should slide under the ties or collar (Fig. 40-3, A).

See Focus on Children and Older Persons: Assisting With Tracheostomy Care.
Suctioning
Secretions can collect in the airway. Retained secretions:
• Obstruct air flow into and out of the airway.
• Provide an environment for microbes.
• Interfere with oxygen (O2) and carbon dioxide (CO2) exchange.
Hypoxia can occur. Usually coughing removes secretions. Some persons cannot cough or the cough is too weak to remove secretions. They need suctioning.
Suction is the process of withdrawing or sucking up fluid (secretions). A tube connects to a suction source—wall outlet or suction machine—at 1 end and to a suction catheter at the other end. The catheter is inserted into the airway. Secretions are suctioned through the catheter.
The upper airway (nose, mouth, and pharynx) and lower airway (trachea and bronchi) are suctioned. These routes are used to suction the airway.
• Oro-pharyngeal. A suction catheter is passed through the mouth (oro) into the pharynx (pharyngeal). The Yankauer suction catheter is used to suction the mouth and for thick secretions (Fig. 40-4).