Prenatal Diagnostic Tests
Learning Objectives
After studying this chapter, you should be able to:
• Identify indications for fetal diagnostic procedures.
• Provide information in response to common questions parents have about procedures.

http://evolve.elsevier.com/McKinney/mat-ch/
Methods to detect physical abnormalities in the fetus and to monitor the fetal condition in a high-risk pregnancy with greater accuracy are becoming common as knowledge about their usefulness accumulates. Many pregnant women now expect to know the sex of their baby before birth because of routine use of technology such as ultrasound.
The ability to predict fetal outcome offers reassurance for most parents but not all. If the fetus is free of anomalies and is determined to be in good condition, the parents are relieved. However, testing may raise questions about fetal health rather than answer them, forcing parents to make decisions about having other tests or perhaps increasing their anxiety throughout the remainder of pregnancy. Decisions can create emotional conflict and raise ethical dilemmas that impose a great deal of stress on the family.
Indications for Prenatal Diagnostic Tests
In general, three reasons exist for performing fetal diagnostic and surveillance procedures: to detect congenital anomalies, to evaluate the condition of the fetus if the pregnancy is high risk and allow appropriate intervention, and to provide baseline information such as a more accurate gestational age. Procedures that were once done only if the pregnancy was high risk are now routine. Tests such as ultrasound or maternal serum screening are often offered to all pregnant women. Box 15-1 lists some risk factors for which prenatal diagnostic procedures are often recommended.
Ultrasound
When high-frequency sound waves are aimed in a specific direction, they are deflected by objects in their path and return as echoes. The amount of energy returned as an echo depends on the density of the object that deflected the ultrasonic wave. In obstetrics, when ultrasonic waves are directed through the abdomen of a pregnant woman, they are deflected by deep tissues of the mother and fetus. The returning sound waves are converted to two- or three-dimensional images that show structures of different densities.
Ultrasound procedures in obstetrics use real-time scanning in which a rapid sequence of fixed images is displayed on the screen, showing movement in body tissues as it happens. This technique allows the observer to detect movement such as fetal heartbeat, fetal breathing activity, and fetal body movement. Still images are captured for purposes such as gestational age calculation using multiple measures (Figure 15-1). Both video images may be captured for medical records as well as memories for the parents. Three-dimensional images may be captured for greater detail of the fetal body (Figure 15-2).


Emotional Responses
Some expectant mothers are excited and pleased and report feelings of love and protectiveness when they view the fetus. Others report increased feelings of vulnerability and anxiety about the fetus, fearing that something wrong will be found, and are thrilled if results are reassuring.
Expectant fathers are often fascinated by fetal movement and insist that the fetus “waved” at them or that they could see the facial expression as the fetus looked directly at them. Some couples wish to know the sex of the fetus, but others prefer to wait and “be surprised” even if the sex is obvious to the technician. Also, determining the fetal sex by ultrasound is sometimes not possible. Occasionally a couple is surprised at birth if the infant’s sex is not what they expected.
Although ultrasound is not yet a standard of care for all women, it is widely used because a great deal of information can be obtained with minimum risk to mother or fetus. Ultrasound may be used during any trimester, but the procedure and the reasons for its use vary for each trimester.
First Trimester
Transvaginal ultrasound is often used during the first trimester because the uterus, gestational sac, embryo, ovaries, and fallopian tubes are deep in the pelvis.
Procedure
The woman is placed in a lithotomy position for transvaginal ultrasound. A transvaginal probe that is encased in a disposable cover and coated with a gel that provides lubrication and promotes sound-wave conduction is inserted into the vagina. The woman may feel more comfortable if she inserts the probe herself.
Purposes
Transvaginal ultrasound is most common during the first trimester for:
• Determining the presence and location (intrauterine or elsewhere) of pregnancy
• Detecting multifetal gestations
• Identifying the need for follow-up testing
• Identifying ultrasound characteristics that suggest fetal abnormality, such as chromosome defects
• As an adjunct for transcervical or transabdominal chorionic villus sampling
During the first trimester, measurement of the crown-rump length of the embryo is the most reliable indicator of gestational age. Fetal viability is confirmed by observation of the fetal heartbeat, which is visible when the embryo is at least 5 mm in length. Maternal structures and some abnormalities such as uterine fibroids, ovarian cysts, and a bicornuate uterus also can be seen (American College of Obstetricians and Gynecologists [ACOG], 2009d).
Second and Third Trimesters
Transabdominal ultrasound is common during the second and third trimesters because the uterus is out of the pelvis and accessible. Transvaginal ultrasound continues to be useful to evaluate the cervical and lower uterine areas.
Procedure
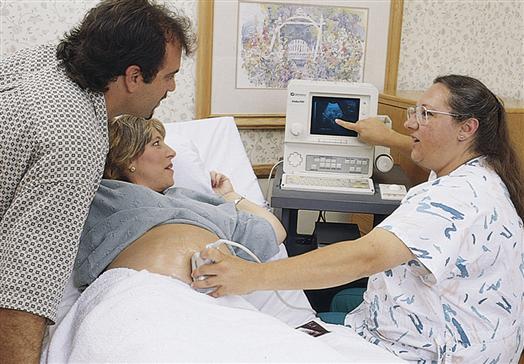
The mother is positioned on her back with her head and knees supported by pillows. Her head should be elevated, and she should be turned slightly to one side with a wedge or rolled blanket under one hip to avoid supine hypotension (see p. 237). If she desires, the screen can be positioned so that she can see the images. Transmission gel is spread over her abdomen, and the sonographer, usually a physician or ultrasound technician, moves a transducer over the abdomen to obtain a picture (Figure 15-3).
During the second trimester, a full bladder may be needed to displace the intestines and elevate the uterus for better visibility. If indicated, the woman should be instructed to drink several glasses of clear fluid an hour before the time of the examination and to delay urination until the examination is completed.
Purposes
Ultrasound is used during the second and third trimesters for many reasons, including to:
• Assess progress of fetal growth over a series of scans
• Compare growth of fetuses in multifetal gestations
• Evaluate amniotic fluid volume (see also “Biophysical Profile,” p. 311)
• Determine fetal presentation
• Guide needle placement for procedures such as amniocentesis or percutaneous umbilical blood sampling
Several body measurements are done to estimate gestational age during the last half of pregnancy, such as biparietal diameter, femur length, and abdominal circumference. Sequential assessments of multiple fetal measurements will help date the pregnancy more accurately than a single measurement. Estimating fetal age by ultrasound after 32 weeks is subject to major error. At this time the fetus may be evaluated for other signs of maturity and for signs of excessive or reduced growth rate (Manning, 2009).
Knowing the true gestational age is needed when screening for the level of maternal serum alpha-fetoprotein (MSAFP), which changes with fetal age. Accurate gestational age is also important if intrauterine growth restriction is suspected or the expected date of delivery is uncertain.
A comprehensive ultrasound in the second trimester is used to evaluate the fetus when risk factors are present or the basic examination shows abnormal findings. Examples include prior birth of an infant with anomalies or abnormal clinical findings such as hydramnios (excessive amniotic fluid), oligohydramnios (insufficient amniotic fluid), or abnormal levels of MSAFP. Fetal anatomy is systematically examined to identify major system and organ structures. Anomalies that can be detected with comprehensive ultrasound include most open neural tube defects such as myelomeningocele and anencephaly (nonclosure of spinal cord); abdominal wall defects such as gastroschisis and omphalocele; malformed kidneys; hydrocephalus; obstruction in fetal bowel and urinary systems; cleft lip and palate; and limb abnormalities. Maternal obesity may limit accuracy of ultrasound in pregnancy (Dashe, McIntire, & Twickler, 2009).
Advantages
Ultrasound allows clear visualization of the fetus and surrounding structures, and it is safe. Ultrasound is noninvasive and relatively comfortable, and the results are immediately available. Small portable scanners allow the machine to be moved easily for quick scans, such as in the case of a questionable fetal presentation in a laboring woman.
Disadvantages
Ultrasound and other prenatal diagnostic procedures cannot identify every fetal structural defect or defects that do not affect body structures, such as an inborn error of metabolism. In addition, women who do not have early prenatal care in the first trimester of pregnancy lose many benefits of early ultrasound examinations, such as best accuracy of gestational age. Cost may be a problem if the woman has no insurance coverage.
Ultrasound findings that are not normal but for which little is known about their implications may occur. The next step in the fetal diagnostic process may be unknown, causing greater parental anxiety.
Doppler Ultrasound Blood Flow Assessment
When an ultrasound wave is directed at an acute angle to a moving target, as with blood flowing through a vessel, the frequency of echoes changes as the cardiac cycle goes through systole and diastole. This change, referred to as the Doppler shift, indicates forward movement of blood within a vessel and resembles gentle hills and valleys that remain above the baseline.
Purpose
Pregnancies complicated by hypertension or fetal growth restriction caused by placental insufficiency may have Doppler ultrasound assessment of blood flow through the umbilical artery to identify abnormalities in the diastolic flow. The most common measurement is the systolic/diastolic (S/D) ratio, which normally decreases throughout gestation. If fetal peripheral resistance rises, the diastolic flow falls, resulting in an increased S/D ratio. In severe cases of growth restriction caused by placental insufficiency, diastolic flow may be absent or even reversed (American Academy of Pediatrics [AAP] & American College of Obstetricians and Gynecologists [ACOG], 2007; Harman, 2009).
Color Doppler
Color Doppler imaging is useful to clarify the relationships of body structures to each other. Nondirectional color Doppler imaging uses a single color to identify structures such as the number of vessels in the umbilical cord. Directional color Doppler uses two or more colors to determine the direction and speed of blood flow and pulsations within cardiovascular structures (Figure 15-4). It helps determine whether the heart has normal structure and whether major vessels have correct relationships to the heart chambers. Color Doppler imaging can determine blood flow and pulsations within umbilical cord vessels and other major vessels such as cranial vessels.

Alpha-Fetoprotein Screening
Alpha-fetoprotein (AFP) is the main protein in fetal plasma. It diffuses from fetal plasma into fetal urine and is excreted into the amniotic fluid. Some AFP crosses placental membranes into the maternal circulation. Therefore AFP can be measured both in maternal serum (i.e., MSAFP) and in amniotic fluid (i.e., amniotic fluid alpha-fetoprotein [AFAFP]). Abnormal concentrations of AFP are associated with serious fetal anomalies, requiring additional testing to determine the reason for the abnormal concentration.
The AFP concentration increases with advancing gestational age of the fetus. It is higher in multifetal gestations because more than one fetus is producing the protein. Interpretation of MSAFP values must be corrected for maternal weight because AFP diffuses into a larger maternal compartment in heavier women.
Purpose
Low levels of MSAFP are associated with chromosomal anomalies, such as trisomy 21 (Down syndrome). The most common cause of elevated AFP is failure of the embryonic neural tube or anterior body wall to close properly. In these conditions, neural or abdominal cavity tissues are exposed or covered with only a very thin layer of tissue, allowing high concentrations of AFP to seep into amniotic fluid and then enter maternal serum.
The most common open neural tube defects are anencephaly, in which the cranial vault is absent and most of the brain is undeveloped, and spina bifida, which has a wide range of severity (see Chapter 52). Box 15-2 lists other conditions that are associated with abnormal MSAFP.
Procedure
Pregnant women should be offered MSAFP screening, ideally between 16 and 18 weeks of gestation (AAP & ACOG, 2007). The mother is informed that MSAFP is a screening test rather than a diagnostic test. Further tests will be indicated to investigate abnormal concentrations. If MSAFP levels are abnormal, ultrasound is recommended initially to determine whether the abnormal concentration is caused by multifetal gestation, inaccurate gestational age, or fetal death.
Advantages
MSAFP evaluation has several advantages:
Limitations
Limitations of MSAFP evaluation are:
Multiple-Marker Screening
Two other markers, human chorionic gonadotropin (hCG) and unconjugated estriol, have been added to routine MSAFP evaluation to screen for chromosomal abnormalities with maternal serum. This multiple-marker screening increases the detection of trisomy 18 and trisomy 21 (Cunningham, Leveno, Bloom, et al., 2010; Jorde, Carey, & Bamshad, 2010). Maternal serum samples are taken between 16 and 18 weeks of gestation, and the results are considered positive if MSAFP and estriol are low and if hCG is high. If testing is positive, the woman should be offered additional testing, such as amniocentesis (withdrawal of amniotic fluid through the abdomen) for karyotyping or additional ultrasound to look for physical characteristics associated with the chromosome defects.
A fourth marker, the placental hormone inhibin A, improves the accuracy of multiple-marker screening for identifying trisomy 21 in women younger than the age of 35 years. Added costs for more tests must be considered when considering their benefit to the woman.
Chorionic Villus Sampling
Chorionic villi are microscopic projections from the outer membrane (chorion) that develop and burrow into endometrial tissue as the placenta is formed. The villi are composed of rapidly dividing cells of fetal origin that reflect the chromosomal and genetic makeup of the fetus. Chorionic villus cells can be used for diagnosis of fetal chromosomal, metabolic, or DNA abnormalities between 10 and 13 weeks of gestation.
Purpose
Chorionic villus sampling (CVS) uses transcervical or transabdominal sampling to obtain villi to diagnose fetal chromosome or metabolic abnormalities. It cannot be used to diagnose anomalies for which amniotic fluid is essential, such as open neural tube or body wall defects, which require measuring AFP levels (AAP & ACOG, 2007; Cunningham et al., 2010; Wapner, Jenkins, & Kalek, 2009).
Indications
CVS is usually performed between 10 and 13 weeks of gestation to diagnose fetal chromosomal, metabolic, or DNA abnormalities.
Procedure
As with all diagnostic procedures, the woman should receive both counseling about the procedure itself and genetic counseling about the specific defect for which CVS is being performed. The benefits and limitations of the procedure should be carefully explained, and a signed informed consent is obtained.
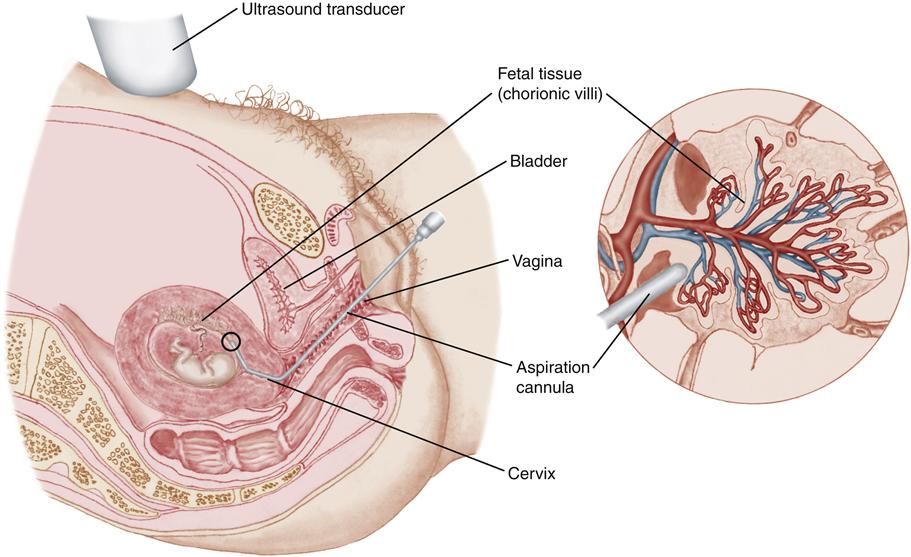
CVS can be performed by a transcervical or transabdominal approach (AAP & ACOG, 2007; Cunningham et al., 2010; Wapner et al., 2009). In the transcervical technique, a flexible catheter is inserted through the cervix and a sample of chorionic villi is aspirated (Figure 15-5). In the transabdominal technique, a needle is inserted through the abdominal and uterine walls to collect chorionic tissue.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


