Chapter 58 Abnormalities of the genital tract
Introduction
The true incidence of reproductive tract anomalies is uncertain and their role in reproductive difficulties is unclear (Saravelos et al 2008, Shulman 2008). While structural abnormalities of the uterus are particularly likely to cause problems, pregnancy and labour may also be affected by other conditions such as fibroids or uterine displacements. Female genital mutilation (also known as female circumcision) presents clear health risks for mother and baby. The midwife must be able to give appropriate and safe care for any woman presenting with a genital tract anomaly.
Developmental anomalies
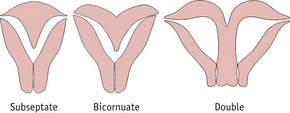
Most of the female genital tract arises from the müllerian ducts (see Ch. 29), which form during embryonic life and which fuse by the 12th week after fertilization. The median septum then breaks down, thus forming a single uterus (Laufer et al 2005). Should this process fail, abnormalities such as double uterus (with or without a double cervix and vagina), bicornuate uterus or subseptate uterus will occur (Fig. 58.1). As the müllerian ducts and wolffian ducts (see Ch. 29) develop close together, genital tract anomalies may be accompanied by malformations of the kidney and ureters. Care should include assessment of the urinary system (Laufer et al 2005).
Diethylstilbestrol (DES)
This synthetic non-steroidal oestrogen was used for approximately 30 years to treat conditions such as recurrent pregnancy loss and threatened abortion. It is still sometimes used as a form of postcoital contraception (Mackay Hart & Norman 2008). Girls who have been exposed to DES in utero have an unusually high incidence of uncommon anomalies. These include an increased incidence of:
Reproductive function is impaired. Conception may be difficult; ectopic pregnancy and preterm birth are commoner (RCOG 2002).
Unicornuate uterus
This uncommon abnormality arises from failure of development of one of the müllerian ducts. There is a higher rate of spontaneous abortion, breech presentation, fetal growth restriction and preterm labour, possibly due to the limited space in the uterine cavity (Akar et al 2005). Caesarean delivery is therefore more likely. If the pregnancy develops in a rudimentary horn, the outcome is usually spontaneous abortion or occasionally rupture of the rudimentary horn, as the myometrium becomes rapidly stretched.
Double uterus (uterus didelphys)
This may be accompanied by a double vagina or a longitudinal vaginal septum. As the pregnancy progresses, the midwife will notice that the fundus is abnormal in shape and may feel unusually wide. Breech presentation is common. As the pregnancy continues, the non-pregnant uterus will enlarge under the influence of the pregnancy hormones and may occupy space in the pelvis, thus obstructing labour. Twin pregnancy (one fetus in each horn) has been recorded (Ahmad et al 2000).
Vaginal septum
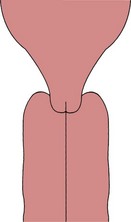
A vaginal septum (Fig. 58.2) may be longitudinal or transverse, complete or partial. It may be detected on vaginal examination, but, as the tissue is usually soft and is easily deflected by the examining fingers, the diagnosis is often overlooked. A vaginal septum may obstruct fetal descent during labour (Heinonen 2000).
Displacements of the uterus
Retroversion of the gravid uterus
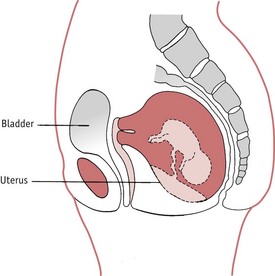
Retroversion of the uterus, where the pregnant uterus falls back into the hollow of the sacrum (Fig. 58.3), is normally of little clinical significance (Mackay Hart & Norman 2008). During pregnancy, the condition usually resolves spontaneously as the uterus grows and rises into the abdomen around the 12th week (Mukhopadhyay & Arulkumaran 2004).
Diagnosis
The woman will experience severe abdominal pain. On abdominal examination there is a soft swelling (the bladder) above the pubes, which may extend to the umbilicus and may be mistaken for the uterus. The fundus is not palpable at the brim of the pelvis. A pelvic ultrasound scan will assist the diagnosis (Mukhopadhyay & Arulkumaran 2004).
Treatment
The bladder is emptied with an indwelling catheter and is then kept empty until bladder tone returns. Once the bladder is empty, the uterus usually corrects its malposition spontaneously. This may be assisted if the mother lies in the semi-prone or Sims position (see Ch. 61). The retroversion will not recur, since the uterus will, in a few days, be too big to fall back into the pelvis. Persistent retroversion has been reported but is rare (Hamoda et al 2002).



