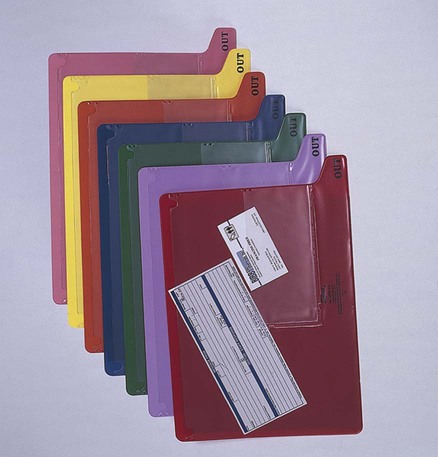
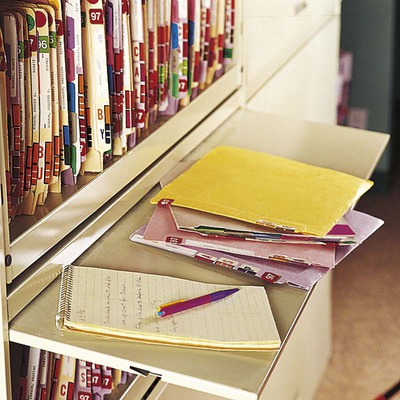
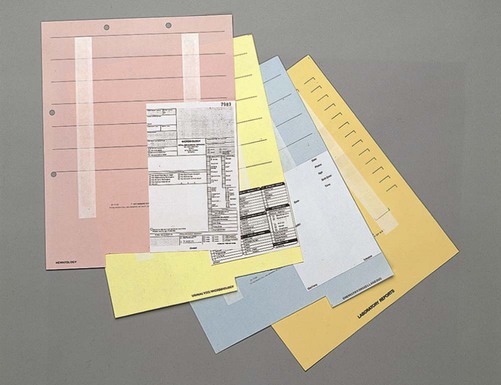
An electronic medical record offers a number of advantages: • Medical information is always legible. • Information is easy to retrieve. • Medical offices can be linked to laboratories, hospitals, and insurance companies. Access to laboratory data and test results is also easy and quick. • The EMR can be linked to medical information such as information about medications or treatment protocols for specific medical conditions. • Cost of computer hardware, software maintenance, and staff training • Orienting new or temporary staff to the EMR system • Difficulty in adding older records to an EMR system • Difficulty preventing unauthorized alterations and authenticating digital signatures • Structuring data so that they can be transferred among different digital systems • Incorporating updates to the software and medical codes as well as meeting new standards for electronic data transfer (see Chapter 46) Shelf units are available in two styles: open-shelf units or pull-down front units. As the name suggests, open-shelf units are open to the environment and cannot be closed. They must be in a room that can be locked separately from other parts of the office. The pull-down front units have lids that can be pulled over the front of the shelves and locked. This protects the records from environmental factors and allows each part of the file to be locked (Figure 41-1). It must always be possible to lock either the entire medical record room or individual shelving units. Folders are available with tabs. A tab is a projection of a folder that extends beyond the top or side edge of the folder. Folders for a file cabinet with drawers have tabs on the top, whereas folders for shelf units have tabs at the side of the file folder. In the medical office with shelf filing cabinets, a folder with a full-cut side tab is used. Indentations at intervals along the tab indicate the placement of adhesive labels. This ensures that all the labels on all the medical records are affixed at the same place on the file folders (Figure 41-2). Laboratory reports, copies of prescriptions, and telephone messages are often filed on mounting sheets with adhesive strips. Usually several items can be filed on the same sheet. The medical assistant files the first item at the bottom, with each succeeding item shingled up the mounting sheet. With this system the most recent item is always on top. Figure 41-3 shows this type of mounting sheet. Outguides, shown in Figure 41-4, are placed in the file to mark the place where a folder has been removed. Each guide has a pocket for a card indicating who removed the record and/or items that accumulate while the record is out of its storage area. Another type of outguide is made of heavy cardboard and has lines to write the name of the individual removing the record. It is important to follow rules when filing alphabetically. One resource for guidelines is ARMA International, an association for records and information management personnel. The medical assistant must always clarify the procedures followed by any given medical office (Procedure 41-1). Alphabetic File patient records correctly using an alphabetic filing system. 1. Procedural Step. Gather the records that are ready to be filed and remove any elastic bands or paper clips. 2. Procedural Step. Check the records to be sure that no loose sheets of paper are present. If loose sheets are found, insert them in the record. 3. Procedural Step. Sort the records alphabetically by last name, using the alphabetic sorter if available. 4. Procedural Step. Find the correct location in the file for the first record, pull the outguide halfway out, slide the record in front of the outguide in the correct location in the file, and finish removing the outguide. If your office does not use outguides, use your hand to make a space between the record before and the record after the one you are filing. 5. Procedural Step. If there is an index card in the outguide showing who had the record from the outguide, remove it. Place the outguide with other unused outguides. Some offices keep index cards for the physicians in separate boxes so that new cards do not need to be written; some offices cross out the name and reuse the index cards; some offices use slips of paper that are discarded after each use. 6. Procedural Step. File each record in the same way until all records have been filed.
Medical Record Management
LEARNING OBJECTIVES
PROCEDURES
1. Identify supplies and equipment needed to create and store paper medical records.
2. List principles of alphabetic and numeric filing.
3. Compare and contrast advantages and disadvantages of alphabetic and numeric filing systems for paper records.
4. Describe the process of filing reports and patient records.
File patient records: alphabetic.
5. Describe the implications of the paper medical record and the electronic medical record for medical record management.
File patient records: numeric.
6. Differentiate between storage of active and inactive records.
File reports.
7. Identify methods for retention and disposition of paper medical records.
Introduction to Medical Records
Electronic Medical Records
Equipment and Supplies
Storage Equipment
Shelf Filing Units
Filing Supplies
File Folders
Mounting Sheets
Other Supplies
Filing Systems
Alphabetic Filing
 Procedure 41-1 Filing Patient Records
Procedure 41-1 Filing Patient Records
Rule 1: Individual Names
Name
Unit 1
Unit 2
Unit 3
Mary Ann Stede
Stede
Mary
Ann
Alan Stone
Stone
Alan
Alan C. Stone
Stone
Alan
C.
Alan Charles Stone
Stone
Alan
Charles
Stoneham Medical Supply
Stoneham
Medical
Supply
Peter H. Stones
Stones
Peter
H. ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



Medical Record Management


 inch.
inch.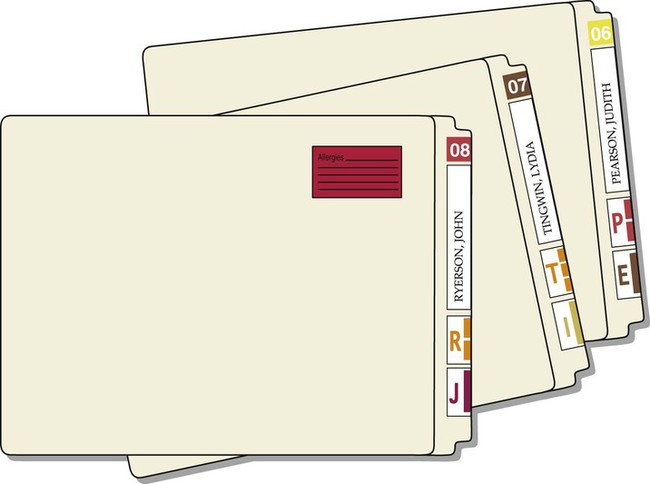


Get Clinical Tree app for offline access