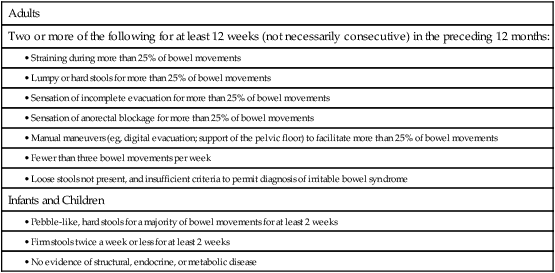
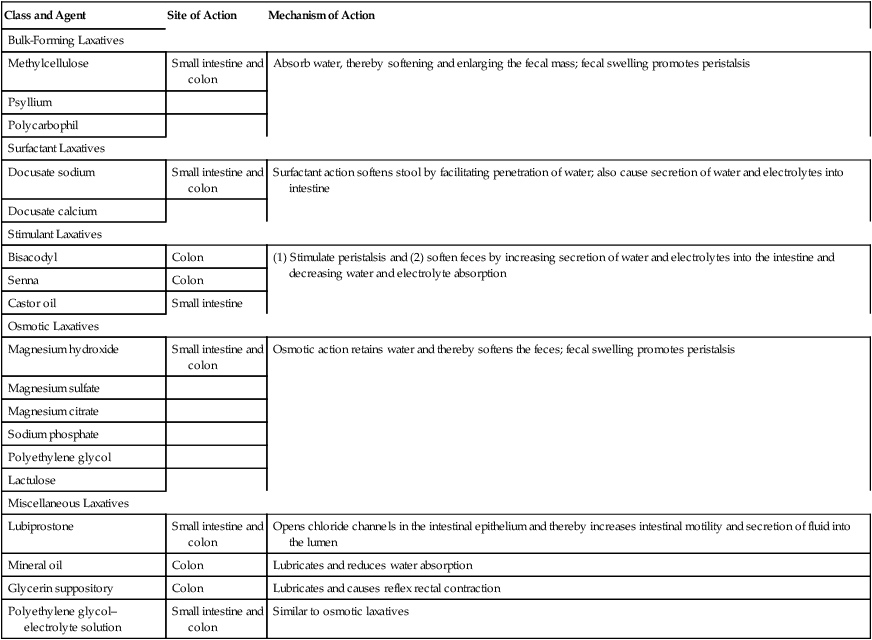
CHAPTER 79 Constipation is defined in terms of symptoms, which include hard stools, infrequent stools, excessive straining, prolonged effort, a sense of incomplete evacuation, and unsuccessful defecation. Scientists who do research on constipation usually define it using the Rome II criteria (Table 79–1). As Table 79–1 shows, constipation is determined more by stool consistency (degree of hardness) than by how often bowel movements occur. Hence, if the interval between bowel movements becomes prolonged, but the stool remains soft and hydrated, a diagnosis of constipation would be improper. Conversely, if bowel movements occur with regularity, but the feces are hard and dry, constipation can be diagnosed—despite the regular and frequent passage of stool. TABLE 79–1 Rome II Criteria for Constipation Traditionally, laxatives have been classified according to general mechanism of action. This scheme has four major categories: (1) bulk-forming laxatives, (2) surfactant laxatives, (3) stimulant laxatives, and (4) osmotic laxatives. Representative drugs are listed in Table 79–2. TABLE 79–2 Classification of Laxatives by Pharmacologic Category From a clinical perspective, it can be useful to classify laxatives according to therapeutic effect (time of onset and impact on stool consistency). When these properties are considered, most laxatives fall into one of three groups, labeled I, II, and III in this chapter. Group I agents act rapidly (within 2 to 6 hours) and give a watery consistency to the stool. Laxatives in group I are especially useful when preparing the bowel for diagnostic procedures or surgery. Group II agents have an intermediate latency (6 to 12 hours) and produce a stool that is semifluid. Group II agents are the ones most frequently abused by the general public. Group III laxatives act slowly (in 1 to 3 days) to produce a soft but formed stool. Uses for this group include treating chronic constipation and preventing straining at stool. Representative members of groups I, II, and III are listed in Table 79–3. TABLE 79–3 Classification of Laxatives by Therapeutic Response
Laxatives
General considerations
Constipation

Adults
Two or more of the following for at least 12 weeks (not necessarily consecutive) in the preceding 12 months:
Infants and Children
Laxative classification schemes

Class and Agent
Site of Action
Mechanism of Action
Bulk-Forming Laxatives
Methylcellulose
Small intestine and colon
Absorb water, thereby softening and enlarging the fecal mass; fecal swelling promotes peristalsis
Psyllium
Polycarbophil
Surfactant Laxatives
Docusate sodium
Small intestine and colon
Surfactant action softens stool by facilitating penetration of water; also cause secretion of water and electrolytes into intestine
Docusate calcium
Stimulant Laxatives
Bisacodyl
Colon
(1) Stimulate peristalsis and (2) soften feces by increasing secretion of water and electrolytes into the intestine and decreasing water and electrolyte absorption
Senna
Colon
Castor oil
Small intestine
Osmotic Laxatives
Magnesium hydroxide
Small intestine and colon
Osmotic action retains water and thereby softens the feces; fecal swelling promotes peristalsis
Magnesium sulfate
Magnesium citrate
Sodium phosphate
Polyethylene glycol
Lactulose
Miscellaneous Laxatives
Lubiprostone
Small intestine and colon
Opens chloride channels in the intestinal epithelium and thereby increases intestinal motility and secretion of fluid into the lumen
Mineral oil
Colon
Lubricates and reduces water absorption
Glycerin suppository
Colon
Lubricates and causes reflex rectal contraction
Polyethylene glycol–electrolyte solution
Small intestine and colon
Similar to osmotic laxatives

Group I: Produce Watery Stool in 2–6 Hr
Group II: Produce Semifluid Stool in 6–12 Hr
Group III: Produce Soft Stool in 1–3 Days
Osmotic Laxatives (in High Doses)
Magnesium salts
Sodium salts
Polyethylene glycol
Others
Castor oil
Polyethylene glycol–electrolyte solution
Osmotic Laxatives (in Low Doses)
Magnesium salts
Sodium salts
Polyethylene glycol
Stimulant Laxatives (Except Castor Oil)
Bisacodyl, oral*
Senna
Bulk-Forming Laxatives
Methylcellulose
Psyllium
Polycarbophil
Surfactant Laxatives
Docusate sodium
Docusate calcium
Others
Lactulose
Lubiprostone
Laxatives



Get Clinical Tree app for offline access
