1. Define the vocabulary terms listed 2. Differentiate diaper dermatitis from candidiasis 3. Summarize the nursing care for an infant who has atopic dermatitis, and give the rationale for each nursing measure 4. Discuss care of the child with impetigo 5. Identify complications associated with Staphylococcus 6. Discuss care of the child with cellulitis 7. Define two sources of pediculosis transmission 8. Identify two methods of evaluating burn injury 9. Discuss wound management precautions associated with burn injury White patches that resemble milk curds are visible on the tongue, inner lips, gums, and oral mucosa. Initially, these are painless but do not wipe away. The patches may bleed if attempts are made to scrape them away. Because of the discomfort, anorexia may be present. The systemic symptoms are mild if the infection remains in the mouth; however, it can pass along the mucous membranes into the gastrointestinal tract, causing inflammation of the esophagus and stomach. The infant may develop a beefy red, weeping diaper rash in the genitalia area (see Diaper Dermatitis). Development of symptoms indicates that the infant is oversensitive to certain substances called allergens, which enter the body via the digestive tract (food), inhalation (dust, pollen), direct contact (wool, soap, strong sunlight), or injections (insect bites, vaccines). Of children who have atopic dermatitis, 50% to 60% present with symptoms in the first year of life and 80% to 85% present by 5 years of age. Overall, 10% to 20% of children are affected by the disease (Cardona et al., 2006). Many children (80%) develop the triad of atopic dermatitis, asthma, and allergic rhinitis. The Child with Atopic Dermatitis (Eczema) • Use tepid water for bathing. • Air-dry skin and pat with a soft towel. • Apply topical corticosteroid before emollient. • Apply emollient within 3 minutes of bath. • Keep fingernails short and clean. • Use cotton “mitts” at night. • Use cotton sheets and pajamas. • Moisturize skin often until skin is soft and pliable. An effective moisturizer that is also inexpensive is Crisco shortening (Cardona et al., 2006). Parents need to be taught that it should not be used around the eyes or nasal passages. The nurse should establish a good working relationship with the parents. Families report high stress and feelings of helplessness in caring for children with atopic dermatitis. Parents express issues with the child’s sleeplessness due to itching and the child’s decreased self-esteem due to his or her physical appearance. The nurse should listen to ensure that parents understand the physician’s instructions and should clarify matters as needed (Nursing Care Plan 16-1). Nursing Care Plan 16-1 Deficient knowledge related to the nature of the disorder
Integumentary Disorders
 http://evolve.elsevier.com/Price/pediatric/
http://evolve.elsevier.com/Price/pediatric/
Integumentary System
Thrush (Oral Candidiasis)
Signs and Symptoms
Atopic Dermatitis (Infantile Eczema)
Nursing Care
 Home Care Considerations
Home Care Considerations
 Nursing Brief
Nursing Brief
 The Child with Atopic Dermatitis (Eczema)
The Child with Atopic Dermatitis (Eczema)
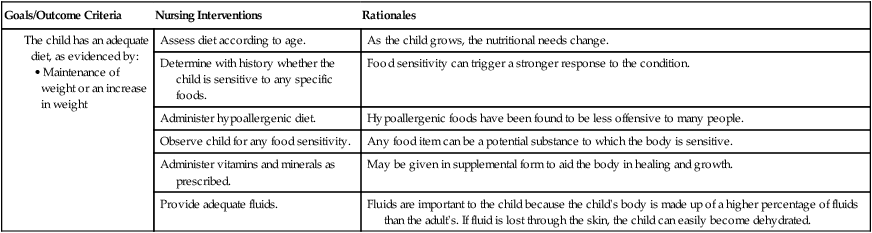
Goals/Outcome Criteria
Nursing Interventions
Rationales
Assess the knowledge of the parents.
Allows the nurse to teach the parents.
Instruct the parents in the care of the child’s skin
These are all areas that decrease the irritation to the skin or aid in healing of the skin.
• Remove clothing that might irritate the skin (e.g., wool).
Wool is an irritant to the skin.
• Provide loose cotton clothing.
Cotton absorbs if it is loose, does not constrict.
• Use a mild detergent to launder clothing.
Decreases the irritation of soap in the clothing.
• Thoroughly rinse clothing.
Ensures that most of the soap is removed from the clothing.
• Bathe the child in tepid water.
Tepid water decreases the amount of vasodilation, thus causing a decrease in stimulation to the skin and resulting in a decrease in itching.
Expose infant to sunlight but monitor closely.
Sunlight can be healing to the skin, but because of the skin’s condition, too much sunlight can cause more irritation.
Help parents identify products that contain wheat, milk, eggs, and peanuts.
These foods have been found to cause allergic reactions in children.
Advise parents to expect exacerbations and remissions.
Eczema can recur. If the parents know this, treatment can be sought earlier and the intensity of the condition can be lessened. ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



Integumentary Disorders
 Nursing Brief
Nursing Brief
 Nursing Brief
Nursing Brief
Get Clinical Tree app for offline access