Health Services Research
Translating Research into Policy
Patricia W. Stone, Arlene M. Smaldone, William M. Enlow and Robert J. Lucero
“Research is formalized curiosity. It is poking and prying with a purpose.”
—Zora Neale Hurston
The high cost of health care, large numbers of uninsured Americans, uncontrolled health care spending, and an unstable economy have led to the most recent efforts to reform health care in the United States. Most health policy experts agree that the nation must control health care costs, improve efficiency, increase access to health care, and improve the quality of care. However, it is often unclear how best to make these improvements. A strong evidence base is needed to inform decision-makers on what does and does not work to improve the health care system. Research that attempts to provide this evidence is often called “health services research” (HSR).
Defining Health Services Research
AcademyHealth, the preeminent professional society for health services researchers, defines HSR as “the multidisciplinary field of scientific investigation that studies how social factors, financing systems, organizational structures and processes, health technologies, and personal behaviors affect access to health care, the quality and cost of health care, and ultimately our health and well-being. Its research domains are individuals, families, organizations, institutions, communities, and populations” (AcademyHealth, 2008). The Agency for Healthcare Research and Quality (AHRQ), a primary funding organization for this type of research, states that, “Health services research examines how people get access to health care, how much care costs, and what happens to patients as a result of this care. Health services research aims to identify the most effective ways to organize, manage, finance, and deliver high-quality care; reduce medical errors; and improve patient safety” (Helping the nation with health services research, 2002).
A recent focus of HSR, based on the Comparative Effectiveness Research Act of 2008, is the conduct and synthesis of research comparing the benefits and harms of various interventions and strategies for preventing, diagnosing, treating, and monitoring health conditions in real-world settings (Conway & Clancy, 2009). The purpose of comparative effectiveness research (CER) is to improve health outcomes by developing and disseminating evidence-based information to patients, clinicians, and other decision-makers about interventions that are most effective for patients under specific circumstances (Iglehart, 2009; Volpp & Das, 2009). The Department of Health and Human Services (DHHS) as part of the American Recovery and Reinvestment Act of 2009, provided $400 million of financial support for CER. In June 2009, the Institute of Medicine recommended 100 national priorities for CER (Committee on Comparative Effectiveness Research Prioritization, 2009). Of the top 25 priorities, the following may be of particular interest to nurses: (1) “Compare the effectiveness of various primary care treatment strategies…and (2) Compare the effectiveness of literacy-sensitive disease management programs and usual care in reducing disparities in children and adults with low literacy and chronic disease.” The Patient Protection and Affordable Care Act authorizes CER and a number of demonstration projects that will depend on the use of HSR methods.
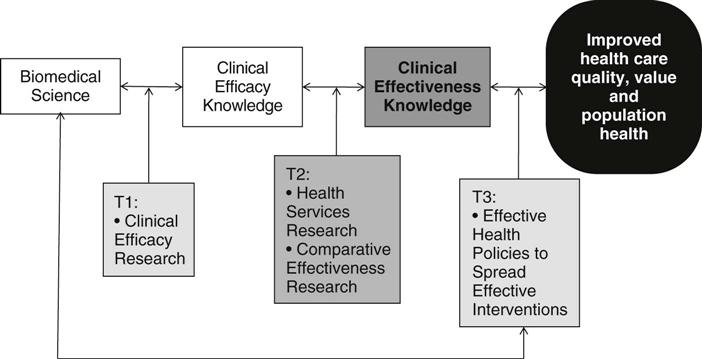
Dougherty and Conway (2008) developed a model intended to accelerate implementation of innovations in clinical settings to address the “how” of health care delivery (Figure 41-1). This transformational model suggests that basic science and its translation into clinical practice is only the first step to achieve effective, safe delivery of high-quality care (translation 1 or T1). Translation 2 (T2) processes focus on the translation of clinical efficacy knowledge into clinical effectiveness, and the policy changes needed to improve outcomes is addressed in T3 activities. Health services research and CER are the necessary population-based research activities at the T2 level and serve as the foundation for effective health policy.
HSR Methods
HSR researchers use both quantitative and qualitative research methods, and these methods are not unique to the field. However, it is the use of these methods to generate knowledge to inform health policy development and changes that is the hallmark of HSR. Edwardson (2007) reported on the theories and conceptual frameworks used by HSR nurse researchers in studies funded by AHRQ between 2000 and early 2005. A total of 28 different frameworks were identified in the 49 studies reviewed. The frameworks most often used were Donabedian’s quality paradigm (Donabedian, 1966) (i.e., structure-process-outcome), Rogers Diffusion of Innovation Theory (Rogers, 2003), Reason’s Theory of Human Error (Reason, 1990), and Andersen and Aday’s Model of Healthcare Access (Aday & Andersen, 1974). The common theoretical underpinning among these frameworks is their conceptualization of variables at the system level rather than the individual level.
Quantitative Methods and Data Sets
Using quantitative multivariate methods, HSR researchers sometimes analyze data from administrative data sets, such as hospital discharge data, and national survey data to examine health care access and quality, regional differences in care delivery patterns, health behavior patterns, and health outcomes from a population perspective. Various types of data are available to HSR researchers through the federal agencies in the DHHS including the Centers for Disease Control and Prevention, and AHRQ. Additionally, population census and employment data are available through the U.S. Census Bureau and the Bureau of Labor Statistics. Table 41-1 provides examples of some of the available national and state data available to HSR researchers through free public websites or by paying a fee to have access to data in a useable format for research.
TABLE 41-1
Examples of Publicly Available Data for Use in Health Services Research
| Agency | Data | Access | Fees |
| U.S. Department of Health and Human Services | Hospital Consumer Assessment of Healthcare Providers and Systems | Hospital Compare: www.hospitalcompare.hhs.gov | Free |
| Area Resource File | Health Resources and Services Administration: www.arfsys.com | $500.00 | |
| Centers for Disease Control and Prevention | Behavioral Risk Factor Surveillance System | Behavioral Risk Factor Surveillance System: www.cdc.gov/brfss | Free |
| National Health and Nutrition Examination Survey | National Center for Health Statistics: www.cdc.gov/nchs/nhanes.htm | Free | |
| National Immunization Survey | National Center for Health Statistics: www.cdc.gov/nis | Free | |
| National Survey of Ambulatory Surgery | National Center for Health Statistics: www.cdc.gov/nchs/nsas.htm | Free | |
| National Survey of Children with Special Health Care Needs | National Center for Health Statistics: www.cdc.gov/nchs/slaits/cshcn.htm | Free | |
| National Survey of Children’s Health | National Center for Health Statistics: www.cdc.gov/nchs/slaits/nsch.htm | Free | |
| Agency for Healthcare Research and Quality | Nationwide Inpatient Sample | Healthcare Cost and Utilization Project: www.hcup-us.ahrq.gov/nisoverview.jsp | Fees vary |
| Kids’ Inpatient Database | Healthcare Cost and Utilization Project: www.hcup-us.ahrq.gov/kidoverview.jsp | Fees vary | |
| State Inpatient Databases | Healthcare Cost and Utilization Project: www.hcup-us.ahrq.gov/sidoverview.jsp | Fees vary | |
| Nationwide Emergency Department Sample | Healthcare Cost and Utilization Project: www.hcup-us.ahrq.gov/nedsoverview.jsp | Fees vary | |
| State Ambulatory Surgery Database | Healthcare Cost and Utilization Project: www.hcup-us.ahrq.gov/sasdoverview.jsp | Fees vary | |
| American Hospital Association | Annual Survey Database | AHA Data: www.ahadata.com/ahadata_app/index.jsp | Fees vary |
| American Nurses Association | National Database of Nursing Quality Indicators | NDNQI: http://ndnqi@kumc.edu | Fees vary |
| Dartmouth | Healthcare Utilization Data of Medicare Patients | The Dartmouth Atlas of Health Care Project: http://dartmouthatlas.org/index.shtm | Free |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


