Health Promotion for the Developing Child
Learning Objectives
After studying this chapter, you should be able to:
• Define terms related to growth and development.
• Discuss principles of growth and development.
• Describe various factors that affect growth and development.
• Discuss theories of language development.
• Identify methods used to assess growth and development.
• Describe the classifications and social aspects of play.
• Explain how play enhances growth and development.
• Discuss recommendations for scheduled vaccines.
• Discuss the components of a nutritional assessment.
• Discuss the etiology and prevention of childhood injuries.

http://evolve.elsevier.com/McKinney/mat-ch/
Humans grow and change dramatically during childhood and adolescence. Normal growth and development proceed in an orderly, predictable pattern that establishes a basis for assessing an individual’s abilities and potential. Nurses provide health care teaching and anticipatory guidance about the growth and development of children in many settings, such as newborn nurseries, emergency departments, community clinics and health centers, and pediatric inpatient units.
Overview of Growth and Development
Nurses are frequently the members of the health care team whom parents approach. Parents are often concerned that their children are not progressing normally. Nurses can reassure parents about normal variations in development and can also identify problems early so that developmental delays can be addressed as soon as possible. Nurses who work with ill children must have a clear understanding of how children differ from adults and from each other at various stages. This awareness is essential to allow nurses to create developmentally appropriate plans of care to meet the needs of their young patients.
Definition of Terms
Although the terms growth and development often are used together and interchangeably, they have distinct definitions and meanings. Growth generally refers to an increase in the physical size of a whole or any of its parts or an increase in the number and size of cells. Growth can be measured easily and accurately. For example, any observer can see that an infant grows rapidly during the first year of life. This growth can be measured readily by determining changes in weight and length. The difference in size between a newborn and a 12-month-old infant is an obvious sign of the remarkable growth that occurs during the first year of life.
Development is a more complex and subtle concept. Development is generally considered to be a continuous, orderly series of conditions leading to activities, new motives for activities, and patterns of behavior.
Another definition of development is an increase in function and complexity that occurs through growth, maturation, and learning—in other words, an increase in capabilities. The process of language acquisition provides an example of development. The use of language becomes increasingly complex as the child matures. At 10 to 12 months of age, a child uses single words to communicate simple desires and needs. By age 4 to 5 years, complete and complex sentences are used to relate elaborate tales. Language development can be measured by determining vocabulary, articulation skill, and word use.
Maturity and learning also affect development. Maturation is the physical change in the complexity of body structures that enable a child to function at increasingly higher levels. Maturity is programmed genetically and may occur as a result of several changes. For example, maturation of the central nervous system depends on changes that occur throughout the body, such as an increase in the number of neurons, myelinization of nerve fibers, lengthening of muscles, and overall weight gain.
Learning involves changes in behavior that occur as a result of both maturation and experience with the environment. Predictable patterns are observed in learning, and these patterns are sequential, orderly, and progressive. For example, when learning to walk, babies first learn to control their heads, then to roll over, next to sit, then to crawl, and finally to walk. The child’s muscle mass and nervous system must grow and mature as well.
These examples show how complex and interrelated the processes of growth, development, maturation, and learning are. Children must be monitored carefully to ensure that these complicated events and activities unfold normally. Wide variations occur as children grow and develop. Each child has a unique rate and pattern of development, although parameters are used to identify abnormalities. Nurses must be familiar with normal parameters so that delays can be detected early. The earlier that delays are discovered and intervention initiated, the less dramatic their effect will be.
Stages of Growth and Development
To simplify analysis and discussion of the complex processes and theories related to growth and development, researchers and theorists have identified stages or age-groupings. These stages serve as reference points in describing various features of growth and development (Table 5-1). Chapters 6 through 9 discuss the physical growth and cognitive, emotional, language, and motor development specific to each stage.
TABLE 5-1
STAGES OF GROWTH AND DEVELOPMENT
The Following Stages and Age-Groupings Refer to Stages of Childhood Growth and Development
| STAGE | AGE |
| Newborn | Birth to 1 month |
| Infancy | 1 month to 1 year |
| Toddlerhood | 1 to 3 years |
| Preschool age | 3 to 6 years |
| School age | 6 to 11 or 12 years |
Parameters of Growth
Statistical data derived from research studies of large groups of children provide health care professionals with information about how children normally grow. Throughout infancy, childhood, and adolescence, growth occurs in bursts separated by periods when growth is stable or consistent.
Weight, length (or height), and head circumference are parameters that are used to monitor growth. They should be measured at regular intervals during infancy and childhood. The weight of the average term newborn infant is approximately 7½ pounds (3.4 kg). Male infants are usually slightly heavier than female infants. Usually, the birth weight doubles by 6 months of age and triples by 1 year of age. Between 2 and 3 years of age, the birth weight quadruples. Slow, steady weight gain during childhood is followed by a growth spurt during adolescence.
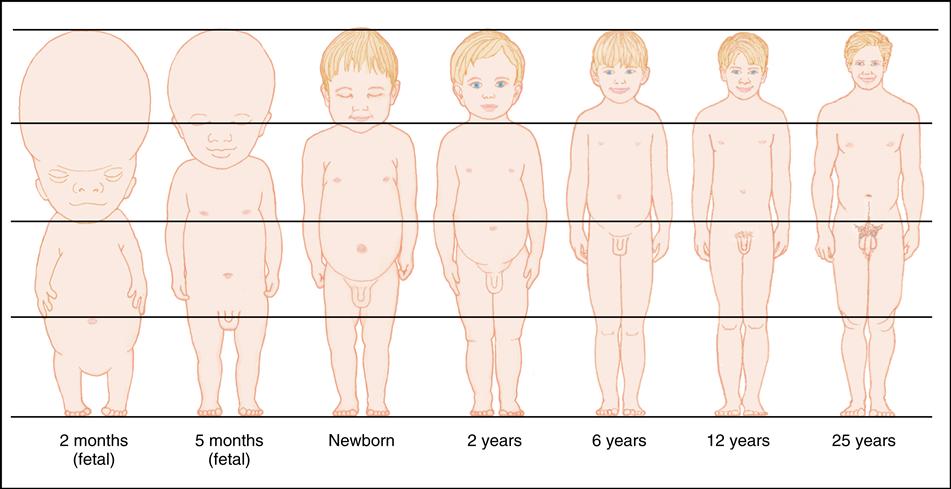
The average newborn infant is approximately 20 inches (50 cm) long, with an average increase of approximately 1 inch (2.5 cm) per month for the first 6 months, followed by an increase of approximately ½ inch (1.2 cm) per month for the remainder of the first year. The child gains 3 inches (7.6 cm) per year from age 1 through 7 years and then 2 inches (5 cm) per year from age 8 through 15 years. Boys generally add more height during adolescence than do girls. Body proportion changes are shown in Figure 5-1.
Head circumference indicates brain growth. The normal occipital-frontal circumference of the term newborn head is 13 to 15 inches (32 to 38 cm). Average head growth occurs according to the following pattern: 4.8 inches (12 cm) during the first year, 1 inch (2.54 cm) during the second year; ½ inch (1.27 cm) per year from 3 to 5 years, and ½ inch (1.2 cm) per year from 5 years until puberty. The average adult head circumference is approximately 21 inches (53 cm).
Dentition, the eruption of teeth, also follows a sequential pattern. Primary dentition usually begins to emerge at approximately 6 to 8 months. Most children have 20 teeth by age 2½ years. Permanent teeth, 32 in all, erupt beginning at approximately age 6 years, accompanied by the loss of primary teeth (see Chapter 33). Although some parents place importance on eruption of the teeth as a sign of maturation, dentition is not related to the level or rate of development.
Principles of Growth and Development
Patterns of Growth and Development
Growth and development are directional and follow predictable patterns (Boxes 5-1 and 5-2). The first direction of growth is cephalocaudal, or proceeding from head to tail (or toe). This means that structures and functions originating in the head develop before those in the lower parts of the body. At birth the head is large, a full one fourth of the entire body length, the trunk is long, and the arms are longer than the legs. As the child matures, the body proportions gradually change; by adulthood, the legs have increased in size from approximately 38% to 50% of the total body length (see Figure 5-1).
BOX 5-2
DIRECTIONAL PATTERNS OF GROWTH AND DEVELOPMENT
Cephalocaudal Pattern (Head to Toe)
Examples
Head initially grows fastest (fetus), then trunk (infant), then legs (child).
Infant can raise the head before sitting and can sit before standing.
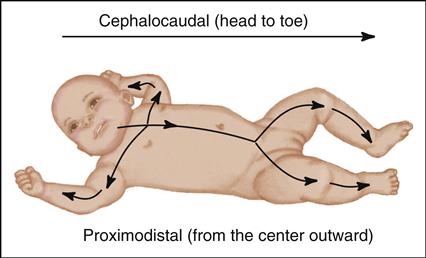
Proximodistal Pattern (from the Center Outward)
Examples
In the respiratory system, the trachea develops first in the embryo, followed by branching and growth outward of the bronchi, bronchioles, and alveoli in the fetus and infant.
Motor control of the arms comes before control of the hands, and hand control comes before finger control.
Directional growth and development are illustrated further by myelinization of the nerves, which begins in the brain and spreads downward as the child matures (see Box 5-1). Growth of the myelin sheath and other nerve structures contributes to cephalocaudal development, which is illustrated by an infant’s ability to raise the head before being able to sit and to sit before being able to stand.
A second directional aspect of growth and development is proximodistal, which means progression from the center outward, or from the midline to the periphery. The growth and branching pattern of the respiratory tract illustrates this concept. The trachea, which is the central structure of the respiratory tree, forms in the embryo by 24 days of gestation. Branching and growth outward occur in the bronchi, bronchioles, and alveoli throughout fetal life and infancy. Alveoli, which are the most distal structures of the system, continue to grow and develop in number and function until middle childhood.
Growth and development follow patterns, one of which is general to specific. As a child matures, activities become less generalized and more focused. For example, a neonate’s response to pain is usually a whole-body response, with flailing of the arms and legs even if the pain is in the abdomen. As the child matures, the pain response becomes more localized to the stimulus. An older child with abdominal pain guards the abdomen.
Another pattern is the progression of functions from simple to complex. This pattern is easily observed in language development. A toddler’s first sentences are formed simply, using only a noun and a verb. By age 5 years, the child constructs detailed stories using many complex modifiers.
The rate of growth is not constant as the child matures. Growth spurts, alternating with periods of slow or stagnant growth, are observed throughout childhood. Spurts are frequently seen as the child prepares to master a significant developmental task, such as walking. An increase in growth around a child’s first birthday may promote the neuromuscular maturation needed for taking the first steps.
All facets of development (cognitive, motor, social/emotional, language) normally proceed according to these patterns. Knowledge of these concepts is useful when determining how a child’s development is progressing and when comparing a child’s development with normal patterns.
Mastery of developmental tasks is not static or permanent, and developmental stages do not always correlate with chronologic age. Children progress through developmental stages at varying rates within normal limits and may master developmental tasks only to regress to earlier levels when ill or stressed. Also, people can struggle repeatedly with particular developmental tasks throughout life, although they have achieved more advanced levels of development.
Critical Periods
After birth, critical or sensitive periods exist for optimal growth and development. Similar to times during embryologic and fetal life, in which certain organs are formed and are particularly vulnerable to injury, critical periods are blocks of time during which children are ready to master specific developmental tasks. Children can master tasks outside these critical periods, but some tasks are learned more easily during particular periods.
Many factors affect a child’s sensitive learning periods, such as injury, illness, and malnutrition. For example, the sensitive period for learning to walk seems to be during the latter part of the first year and the beginning of the second year. Children seem to be driven by an irresistible urge to practice walking and display great pride as they succeed. If a child is immobilized, for example, for the treatment of an orthopedic condition from age 10 months to 18 months, the child may have difficulty learning to walk. The child can learn to walk, but the task may be more difficult than for other children.
Factors Influencing Growth and Development
Genetics
One factor that greatly influences a child’s growth and development is genetics. Genetic potential is affected by many factors. Environment influences how and to what extent particular genetic traits are manifested. See Chapter 10 for a discussion of genetics.
Environment
The environment, both physical and psychosocial, is a significant determinant of growth and developmental outcomes before and after birth. Prenatal exposures, which include maternal smoking, alcohol intake, chemical exposures, infectious diseases, and disease such as diabetes, can adversely affect the developing fetus. Socioeconomic status, mainly poverty, also has a significant effect on the developing child. Imported toys and other equipment for children can pose environmental hazards, particularly if they have multiple small pieces or components with high concentrations of lead or leaded paint.
Scientists suggest that factors in children’s physical environment increasingly influence their health status (American Academy of Pediatrics [AAP] Council on Environmental Health, 2011). Children are vulnerable to environmental exposures for the following reasons (AAP Council on Environmental Health, 2011; United States Environmental Protection Agency [EPA], 2008):
• More rapid respirations increase inhalation of air pollutants.
• Larger body surface area enhances absorption through the skin.
• Decreased ability to metabolically clear ingested toxins.
• Environmental toxins can be passed to an infant through breast milk.
Nurses can assist parents in preventing environmental injury by teaching them how to avoid the most common sources of environmental exposure. Anticipatory guidance about avoiding sun exposure, secondhand smoke or other air pollutants, lead in the home environment and in toys, mercury in foods, use of pesticides in gardens and playground equipment, pet insecticides (e.g., flea and tick collars), and radon will provide parents with the information they need to reduce risk. As with communicable disease, teaching about the importance of hand hygiene is paramount.
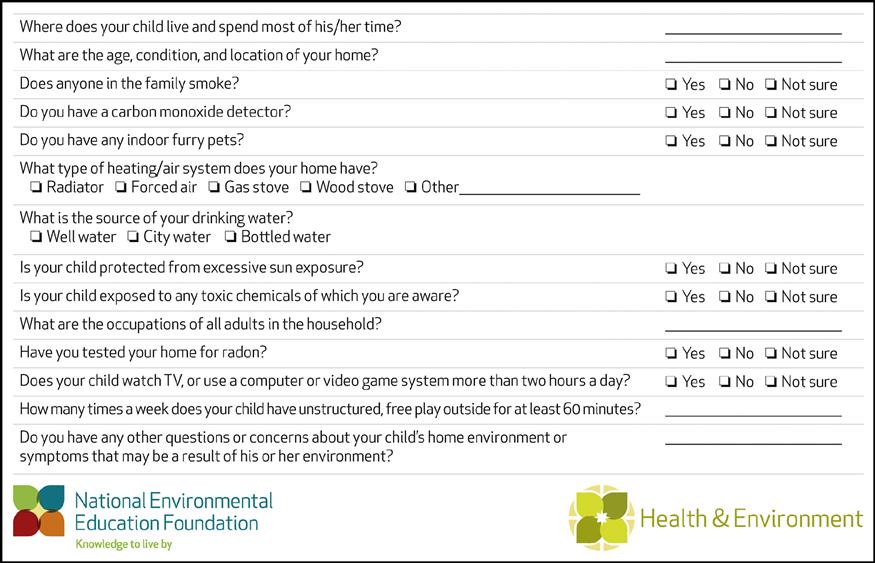
During well visits, nurses can perform a brief or expanded environmental health screening. Figure 5-2 provides an example of an environmental history. There are thousands of synthetic chemicals to which children are exposed, with very few having federal guidelines for exposure limits (Veal, Lowry, & Belmont, 2007). The AAP (2011) has expressed heightened concern that toxic chemicals in the environment are not being regulated to the extent needed to protect children and pregnant women, and this position has been supported by the American Nurses’ Association, the American Medical Association, and the American Public Health Association. The AAP (2011) recommends revisions to the Toxic Substances Control Act that would base decisions about toxic chemical exposures on a “reasonable concern” for harm, especially their potential for harm to children and pregnant women (p. 988). Among other recommendations, the AAP (2011) recommends increased funding for evidence-based research to examine the effects of chemical exposures on children.
Nurses can access, and can refer parents to, several online resources, including the Environmental Protection Agency (www.epa.gov/children), Pediatric Environmental Health Specialty Units (PEHU) (www.aoec.org), Tools for Schools program (www.epa.gov/schools), and Tox Town (www.toxtown.nlm.nih.gov), among others. Nurses can advise parents to be aware of toy and equipment recalls and to suggest that parents examine toys carefully before purchasing them.
Culture
Culture is the way of life of a people, including their habits, beliefs, language, and values. It is a significant factor influencing children as they grow toward adulthood.
When gathering data, nurses need to recognize how the common family structures and traditional values of various groups affect children’s performance on assessment tests. The child’s cultural and ethnic background must be considered when assessing growth and development. Standard growth curves and developmental tests do not necessarily reflect the normal growth and development of children of different cultural groups. Growth curves for children of various racial and cultural backgrounds are increasingly available. Nurse researchers and others conduct studies to determine the effectiveness of measurement tools for culturally diverse populations. In addition, culturally sensitive instruments are being developed to gather data to determine appropriate nursing interventions. To provide quality care to all children, nurses must consider the effect of culture on children and families (see Chapter 3).
Nutrition
Because children are growing constantly and need a continuous supply of nutrients, nutrition plays an important role throughout childhood. Children need more nutritious food in proportion to size than adults do. Children’s food patterns have changed over the years. Children are drinking more low fat or skim milk, however children older than 3 years of age consistently do not drink enough milk. Instead, they consume juices or other drinks that contain sugar (Peckenpaugh, 2010). Today’s children often eat meals outside the home, with 10% of young children having one or more meals in a daycare setting, away from parental supervision (Peckenpaugh, 2010). Nutrition is discussed in more depth later in this chapter.
Health Status
Overall health status plays an important part in the growth and development of children. At the cellular level, inherited or acquired disease can affect the delivery of nutrients, hormones, or oxygen to organs and also can affect organ growth and function. Disease states that affect growth and development include digestive or malabsorptive disorders, heart defects, and metabolic diseases.
Family
A child is an inseparable part of a family. Family relationships and influences substantially determine how children grow and progress. Because of the special bond and influence of the family on the child, there can be no separation of child from family in the health care setting. For example, to diminish anxiety in a child, nurses sometimes attempt to reduce parental anxiety, which may then reduce the stress on the child. Nursing care of children involves nursing care of the whole family and requires skill in dealing with both adults and children.
Family structures are in a constant state of change, and these dynamic states influence how children develop. Within the family, relationships change because of marriage, birth, divorce, death, and new roles and responsibilities. Societal forces outside the family, such as economics, population shifts, and migration, change how children are raised. These forces cause changes in family structures and the outcomes of child rearing, which must be considered when planning nursing care for children. The family is discussed in Chapter 3.
Parental Attitudes
Parental attitudes affect growth and development. Growth and development continue throughout life, and parents have stage-related needs and tasks that affect their children. Superimposed on these developmental issues are other factors influencing parental attitudes: educational level, childhood experiences, financial pressures, marital status, and available support systems. Parental attitudes are also affected by the child’s temperament, or the child’s unique way of relating to the world. Different temperaments affect parenting practices and have a bearing on whether a child’s unique personality traits develop into assets or problems.
Child-Rearing Philosophies
Child-rearing philosophies, shaped by myriad life events, influence how children grow and develop. For example, well-educated, well-read parents often provide their children with extra stimulation and opportunities for learning beginning at a young age. This enrichment includes extra parental attention and interaction—not necessarily expensive toys. Generally, development progresses best when children have access to enriched opportunities for learning.
Other parents may not recognize the value of providing a rich learning environment at home, may not have time, or may not appreciate this type of parenting. Children of these parents may not progress at the same rate as those raised in a more enriching atmosphere.
A significant point for parents to remember is that children must be ready to learn. If motor and neurologic structures are not mature, an overzealous approach for accomplishing a task related to those structures can be frustrating for both child and parent. For example, a child who is 6 months old will not be able to walk alone no matter how much time and effort the parent expends. However, at 12 to 14 months, a child usually is ready to begin walking and will do so with ease if given opportunities to practice.
Theories of Growth and Development
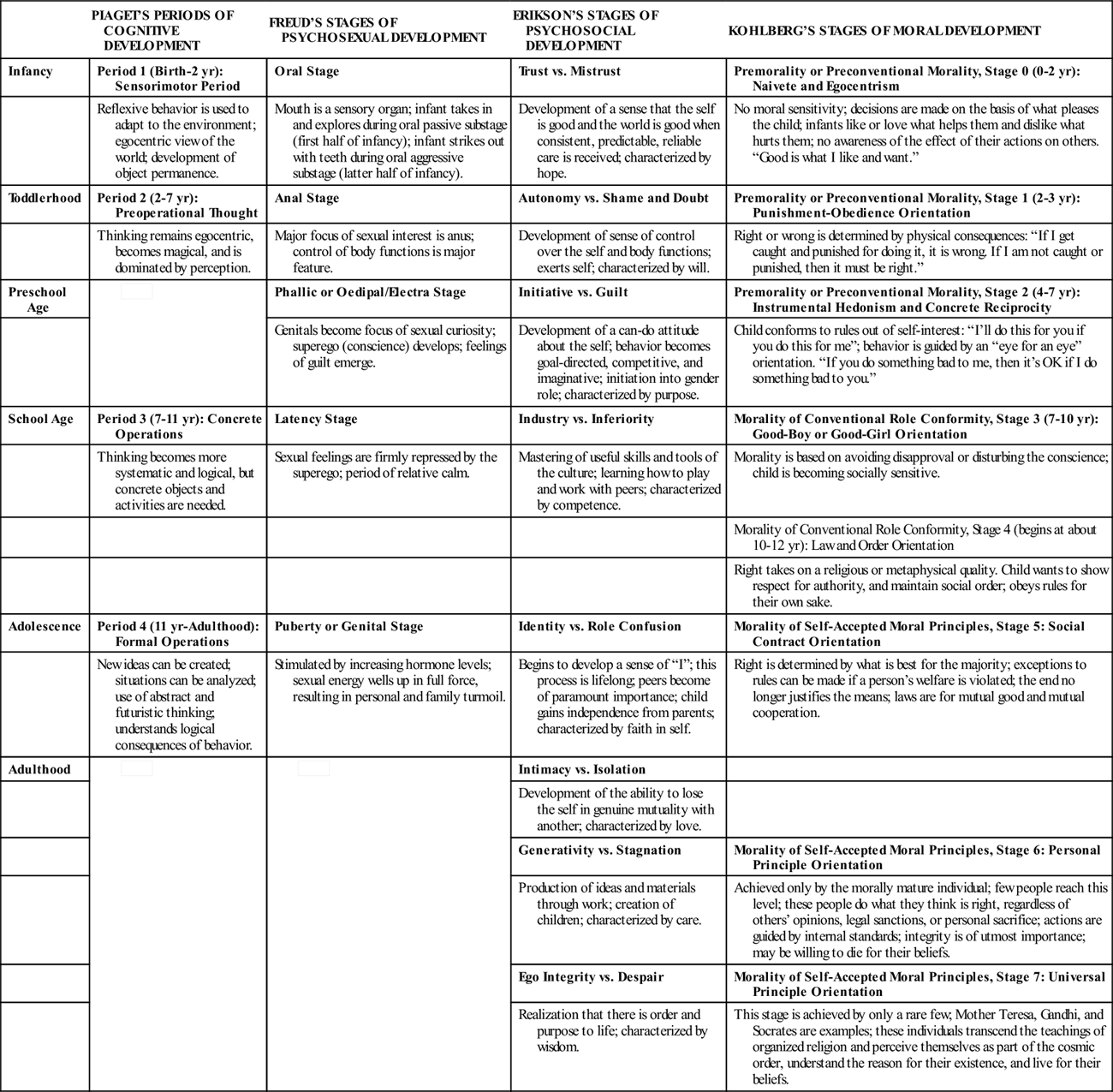
Many theorists have attempted to organize and classify the complex phenomena of growth and development. No single theory can adequately explain the wondrous journey from infancy to adulthood. However, each theorist contributes a piece of the puzzle. Theories are not facts but merely attempts to explain human behavior. Table 5-2 compares and contrasts theories discussed in the text. The chapters on each age-group provide further discussion of these theories.
TABLE 5-2
THEORIES OF GROWTH AND DEVELOPMENT
| PIAGET’S PERIODS OF COGNITIVE DEVELOPMENT | FREUD’S STAGES OF PSYCHOSEXUAL DEVELOPMENT | ERIKSON’S STAGES OF PSYCHOSOCIAL DEVELOPMENT | KOHLBERG’S STAGES OF MORAL DEVELOPMENT | |
| Infancy | Period 1 (Birth-2 yr): Sensorimotor Period | Oral Stage | Trust vs. Mistrust | Premorality or Preconventional Morality, Stage 0 (0-2 yr): Naivete and Egocentrism |
| Reflexive behavior is used to adapt to the environment; egocentric view of the world; development of object permanence. | Mouth is a sensory organ; infant takes in and explores during oral passive substage (first half of infancy); infant strikes out with teeth during oral aggressive substage (latter half of infancy). | Development of a sense that the self is good and the world is good when consistent, predictable, reliable care is received; characterized by hope. | No moral sensitivity; decisions are made on the basis of what pleases the child; infants like or love what helps them and dislike what hurts them; no awareness of the effect of their actions on others. “Good is what I like and want.” | |
| Toddlerhood | Period 2 (2-7 yr): Preoperational Thought | Anal Stage | Autonomy vs. Shame and Doubt | Premorality or Preconventional Morality, Stage 1 (2-3 yr): Punishment-Obedience Orientation |
| Thinking remains egocentric, becomes magical, and is dominated by perception. | Major focus of sexual interest is anus; control of body functions is major feature. | Development of sense of control over the self and body functions; exerts self; characterized by will. | Right or wrong is determined by physical consequences: “If I get caught and punished for doing it, it is wrong. If I am not caught or punished, then it must be right.” | |
| Preschool Age |  | Phallic or Oedipal/Electra Stage | Initiative vs. Guilt | Premorality or Preconventional Morality, Stage 2 (4-7 yr): Instrumental Hedonism and Concrete Reciprocity |
| Genitals become focus of sexual curiosity; superego (conscience) develops; feelings of guilt emerge. | Development of a can-do attitude about the self; behavior becomes goal-directed, competitive, and imaginative; initiation into gender role; characterized by purpose. | Child conforms to rules out of self-interest: “I’ll do this for you if you do this for me”; behavior is guided by an “eye for an eye” orientation. “If you do something bad to me, then it’s OK if I do something bad to you.” | ||
| School Age | Period 3 (7-11 yr): Concrete Operations | Latency Stage | Industry vs. Inferiority | Morality of Conventional Role Conformity, Stage 3 (7-10 yr): Good-Boy or Good-Girl Orientation |
| Thinking becomes more systematic and logical, but concrete objects and activities are needed. | Sexual feelings are firmly repressed by the superego; period of relative calm. | Mastering of useful skills and tools of the culture; learning how to play and work with peers; characterized by competence. | Morality is based on avoiding disapproval or disturbing the conscience; child is becoming socially sensitive. | |
| Morality of Conventional Role Conformity, Stage 4 (begins at about 10-12 yr): Law and Order Orientation | ||||
| Right takes on a religious or metaphysical quality. Child wants to show respect for authority, and maintain social order; obeys rules for their own sake. | ||||
| Adolescence | Period 4 (11 yr-Adulthood): Formal Operations | Puberty or Genital Stage | Identity vs. Role Confusion | Morality of Self-Accepted Moral Principles, Stage 5: Social Contract Orientation |
| New ideas can be created; situations can be analyzed; use of abstract and futuristic thinking; understands logical consequences of behavior. | Stimulated by increasing hormone levels; sexual energy wells up in full force, resulting in personal and family turmoil. | Begins to develop a sense of “I”; this process is lifelong; peers become of paramount importance; child gains independence from parents; characterized by faith in self. | Right is determined by what is best for the majority; exceptions to rules can be made if a person’s welfare is violated; the end no longer justifies the means; laws are for mutual good and mutual cooperation. | |
| Adulthood |  |  | Intimacy vs. Isolation | |
| Development of the ability to lose the self in genuine mutuality with another; characterized by love. | ||||
| Generativity vs. Stagnation | Morality of Self-Accepted Moral Principles, Stage 6: Personal Principle Orientation | |||
| Production of ideas and materials through work; creation of children; characterized by care. | Achieved only by the morally mature individual; few people reach this level; these people do what they think is right, regardless of others’ opinions, legal sanctions, or personal sacrifice; actions are guided by internal standards; integrity is of utmost importance; may be willing to die for their beliefs. | |||
| Ego Integrity vs. Despair | Morality of Self-Accepted Moral Principles, Stage 7: Universal Principle Orientation | |||
| Realization that there is order and purpose to life; characterized by wisdom. | This stage is achieved by only a rare few; Mother Teresa, Gandhi, and Socrates are examples; these individuals transcend the teachings of organized religion and perceive themselves as part of the cosmic order, understand the reason for their existence, and live for their beliefs. |
Piaget’s Theory of Cognitive Development
Jean Piaget (1896-1980), a Swiss theorist, made major contributions to the study of how children learn. His complex theory provides a framework for understanding how thinking during childhood progresses and differs from adult thinking. Like other developmental theorists, Piaget postulated that, as children develop intellectually, they pass through progressive stages (Piaget, 1962, 1967). The ages assigned to these periods are only averages. Piaget (1962, 1967) describes these stages as follows:
During the sensorimotor period of development, infant thinking seems to involve the entire body. Reflexive behavior is gradually replaced by more complex activities. The world becomes increasingly solid through the development of the concept of object permanence, which is the awareness that objects continue to exist even when they disappear from sight. By the end of this stage, the infant shows some evidence of reasoning.
During the period of preoperational thought, language becomes increasingly useful. Judgments are dominated by perception and are illogical, and thinking is characterized, especially during the early part of this stage, by egocentrism. In other words, children are unable to think about another person’s viewpoint and believe that everyone perceives situations as they do. Magical thinking (the belief that events occur because of wishing) and animism (the perception that all objects have life and feeling) characterize this period.
At the end of the preoperational stage, the child shifts from egocentric thinking and begins to be able to look at the world from another person’s view. This shifting enables the child to move into the period of concrete operations, where the child is no longer bound by perceptions and can distinguish fact from fantasy. The concept of time becomes increasingly clear during this stage, although far past and far future events remain obscure. Although reasoning powers increase rapidly during this stage, the child cannot deal with abstractions or with socialized thinking.
Normally, adolescents progress to the period of formal operations. In this period the adolescent proceeds from concrete to abstract and symbolic and from self-centered to other centered. Adolescents can develop hypotheses and then systematically deduce the best strategies for solving a particular problem because they use a formal operations cognitive style. Not all adolescents, however, reach this landmark at a consistent age, and at any given time, an adolescent may or may not exhibit characteristics of formal operations (Kuhn, 2008).
Nursing Implications of Piaget’s Theory
Although other developmental theorists have disputed Piaget’s theories, especially the ages at which cognitive changes occur, his work provides a basis for learning about and understanding cognitive development. Piaget’s theory is especially significant to nurses as they develop teaching plans of care for children. Piaget believed that learning should be geared to the child’s level of understanding and that the child should be an active participant in the learning process. For health teaching to be effective, nurses need to understand the different cognitive abilities of children at various ages. Nurses also need to know how to engage children in the learning process with developmentally appropriate activities. Because illness and hospitalization are often frightening to children, especially toddlers and preschoolers, nurses need to understand the cognitive basis of fears related to treatment and be able to intervene appropriately (see Chapter 35).
Understanding cognitive development that occurs at various ages and developmental levels also has implications for children’s health literacy (Borzekowski, 2009). With health-related messages so obvious in the media and so accessible on the Internet, it is important that children begin to think about health, evaluate health messages, and become involved in their own health promotion (Borzekowski, 2009).
Freud’s Theory of Psychosexual Development
Sigmund Freud (1856-1939) developed theories to explain psychosexual development. His theories were in vogue for many years and provided a basis for other theories. Freud postulated that early childhood experiences provide unconscious motivation for actions later in life (Freud, 1960). According to Freudian theory, certain parts of the body assume psychological significance as foci of sexual energy. These areas shift from one part of the body to another as the child moves through different stages of development. Freud’s work may help to explain normal behavior that parents may confuse with abnormal behavior, and it also may provide a good foundation for sex education.
Freud believed that during infancy sexual behavior seems to focus around the mouth, the most erogenous area of the infant body (oral stage). Infants derive pleasure from sucking and exploring objects by placing them in their mouths. During early childhood, when toilet training becomes a major developmental task, sensations seem to shift away from the mouth and toward the anus (anal stage). Psychoanalysts see this period as a time of holding on and letting go. A sense of control or autonomy develops as the child masters body functions.
During the preschool years, interest in the genitalia begins (phallic stage). Children are curious about anatomic differences, childbirth, and sexuality. Children at this age often ask many questions, freely exhibit their own sexual organs, and want to peek at those of others. Children often masturbate, sometimes causing parents great concern. Although it is not universal, a phenomenon described by Freud as the Oedipus complex in boys and the Electra complex in girls is seen in preschool children. This possessiveness of the child for the opposite-sex parent, marked by aggressiveness toward the same-sex parent, is considered normal behavior, as is a heightened interest in sex. To resolve these disturbing sexual feelings, the preschooler identifies with or becomes more like the same-sex parent. The superego (an inner voice that reprimands and evokes guilt) also develops. The superego is similar to a conscience (Freud, 1960).
Freud describes the school-age period as the latency stage, when sexuality plays a less prominent role in the everyday life of the child. Best friends and same-sex peer groups are influential in the school-age child’s life. Younger school-age children often refuse to play with children of the opposite sex, whereas prepubertal children begin to desire the companionship of opposite-sex friends.
During adolescence, interest in sex again flourishes as children search for identity (genital stage). Under the influence of fluctuating hormone levels, dramatic physical changes, and shifting social relationships, the adolescent develops a more adult view of sexuality. Cognitive skills, particularly in young adolescents, are not fully developed, however, and decisions are made often based on the adolescent’s emotional state, rather than on critical reasoning (Cromer, 2011). This can lead to questionable judgments about sexual matters and questions or confusion about sexual feelings and behaviors (A. Freud, 1974).
Nursing Implications of Freud’s Theory
Both children and parents may have questions and concerns about normal sexual development and sex education. Nurses need to understand normal sexual growth and development to help parents and children form healthy attitudes about sex and create an accepting climate in which adolescents may talk about sexual concerns.
Erikson’s Psychosocial Theory
Erik H. Erikson (1902-1994), inspired by the work of Sigmund Freud, proposed a popular theory about child development. He viewed development as a lifelong series of conflicts affected by social and cultural factors. Each conflict must be resolved for the child and adult to progress emotionally. How individuals address the conflicts varies widely. According to Erikson, however, unsuccessful resolution leaves the individual emotionally disabled (Erikson, 1963).
Each of eight stages of development has a specific central conflict or developmental task. These eight tasks are described in terms of a positive or negative resolution. The actual resolution of a specific conflict lies somewhere along a continuum between a perfect positive and a perfect negative.
According to Erikson (1963), the first developmental task is the establishment of trust. The basic quality of trust provides a foundation for the personality. If an infant’s physical and emotional needs are met in a timely manner through warm and nurturing interactions with a consistent caregiver, the infant begins to sense that the world is trustworthy. The infant begins to develop trust in others and a sense of being worthy of love. Through successful achievement of a sense of trust, the infant can move on to subsequent developmental stages.
According to Erikson, unsuccessful resolution of this first developmental task results in a sense of mistrust. If needs are consistently unmet, acute tension begins to appear in children. During infancy, signs of unmet needs include restlessness, fretfulness, whining, crying, clinging, physical tenseness, and physical dysfunctions such as vomiting, diarrhea, and sleep disturbances. All children exhibit these signs at times. If these behaviors become personality characteristics, however, unsuccessful resolution of this stage is suspected.
The toddler’s developmental task is to acquire a sense of autonomy rather than a sense of shame and doubt. A positive resolution of this task is accomplished by the ability to control the body and body functions, especially elimination. Success at this stage does not mean that the toddler, even as an adult, will exhibit autonomous behavior in all life situations. In certain circumstances, feelings of shame and self-doubt are normal and may be adaptive.
Erikson’s theory describes each developmental stage, with crises related to individual stages emerging at specific times and in a particular order. Likewise, each stage is built on the resolution of previous developmental tasks. During each conflict, however, the child spends some energy and time resolving earlier conflicts (Erikson, 1963).
Nursing Implications of Erikson’s Theory
In stressful situations, such as hospitalization, children, even those with healthy personalities, evoke defense mechanisms that protect them against undue anxiety. Regression, a behavior used frequently by children, is a reactivation of behavior more appropriate to an earlier stage of development. This defense mechanism is illustrated by a 6-year-old boy who reverts to sucking his thumb and wetting his pants under increased stress, such as illness or the birth of a sibling. Nurses can educate parents about regression and encourage them to offer their children support, not ridicule. They can provide constructive suggestions for stress management and reassure parents that regression normally subsides as anxiety decreases.
Erikson’s main contribution to the study of human development lies in his outline of a universal sequence of phases of psychosocial development. His work is especially relevant to nursing because it provides a theoretic basis for much of the emotional care that is given to children. The stages are further discussed in the chapters on each age-group.
Kohlberg’s Theory of Moral Development
Lawrence Kohlberg (1927-1987), a psychologist and philosopher, described a stage theory of moral development that closely parallels Piaget’s stages of cognitive development. He discussed moral development as a complicated process involving the acceptance of the values and rules of society in a way that shapes behavior. This cognitive-developmental theory postulates that, although knowing what behaviors are right and wrong is important, it is much less important than understanding and appreciating why the behaviors should or should not be exhibited (Kohlberg, 1964).
Guilt, an internal expression of self-criticism and a feeling of remorse, is an emotion closely tied to moral reasoning. Most children 12 years old or older react to misbehavior with guilt. Guilt helps them realize when their moral judgment fails.
Building on Piaget’s work, Kohlberg studied boys and girls from middle- and lower-class families in the United States and other countries. He interviewed them by presenting scenarios with moral dilemmas and asking them to make a judgment. His focus was not on the answer but on the reasoning behind the judgment (Kohlberg, 1964). He then classified the responses into a series of levels and stages.
During the Premorality (preconventional morality) level, which has three substages (see Table 5-2), the child demonstrates acceptable behavior because of fear of punishment from a superior force, such as a parent. At this stage of cognitive and moral development, children cannot reason as mature members of society. They view the world in a selfish, egocentric way, with no real understanding of right or wrong. They view morality as external to themselves, and their behavior reflects what others tell them to do, rather than an internal drive to do what is right. In other words, they have an external locus of control. A child who thinks “I will not steal money from my sister because my mother will spank me” illustrates premorality.
During the Morality of Conventional Role Conformity (conventional morality) level, which is primarily during the school-age years, the child conforms to rules to please others. The child still has an external locus of control, but a concern for social order begins to emerge and replace the more egocentric thinking of the earlier stage. The child has an increased awareness of others’ feelings. In the child’s view, good behavior is that which those in authority will approve. If behavior is not acceptable, the child feels guilty.
Two stages, stage 3 and stage 4, characterize this level (see Table 5-2). This level of moral reasoning develops as the child shifts the focus of living from the family to peer groups and society as a whole. As the child’s cognitive capacities increase, an internal sense of right and wrong emerges, and the individual is said to have developed an internal locus of control. Along with this internal locus of control comes the ability to consider circumstances when judging behavior.
Level 3, Morality of Self-Accepted Moral Principles (postconventional morality), begins in adolescence, when abstract thinking abilities develop. The person focuses on individual rights and principles of conscience during this stage. There is an internal locus of control. Concern about what is best for all is uppermost, and persons step back from their own viewpoint to consider what rights and values must be upheld for the good of all. Some individuals never reach this point. Within this level is stage 5, in which conformity occurs because individuals have basic rights and society needs to be improved. The adolescent in this stage gives as well as takes and does not expect to get something without paying for it. In stage 6, conformity is based on universal principles of justice and occurs to avoid self-condemnation (Colby, Kohlberg, & Kauffman, 1987; Kohlberg, 1964).
Only a few morally mature individuals achieve stage 6. These people, committed to a moral ideal, live and die for their principles.
Kohlberg believes that children proceed from one stage to the next in a sequence that does not vary, although some people may never reach the highest levels. Even though children are raised in different cultures and with different experiences, he believes that all children progress according to his description.
Nursing Implications of Kohlberg’s Theory
To provide anticipatory guidance to parents about expectations and discipline of their children, nurses must be aware of how moral development progresses. Parents are often distraught because their young children apparently do not understand right and wrong. For example, a 6-year-old girl who takes money from her mother’s purse does not show remorse or seem to recognize that stealing is wrong. In fact, she is more concerned about her punishment than about her misdeed. With an understanding of normal moral development, the nurse can reassure the concerned parents that the child is showing age-appropriate behavior.
Theories of Language Development
Human language has a number of characteristics that are not shared with other species of animals that communicate with each other. Human language has meaning, provides a mechanism for thought, and permits tremendous creativity.
Because language is such a complex process and involves such a vast number of neuromuscular structures, brain growth and differentiation must reach a certain level of maturity before a child can speak. Language development, which closely parallels cognitive development, is discussed by most cognitive theorists as they explain the maturation of thinking abilities. The process of how language develops remains a mystery, however.
Passive, or receptive, language is the ability to understand the spoken word. Expressive language is the ability to produce meaningful vocalizations. In most people, the areas in the brain responsible for expressive language are close to motor centers in the left cerebral area that control muscle movement of the mouth, tongue, and hands. Humans use a variety of facial and hand movements as well as words to convey ideas.
Crying is the infant’s first method of communication. These vocalizations quickly become distinct and individual and accurately convey such states as hunger, diaper discomfort, pain, loneliness, and boredom. Vowel sounds appear first, as early as 2 weeks of age, followed by consonants at approximately 5 months of age.
By age 2 years, children have a vocabulary of roughly 300 words and can construct simple sentences. By age 4 years, children have gained a sense of correct grammar and articulation, but several consonants, including “l” and “r,” remain difficult to pronounce. For example, the sentence “The red and blue bird flew up to the tree” might be pronounced by the preschooler as “The wed and boo bud fwew up to the twee!”
The language of school-age children is less concrete and much more articulate than that of the preschooler. School-age children learn and understand language construction, use more sophisticated terminology, use varied meanings for words, and can write and express ideas in paragraphs and essays (Feigelman, 2011).
Infants learn much of their language from their parents. Children who are raised in homes where verbalization is encouraged and modeled tend to display advanced language skills. Also, in infancy, receptive ability (the understanding of language) is more developed than expressive skill (the actual articulation of words). This tendency, which persists throughout life, is important to realize when caring for children. In clinical situations, nurses must communicate what is happening to their young patients by use of simple, age-appropriate words, although the child may not verbalize understanding.
Nurses and other health providers need to assess a young child’s language development at each well visit. Parent concern or positive family history of language problems, combined with clinical assessment of language development, can identify children who may be at risk for disorders associated with altered expressive or receptive language (Schum, 2007). Language development is discussed in more depth in chapters on each age-group and in Chapter 55.
Assessment of Growth
Because growth is an excellent indicator of physical well-being, accurate assessments must be made at regular intervals so that patterns of growth can be determined. Trained individuals using reliably calibrated equipment and proper techniques should perform growth measurement. Methods of obtaining accurate measurements in children are described in Chapter 33. To minimize the chance of error, data should be collected on children under consistent conditions on a routine basis, and values should be recorded and plotted on growth charts immediately.
Standardized growth charts allow an individual child’s growth (length/height, weight, head circumference, body mass index [BMI]) to be compared with statistical norms. The most commonly used growth charts for boys and girls ages 2 years to 20 years are those developed by the National Center for Health Statistics. The World Health Organization growth charts are recommended for use for infants and children up to 2 years of age (available at www.cdc.gov/growthcharts).
Because height and weight are the best indicators of growth, these parameters are measured, plotted on growth charts, and monitored over time at each well visit. Brain growth can also be monitored by measuring infant frontal-occipital circumference at intervals and plotting the values on growth charts. It is important to relate head size to weight because larger babies have bigger heads. These measurements are routinely performed during the first 2 years of life.
BMI, which is a function of both height and weight, is an important measure of growth and overall nutritional status in children older than age 2 years. Because childhood overweight and obesity can contribute to health problems later in life, the American Academy of Pediatrics (Barlow, 2007) recommends obesity prevention beginning at birth. Infants and children younger than 2 years old can be screened for overweight using the weight-to-length measurement; concern is generated when that percentile exceeds the 95th. BMI charts are included in the most recent versions of charts available from the Centers for Disease Control and Prevention.
Growth rate is measured in percentiles. The area between any two percentiles is referred to as a growth channel. Childhood growth normally progresses according to a pattern along a particular growth channel. Deviations from normal growth patterns may suggest problems. Any change of more than two growth channels indicates a need for more in-depth assessment.
Recognition of abnormal growth patterns is an important nursing function. The earlier that growth disorders are detected, diagnosed, and treated, the better the long-term prognosis.
Assessment of Development
Assessment of development is a more complex process than assessment of growth. To assess developmental progress accurately, nurses and health providers need to gather data from many sources, including observations and interviews, physical examinations, interactions with the child and parents, and various standardized assessment tools.
The AAP issued a policy statement in 2006 (reaffirmed in 2010), which calls for providers to do a combination of developmental surveillance and developmental screening throughout a child’s infancy and early childhood (AAP, 2006/2010). Developmental surveillance is performed at every well visit and includes eliciting and paying attention to parent concerns, keeping a documented developmental history, identifying protective and risk factors, and directly observing the child’s development (AAP, 2006/2010, p. 419). If surveillance raises a concern, the provider refers the child for more formalized screening. The AAP recommends that providers conduct a formal developmental screening with a sensitive and specific screening instrument when the child is 9 months, 18 months, and 24 to 30 months of age (AAP, 2006/2010). Using formalized screening in addition to routine surveillance can increase appropriate referrals for early intervention; however, recent mixed (quantitative and qualitative) research using a national sample of 17 pediatric practices found that the percentage of children screened at the appropriate ages is approximately 85% of children; however, the rate of referral for follow-up is far less (King, Tandon, Macias, et al., 2010).
Observation is a valuable method most often used to obtain information about a child’s developmental age (level of functioning). By watching a child during daily activities, such as eating, playing, toileting, and dressing, nurses gather a great deal of assessment data. Observation of the child’s problem-solving abilities, communication patterns, interaction skills, and emotional responses can yield valuable information about the child’s level of development. Similarly, interviews and physical examinations can provide much information about how the child functions.
In addition to these sources of data, many standardized assessment tools are available for nurses and other health care professionals to use for developmental assessment. Standardized developmental tools should be both sensitive (accurately identifies developmental problems) and specific (accurately identifies those who do not have developmental problems). Additionally, they should be relatively easy to administer or to have the parent complete in a reasonable amount of time. General assessment screening instruments that meet these criteria include the Ages and Stages Questionnaire, the Infant Development Inventory, and the Parents’ Evaluations of Developmental Status (PEDS), among others (AAP, 2006/2010). In general, screening tools are organized around major developmental areas (language, cognitive, social, behavioral, and motor). Many are given to parents to complete in the office setting or before the child’s appointment. Domain-specific instruments for identifying delays in language/cognitive areas or for screening for autism also are available (Wallis & Smith, 2008).
Developmental assessment should be part of a newborn infant’s assessment and of every well-child examination for several reasons. One reason is that parents want to know how their child compares with others and whether development is normal, especially if they had a difficult pregnancy or have other children who are developmentally delayed. Developmental assessment tends to allay fears. Probably the most important reason for assessment is that abnormal development must be discovered early to facilitate optimal outcomes through early intervention.
Denver Developmental Screening Test II (DDST-II)
One, more in-depth, screening tool used for infants and young children is the Denver Developmental Screening Test II (DDST-II). The DDST-II provides a clinical impression of a child’s overall development and alerts the user to potential developmental difficulties. It requires training to learn how to administer it properly.
The DDST-II, designed to be used with children between birth and 6 years of age, assesses development on the basis of performance of a series of age-appropriate tasks. There are 125 tasks or items arranged in four functional areas (Frankenburg & Dodds, 1992):
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


