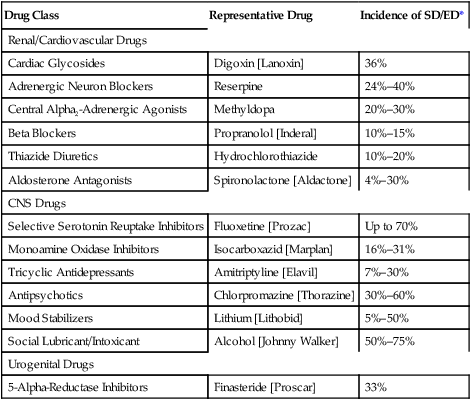
CHAPTER 66 Erectile dysfunction (ED), also known as impotence, is defined as a persistent inability to achieve or sustain an erection suitable for satisfactory sexual performance. In the United States, ED affects up to 30 million men, and accounts for 525,000 physician visits each year. ED is commonly associated with chronic illnesses, especially diabetes, hypertension, and depression. The cause of ED may be the illness itself or the drugs used for treatment. Among men with diabetes, the incidence of ED is between 35% and 75%. Some of the drugs that can cause ED are listed in Table 66–1. TABLE 66–1 Some Drugs That Can Cause Sexual/Erectile Dysfunction *Values for sexual dysfunction/erectile dysfunction (SD/ED) incidence are estimates based on patient reports, not on carefully controlled trials. Before discussing drugs for ED, we need to review the physiology of erection. As indicated in Figure 66–1, the process begins with sexual arousal, which increases parasympathetic nerve traffic to the penis, causing local release of nitric oxide. Nitric oxide then activates guanylyl cyclase, an enzyme that makes cyclic guanosine monophosphate (cGMP). Through a series of steps, cGMP promotes relaxation of arterial and trabecular smooth muscle. The resultant arterial dilation increases local blood flow and blood pressure, which, in combination with relaxation of trabecular smooth muscle, causes expansion and engorgement of sinusoidal spaces in the corpus cavernosum. This, in turn, causes venous occlusion and thereby reduces venous outflow. The combination of increased arterial pressure and arterial inflow plus reduced venous outflow causes sufficient engorgement to produce erection. Erection subsides when cGMP is removed by phosphodiesterase type 5 (PDE5), an enzyme that converts cGMP into guanosine monophosphate. Sildenafil [Viagra] was introduced in 1998 as the first oral treatment for ED. The drug is reliable and easy to use. Benefits derive from enhancing the natural response to sexual stimuli; sildenafil does not cause erection directly. Although sildenafil is generally well tolerated, it can be dangerous for men taking certain vasodilators, specifically alpha-adrenergic blockers, and nitroglycerin and other nitrates used for angina pectoris. In addition to ED, sildenafil is approved for pulmonary arterial hypertension (PAH) (see Chapter 107). • Myocardial infarction, stroke, or life-threatening dysrhythmia within the last 6 months • Resting hypotension (blood pressure below 90/50 mm Hg) • Resting hypertension (blood pressure above 170/110 mm Hg) Vardenafil and tadalafil are very similar to sildenafil. All three drugs inhibit PDE5, and all three are approved for oral therapy of ED. Vardenafil is unique in that it prolongs the QT interval, and tadalafil is unique in that its effects last 36 hours. Otherwise, the clinical effects of all three drugs appear about equal, although some patients may respond better to one than to the others. Properties of all three are summarized in Table 66–2. TABLE 66–2
Drugs for erectile dysfunction and benign prostatic hyperplasia
Erectile dysfunction

Drug Class
Representative Drug
Incidence of SD/ED*
Renal/Cardiovascular Drugs
Cardiac Glycosides
Digoxin [Lanoxin]
36%
Adrenergic Neuron Blockers
Reserpine
24%–40%
Central Alpha2-Adrenergic Agonists
Methyldopa
20%–30%
Beta Blockers
Propranolol [Inderal]
10%–15%
Thiazide Diuretics
Hydrochlorothiazide
10%–20%
Aldosterone Antagonists
Spironolactone [Aldactone]
4%–30%
CNS Drugs
Selective Serotonin Reuptake Inhibitors
Fluoxetine [Prozac]
Up to 70%
Monoamine Oxidase Inhibitors
Isocarboxazid [Marplan]
16%–31%
Tricyclic Antidepressants
Amitriptyline [Elavil]
7%–30%
Antipsychotics
Chlorpromazine [Thorazine]
30%–60%
Mood Stabilizers
Lithium [Lithobid]
5%–50%
Social Lubricant/Intoxicant
Alcohol [Johnny Walker]
50%–75%
Urogenital Drugs
5-Alpha-Reductase Inhibitors
Finasteride [Proscar]
33%
Physiology of erection
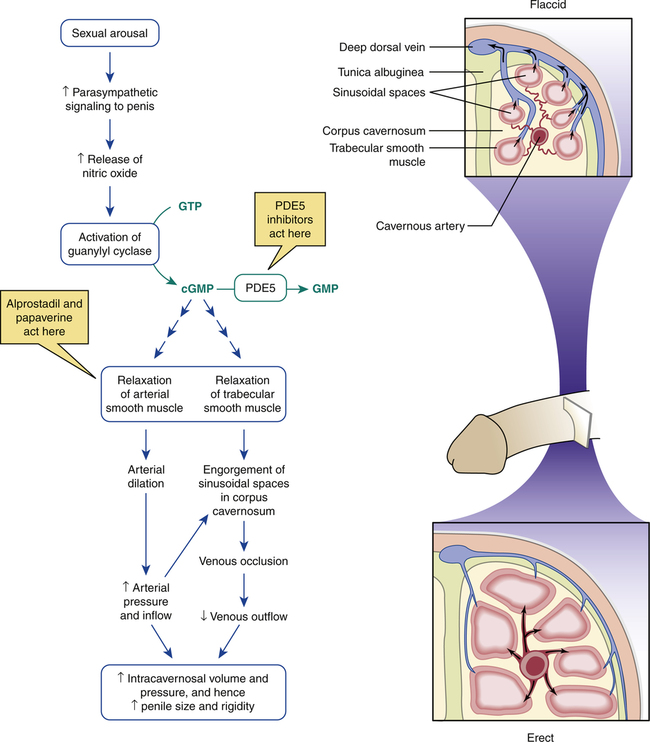
 Physiology of penile erection.
Physiology of penile erection.
In the flaccid state, there is free outflow of venous blood and restricted inflow of arterial blood. During sexual arousal, cGMP relaxes arterial and trabecular smooth muscle, thereby permitting free inflow of arterial blood and subsequent engorgement of sinusoidal spaces, whose expansion compresses penile veins, thereby restricting blood outflow. The resultant accumulation of blood at elevated pressure increases penile size and rigidity. Removal of cGMP by PDE5 restores penile smooth muscle to the nonaroused state, and hence detumescence ensues. (cGMP = cyclic guanosine monophosphate, GMP = guanosine monophosphate, GTP = guanosine triphosphate, PDE5 = phosphodiesterase type 5.)
Oral drugs for ED: PDE5 inhibitors
Sildenafil
Is sildenafil safe for men with CHD?

Drug
Parameter
Sildenafil [Viagra]
Tadalafil [Cialis]
Vardenafil [Levitra, Staxyn]
Date approved
3/27/1998
11/21/2003
8/19/2003
Dosing schedule
PRN only
PRN or once daily
PRN only
Dosing with food
May be taken without regard to meals—but high-fat meals delay absorption and reduce peak levels
May be taken without regard to meals
May be taken without regard to meals—but high-fat meals delay absorption and reduce peak levels
Median time to peak level
1 hr
2 hr
1 hr
Half-life
4 hr
17.5 hr
4–5 hr
Duration of action
4 hr
36 hr
4 hr
Major mode of metabolism
CYP3A4
CYP3A4
CYP3A4
Drug interactions
Nitrates
Contraindicated: Wait 24 hr before giving a nitrate
Contraindicated: Wait 48 hr before giving a nitrate
Contraindicated: Wait 24 hr before giving a nitrate
Alpha blockers
Use with caution
Contraindicated (except for tamsulosin, 0.4 mg once daily)
Contraindicated
CYP3A4 inhibitors
Reduce sildenafil dosage
Reduce tadalafil dosage to no more than 10 mg every 72 hr
Reduce vardenafil dosage
Class I and class III antidysrhythmic drugs
No interaction
No interaction
Vardenafil prolongs the QT interval—avoid class I and class III antidysrhythmics ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



Drugs for erectile dysfunction and benign prostatic hyperplasia
Get Clinical Tree app for offline access