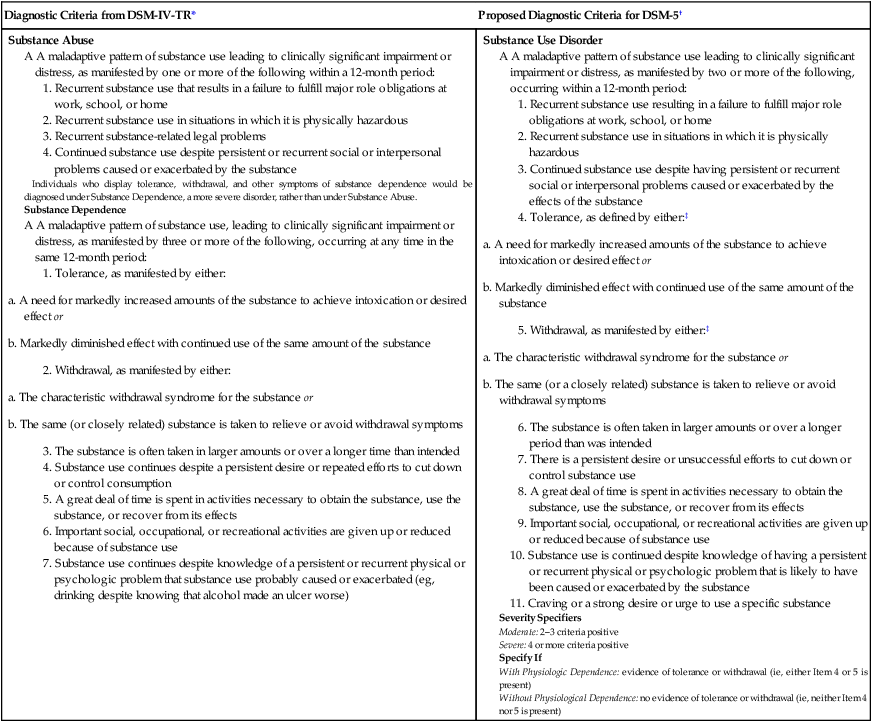
CHAPTER 37 Our discussion of drug abuse occurs in two stages. In this chapter, we discuss basic concepts in drug abuse. In Chapters 38, 39, and 40, we focus on the pharmacology of specific abused agents and methods of treatment. The American Psychiatric Association (APA) has established diagnostic criteria for disorders relating to drugs of abuse. The criteria now in use, published in the fourth edition of the APA’s Diagnostics and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), were released in 1994. Revised criteria will be published in the fifth edition (DSM-5), scheduled for release in 2013. The new criteria, viewable online at www.DSM5.org, differ significantly from the criteria in DSM-IV. Both sets of criteria are summarized in Table 37–1. As the table shows, DSM-IV divides substance use disorders into two major groups: substance abuse and substance dependence. Substance dependence, which can be equated with our definition of addiction, is a more severe disorder than substance abuse. Accordingly, individuals whose drug problem is not bad enough to meet the criteria for substance dependence might nonetheless meet the criteria for substance abuse. In DSM-5, the criteria for substance abuse and substance dependence will be merged into a single, new diagnostic category—substance use disorder—which will replace the two older categories. This change is welcome in that the distinction between substance abuse and substance dependence is somewhat vague, and hence has been a source of confusion. TABLE 37–1 American Psychiatric Association Diagnostic Criteria Pertaining to Drugs of Abuse *Modified from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC: American Psychiatric Association, 2000, with permission. Copyright © 2000 American Psychiatric Association. †Modified from the proposed diagnostic criteria for a Substance Use Disorder, to be published in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Washington, DC: American Psychiatric Association. Expected publication date: May 2013. Copyright © American Psychiatric Association. The proposed criteria are from the DSM-5 web site—www.DSM5.org—accessed on November 12, 2010. ‡Tolerance and withdrawal are not counted if they develop for medications (eg, analgesics, anxiolytics) taken under medical supervision.
Drug abuse I: basic considerations
APA diagnostic criteria regarding drugs of abuse

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Drug abuse I: basic considerations
Only gold members can continue reading. Log In or Register to continue
