Developmental Theories
Objectives
• Discuss factors influencing growth and development.
• Describe biophysical developmental theories.
• Describe and compare the psychoanalytical/psychosocial theories proposed by Freud and Erikson.
• Describe Piaget’s theory of cognitive development.
• Discuss nursing implications for the application of developmental principles to patient care.
Key Terms
Biophysical development, p. 131
Conventional reasoning, p. 135
Erikson’s theory of psychosocial development, p. 132
Freud’s psychoanalytical model of personality development, p. 131
Kohlberg’s theory of moral development, p. 135
Piaget’s theory of cognitive development, p. 134
Postconventional reasoning, p. 136
Temperament, p. 133

Understanding normal growth and development helps nurses predict, prevent, and detect deviations from patients’ own expected patterns. Growth encompasses the physical changes that occur from the prenatal period through older adulthood and also demonstrates both advancement and deterioration. Young children grow more quickly than older children, and by adulthood growth in height ceases. In late adulthood there is a loss of both muscle and bone, which may cause a decrease in height in some people (Santrock, 2009). Development refers to the biological, cognitive, and socioemotional changes that begin at conception and continue throughout a lifetime. Development is dynamic and includes progression. However, in some disease processes development is delayed or regresses. For example, older adults demonstrate cognitive development resulting in wisdom as they incorporate life experiences into decision making, but they do not perform as well as young adults when speed is required for information processing (Santrock, 2008).
Individuals have unique patterns of growth and development. The ability to progress through each developmental phase influences the overall health of the individual. The success or failure experienced within a phase affects the ability to complete subsequent phases. If individuals experience repeated developmental failures, inadequacies sometimes result. However, when the individual experiences repeated successes, health is promoted. For example, a child who does not walk by 20 months may demonstrate delayed gross motor ability that slows exploration and manipulation of the environment. In contrast, a child who walks by 10 months is able to explore and find stimulation in the environment.
Today nurses need to adopt a life span perspective of human development that takes into account all developmental stages of life. Traditionally development focused on childhood, but a comprehensive view of development also includes the changes that occur during the adult years. An understanding of growth and development throughout the life span assists in planning questions for health screening and health history and in health teaching for patients of all ages.
Developmental Theories
Developmental theories provide a framework for examining, describing, and appreciating human development. For example, knowledge of Erikson’s psychosocial theory of development helps caregivers understand the importance of supporting the development of basic trust in the infancy stage. Trust establishes the foundation for all future relationships. Developmental theories are also important in helping nurses assess and treat a person’s response to an illness. Understanding the specific task or need of each developmental stage guides caregivers in planning appropriate individualized care for patients. Specific developmental theories that define the aging process for adults are discussed in Chapters 13 and 14.
Human development is a dynamic and complex process that cannot be explained by only one theory. This chapter presents biophysical, psychoanalytical/psychosocial, cognitive, and moral developmental theories. Chapters 25 and 35 cover the areas of learning theory for patient teaching and spiritual development.
Biophysical Developmental Theories
Biophysical development is how our physical bodies grow and change. Health care providers are able to quantify and compare the changes that occur as a newborn infant grows into adulthood against established norms. How does the physical body age? What are the triggers that move the body from the physical characteristics of childhood, through adolescence, to the physical changes of adulthood?
Gesell’s Theory of Development
Fundamental to Gesell’s theory of development is that each child’s pattern of growth is unique and this pattern is directed by gene activity (Gesell, 1948). Gesell found the pattern of maturation follows a fixed developmental sequence in humans. Sequential development is evident in fetuses, in which there is a specified order of organ system development. Today we know that growth in humans is both cephalocaudal and proximodistal. The cephalocaudal pattern describes the sequence in which growth is fastest at the top (head and then down); proximodistal growth starts at the center of the body and moves toward the extremities.
Genes direct the sequence of development; but environmental factors also influence development, resulting in developmental changes. For example, genes may direct the growth rate for an individual, but that growth is only maximized if environmental conditions are adequate. Poor nutrition or chronic disease often affects the growth rate and results in smaller stature, regardless of the genetic blueprint. However, adequate nutrition and the absence of disease cannot result in stature beyond that determined by heredity.
Psychoanalytical/Psychosocial Theory
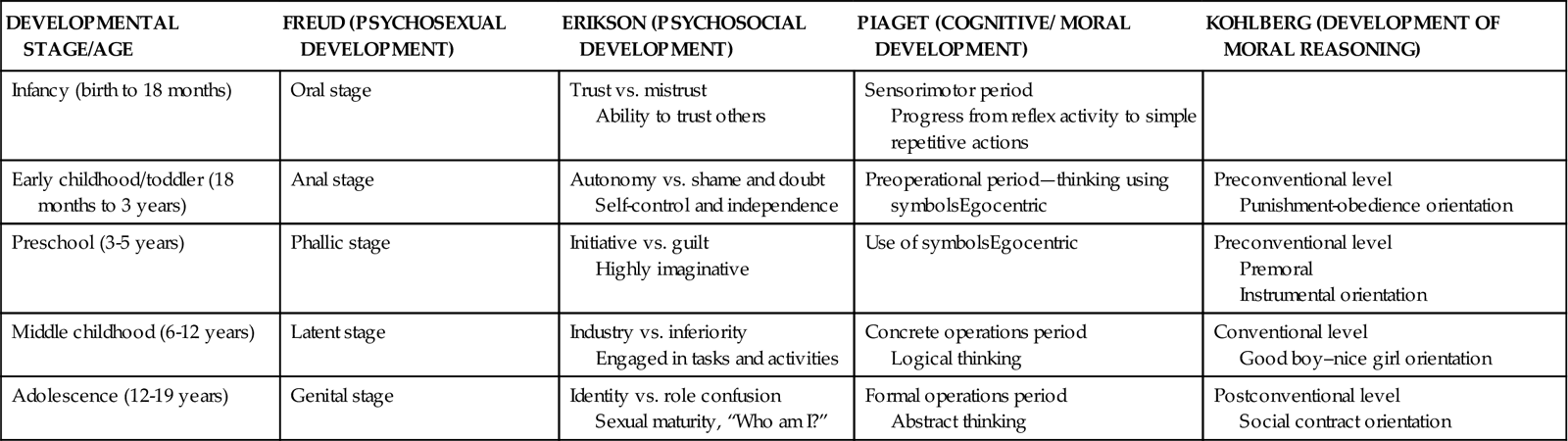
Theories of psychoanalytical/psychosocial development describe human development from the perspectives of personality, thinking, and behavior (Table 11-1). Psychoanalytical theory explains development as primarily unconscious and influenced by emotion. Psychoanalytical theorists maintain that these unconscious drives influence development through universal stages experienced by all individuals (Berger, 2007).
TABLE 11-1
Comparison of Major Developmental Theories
| DEVELOPMENTAL STAGE/AGE | FREUD (PSYCHOSEXUAL DEVELOPMENT) | ERIKSON (PSYCHOSOCIAL DEVELOPMENT) | PIAGET (COGNITIVE/ MORAL DEVELOPMENT) | KOHLBERG (DEVELOPMENT OF MORAL REASONING) |
| Infancy (birth to 18 months) | Oral stage | Trust vs. mistrust Ability to trust others | Sensorimotor period Progress from reflex activity to simple repetitive actions | |
| Early childhood/toddler (18 months to 3 years) | Anal stage | Autonomy vs. shame and doubt Self-control and independence | Preoperational period—thinking using symbolsEgocentric | Preconventional level Punishment-obedience orientation |
| Preschool (3-5 years) | Phallic stage | Initiative vs. guilt Highly imaginative | Use of symbolsEgocentric | Preconventional level Premoral Instrumental orientation |
| Middle childhood (6-12 years) | Latent stage | Industry vs. inferiority Engaged in tasks and activities | Concrete operations period Logical thinking | Conventional level Good boy–nice girl orientation |
| Adolescence (12-19 years) | Genital stage | Identity vs. role confusion Sexual maturity, “Who am I?” | Formal operations period Abstract thinking | Postconventional level Social contract orientation |
Sigmund Freud
Freud’s psychoanalytical model of personality development states that individuals go through five stages of psychosexual development and that each stage is characterized by sexual pleasure in parts of the body: the mouth, the anus, and the genitals. Freud believed that adult personality is the result of how an individual resolved conflicts between these sources of pleasure and the mandates of reality (Berger, 2007; Santrock, 2009).
Stage 1: Oral (Birth to 12 to 18 Months)
Initially sucking and oral satisfaction are not only vital to life but also extremely pleasurable in their own rights. Late in this stage the infant begins to realize that the mother/parent is something separate from self. Disruption in the physical or emotional availability of the parent (e.g., inadequate bonding or chronic illness) could affect an infant’s development.
Stage 2: Anal (12 to 18 Months to 3 Years)
The focus of pleasure changes to the anal zone. Children become increasingly aware of the pleasurable sensations of this body region with interest in the products of their effort. Through the toilet-training process the child delays gratification to meet parental and societal expectations.
Stage 3: Phallic or Oedipal (3 to 6 Years)
The genital organs are the focus of pleasure during this stage. The boy becomes interested in the penis; the girl becomes aware of the absence of the penis, known as penis envy. This is a time of exploration and imagination as the child fantasizes about the parent of the opposite sex as his or her first love interest, known as the Oedipus or Electra complex. By the end of this stage the child attempts to reduce this conflict by identifying with the parent of the same sex as a way to win recognition and acceptance.
Stage 4: Latency (6 to 12 Years)
In this stage Freud believed that sexual urges from the earlier oedipal stage are repressed and channeled into productive activities that are socially acceptable. Within the educational and social worlds of the child, there is much to learn and accomplish.
Stage 5: Genital (Puberty Through Adulthood)
In this final stage sexual urges reawaken and are directed to an individual outside the family circle. Unresolved prior conflicts surface during adolescence. Once the individual resolves conflicts, he or she is then capable of having a mature adult sexual relationship.
Freud believed that the components of the human personality develop in stages and regulate behavior. These components are the id, the ego, and the superego. The id (i.e., basic instinctual impulses driven to achieve pleasure) is the most primitive part of the personality and originates in the infant. The ego represents the reality component, mediating conflicts between the environment and the forces of the id. The ego helps people judge reality accurately, regulate impulses, and make good decisions. The third component, the superego, performs regulating, restraining, and prohibiting actions. Often referred to as the conscience, the superego is influenced by the standards of outside social forces (e.g., parent or teacher).
Some of Freud’s critics contend that he based his analysis of personality development on biological determinants and ignored the influence of culture and experience. Other critics think that Freud’s basic assumptions such as the Oedipus complex are not applicable across different cultures. Psychoanalysts today believe that the role of conscious thought is much greater than Freud imagined (Santrock, 2008).
Erik Erikson
Freud had a strong influence on his psychoanalytical followers, including Erik Erikson (1902-1994), who constructed a theory of development that differed from Freud’s in two major views. Erikson maintained that development occurred throughout the life span and that it focused on psychosocial stages rather than psychosexual stages.
According to Erikson’s theory of psychosocial development, individuals need to accomplish a particular task before successfully mastering the stage and progressing to the next one. Each task is framed with opposing conflicts, and tasks once mastered are challenged and tested again during new situations or at times of conflict (Hockenberry and Wilson, 2011). Erikson’s eight stages of life are described here.
Trust versus Mistrust (Birth to 1 Year)
Establishing a basic sense of trust is essential for the development of a healthy personality. The infant’s successful resolution of this stage requires a consistent caregiver who is available to meet his needs. From this basic trust in parents, the infant is able to trust in himself, in others, and in the world (Hockenberry and Wilson, 2011). The formation of trust results in faith and optimism. A nurse’s use of anticipatory guidance helps parents cope with the hospitalization of an infant and the infant’s behaviors when discharged to home.
Autonomy versus Sense of Shame and Doubt (1 to 3 Years)
By this stage a growing child is more accomplished in some basic self-care activities, including walking, feeding, and toileting. This newfound independence is the result of maturation and imitation. The toddler develops his or her autonomy by making choices. Choices typical for the toddler age-group include activities related to relationships, desires, and playthings. There is also opportunity to learn that parents and society have expectations about these choices. Limiting choices and/or enacting harsh punishment leads to feelings of shame and doubt. The toddler who successfully masters this stage achieves self-control and willpower. The nurse models empathetic guidance that offers support for and understanding of the challenges of this stage.
Initiative versus Guilt (3 to 6 Years)
Children like to pretend and try out new roles. Fantasy and imagination allow them to further explore their environment. Also at this time they are developing their superego, or conscience. Conflicts often occur between the child’s desire to explore and the limits placed on his or her behavior. These conflicts sometimes lead to feelings of frustration and guilt. Guilt also occurs if the caregiver’s responses are too harsh. Preschoolers are learning to maintain a sense of initiative without imposing on the freedoms of others. Successful resolution of this stage results in direction and purpose. Teaching the child impulse control and cooperative behaviors helps the family avoid the risks of altered growth and development.
Industry versus Inferiority (6 to 11 Years)
School-age children are eager to apply themselves to learning socially productive skills and tools. They learn to work and play with their peers. They thrive on their accomplishments and praise. Without proper support for learning new skills or if skills are too difficult, they develop a sense of inadequacy and inferiority. Children at this age need to be able to experience real achievement to develop a sense of competency. Erikson believed that the adult’s attitudes toward work are traced to successful achievement of this task (Erikson, 1963). During hospitalization it is important for the school-age child to understand the routines and participate as actively as possible in his or her treatment. For example, some children enjoy keeping a record of their intake and output.
Identity versus Role Confusion (Puberty)
Dramatic physiological changes associated with sexual maturation mark this stage. There is a marked preoccupation with appearance and body image. This stage, in which identity development begins with the goal of achieving some perspective or direction, answers the question, “Who am I?” Acquiring a sense of identity is essential for making adult decisions such as choice of a vocation or marriage partner. Each adolescent moves in his or her unique way into society as an interdependent member. There are also new social demands, opportunities, and conflicts that relate to the emergent identity and separation from family. Erikson held that successful mastery of this stage resulted in devotion and fidelity to others and to their own ideals (Hockenberry and Wilson, 2011). The nurse provides education and anticipatory guidance for the parent about the changes and challenges to the adolescent. Nurses also help hospitalized adolescents deal with their illness by giving them enough information to allow them to make decisions about their treatment plan.
Intimacy versus Isolation (Young Adult)
Young adults, having developed a sense of identity, deepen their capacity to love others and care for them. They search for meaningful friendships and an intimate relationship with another person. Erikson portrayed intimacy as finding the self and then losing the self in another (Santrock, 2008). If the young adult is not able to establish companionship and intimacy, isolation results because he or she fears rejection and disappointment (Berger, 2007). Nurses must understand that hospitalization increases a young adults’ need for intimacy; thus young adults benefit from the support of their partner or significant other during this time.
Generativity versus Self-Absorption and Stagnation (Middle Age)
Following the development of an intimate relationship, the adult focuses on supporting future generations. The ability to expand one’s personal and social involvement is critical to this stage of development. Middle-age adults achieve success in this stage by contributing to future generations through parenthood, teaching, and community involvement. Achieving generativity results in caring for others as a basic strength. Inability to play a role in the development of the next generation results in stagnation (Santrock, 2008). Nurses assist physically ill adults in choosing creative ways to foster social development. Middle-age persons often find a sense of fulfillment by volunteering in a local school, hospital, or church.
Integrity versus Despair (Old Age)
Many older adults review their lives with a sense of satisfaction, even with their inevitable mistakes. Others see themselves as failures, with their lives marked by despair and regret. Older adults often engage in a retrospective appraisal of their lives. They interpret their lives as a meaningful whole or experience regret because of goals not achieved (Berger, 2007). Because the aging process creates physical and social losses, some adults also suffer loss of status and function (e.g., through retirement or illness). These external struggles are also met with internal struggles such as the search for meaning in life. Meeting these challenges creates the potential for growth and the basic strength of wisdom (Fig. 11-1).

Nurses are in positions of influence within their communities to help people feel valued, appreciated, and needed. Erikson stated, “Healthy children will not fear life, if their parents have integrity enough not to fear death” (Erikson, 1963). Although Erikson believed that problems in adult life resulted from unsuccessful resolution of earlier stages, his emphasis on family relationships and culture offered a broad, life-span view of development. As a nurse, you will use this knowledge of development as you deliver care in any health care setting.
Theories Related to Temperament
Temperament is a behavioral style that affects an individual’s emotional interactions with others (Santrock, 2008). Personality and temperament are often closely linked, and research shows that individuals possess some enduring characteristics into adulthood. The individual differences that children display in responding to their environment significantly influence the way others respond to them and their needs. Knowledge of temperament helps parents better understand their child (Hockenberry and Wilson, 2011).
Psychiatrists Stella Chess (1914-2007) and Alexander Thomas (1914-2003) conducted a 20-year longitudinal study that identified three basic classes of temperament:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


