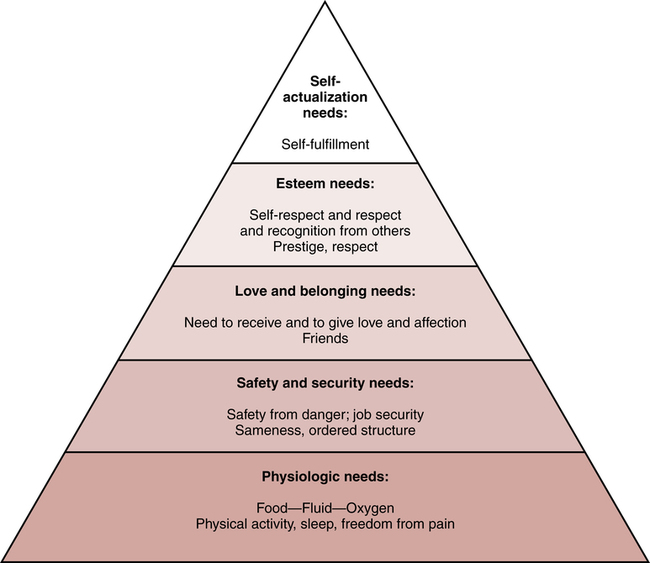
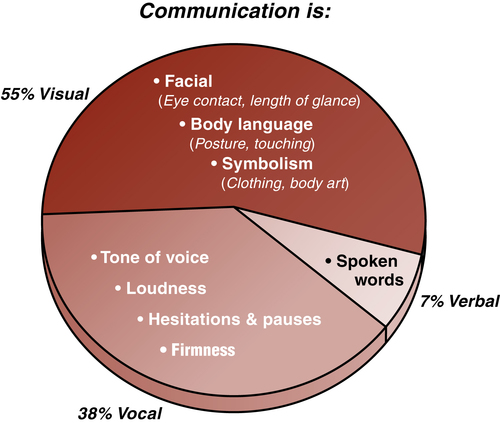
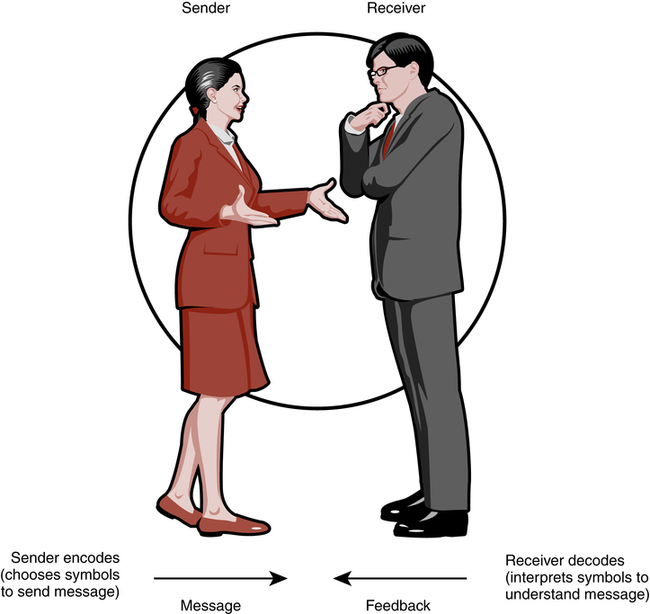
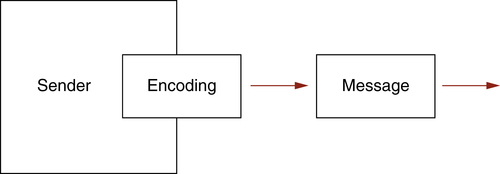
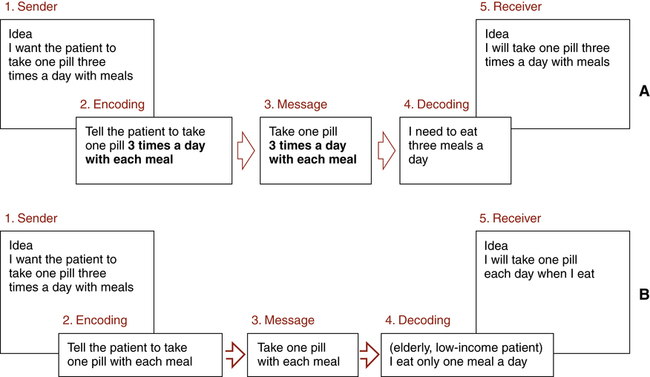
On completion of this chapter, you will be able to: 1. Define the terms in the vocabulary list. 2. Explain why implementation of the electronic medical record is requiring advanced communication and skills for the health unit coordinator (HUC). 3. Give instances that exemplify human needs, classify each according to Maslow’s hierarchy of human needs, and give appropriate responses to meet the listed needs. 4. List four components of the communication process. 5. Interpret and apply the communication model. 6. Explain how unsuccessful communication can occur during the encoding and decoding process. 7. Discuss two types of nonverbal communication. 8. List five levels of listening and nine ways to improve listening skills. 9. List five ways to improve feedback skills. 10. Define and explain the importance of culturally sensitive care in the health care setting. 11. List five guidelines to follow that could improve intercultural communication. 12. Identify assertive, nonassertive, and aggressive behaviors, and evaluate your assertiveness; and respond to situations using assertiveness skills. 13. List six steps to follow when dealing on the telephone with a person who is angry. 14. Identify five ways that communication and interpersonal skills are used in the health care setting. 15. List 12 preceptor guidelines for training a HUC student or a new employee. 16. List 10 student guidelines for completing the clinical experience. Stereotyping of and discrimination against individuals or groups because of their age. A disagreement or clash among ideas, values, principles, or people. A set of values, beliefs, and traditions that are held by a specific social group. A person’s need for self-respect and for the respect of others. The inability to accept other cultures, or an assumption of cultural superiority. Verbal or nonverbal response to a message. An experienced working HUC who is selected to train or teach a HUC student or a new employee. A person’s need to have affectionate relationships with people and to have a place in a group. Attempts at influencing or controlling others’ actions or behaviors to one’s own advantage. Images, feelings, and ideas transmitted from one person to another. An assertive skill in which a person requests clarification of a criticism to get to the real issue. A behavioral style in which a person allows others to dictate her or his self-worth. Repeating a message back to the sender in one’s own words to clarify meaning. A person’s physical needs, such as the need for food and water. To train or teach (a student or a new employee). The person who receives a message. The need to maximize one’s potential. Confidence in and respect for oneself. The person who transmits a message. The use of language or actual spoken words. Dealing with conflict in such a way that the solution is satisfactory to all parties. The health unit coordinator (HUC) is the liaison among the doctor, the nursing staff, ancillary departments, visitors, and patients. The main responsibility of the HUC is to keep the nursing unit running effectively and smoothly. With the implementation of the electronic medical record (EMR), the HUC has expanded responsibilities and is often the “go-to” person to assist doctors, nurses, and ancillary personnel in use of the EMR system. The HUC also has a larger role in listening to visitor, patient, and nursing unit personnel complaints and also in problem solving. The nursing unit can become very hectic, and tensions can build easily. If communication breaks down and tempers become short, chaos most likely will result, and the risk of errors being made becomes higher. Hospitals are rated by The Joint Commission (TJC) on patient safety goals that include the communication process. The HUC as well as all health care professionals need to stay proactive to meet the requirements placed on the hospital. Many hospitals provide computer-based learning (including communication and other topics) for employees that can be completed on their own time. Although several models may be used to study interpersonal behavior, we have chosen Maslow’s hierarchy of needs, developed by the late Abraham Maslow, a famous psychologist. Maslow’s human needs model emphasizes that all people have the same basic needs and that these needs motivate and influence a person’s behavior, consciously or unconsciously. The needs are arranged in a pyramid, with the most basic or immediate needs at the bottom of the pyramid and less critical needs at the top of the pyramid (Fig. 5-1). Needs that are lower on the pyramid have the greatest influence on a person’s behavior. For instance, a person will work harder to meet the need for water to drink than to meet the need for self-esteem. HUC: “Mary is in isolation. You will need to put this gown on before going into her room.” (No dominant need expressed.) Husband: “Mary is in isolation? What are you talking about? What for? I want to know exactly what is going on here!” (Safety need expressed. Mary’s husband is concerned about her safety and is also concerned that he may contract what Mary has.) HUC (defensively): “Look, if you don’t want to wear the gown, don’t go in. I don’t make the rules here.” (Esteem need expressed. The HUC interprets the husband’s request for information as an attack on her competence; self-esteem is at stake. Fighting back is used to try to satisfy self-esteem needs.) Communication is 55% visual, including facial body language and symbolism; 38% vocal qualities, including tone, loudness, firmness, hesitations, and pauses; and 7% verbal, meaning actual words (Fig. 5-2). There is often inconsistency between what a person is saying and how he or she appears. (“Of course I’m listening to you, Mother,” says the 9-year-old boy as he sits glued to the television set, leaving the mother wondering whether the child is indeed listening to her.) Daughter: I’ve stopped eating breakfast meats. Mother: But breakfast is the most important meal of the day. You should not give it up. Communication takes place daily with nurses (Fig. 5-3, A), physicians (Fig. 5-3, B), allied health professionals, patients (Fig. 5-3, C), visitors, and administrators. The HUC is often the first person seen by the new patient and visitors. The words, gestures, facial expression, and body posture that are used can suggest that one is opinionated, supportive, thoughtful, or insecure. The tone of voice, the words spoken, and the facial expressions used during the patient’s or the visitor’s initial contact with the nursing unit leave a lasting impression. A model is a representation of a process—a map, for instance. We will use a model to take a closer look at the communication process, to identify why so many of us communicate poorly, and to find ways to improve our ability to communicate with others (Fig. 5-4). The sender must translate mental images, feelings, and ideas into symbols to communicate them to the receiver. This process is called encoding. When encoding, the sender decides whether to send the message in verbal symbols or in nonverbal symbols (Fig. 5-5). What are the right words to use so the receiver will understand the message? Different words are used if you are speaking to a child, to an adult, or to another health care professional. Nonverbal symbols, such as facial expressions, may be used to communicate the message. Encoding occurs each time we communicate. A poor choice of words or an inconsistency between verbal and nonverbal messages may result in unsuccessful communication. As the message reaches the receiver, the verbal and nonverbal symbols are decoded. Decoding is the process of translating symbols received from the sender to determine the message. Unsuccessful decoding can be caused by inconsistency in the verbal and nonverbal symbols received from the sender. For instance, “Of course I love you” said harshly may be difficult to decode correctly. Lifestyle, age, cultural background, environment, and poor listening habits are other reasons for incorrect decoding. In successful communication, the ideas, feelings, and images of the sender match those of the receiver (Fig. 5-6, A). In unsuccessful communication, errors occur in encoding or in decoding the message (Fig. 5-6, B). Nonverbal communication can be separated into two types: symbolic and body language. 1. Ignoring: making no effort to listen 2. Pretend listening: giving the appearance that you are listening 3. Selective listening: hearing only the parts that interest you 4. Attentive listening (also called active listening): paying attention and focusing on what the speaker says and comparing it with your own experience 5. Empathic listening: listening and responding with both the heart and the mind to truly understand, realizing that all persons have the right to feel as they do
Communication and Interpersonal Skills
Expanding Communication Role for the Health Unit Coordinator
Interpersonal Behavior
Examples of Different Needs in a Conversation
Communication Skills
Communication Model
Sender
Receiver
Verbal and Nonverbal Communication
Types of Nonverbal Communication
Symbolic
Body Language
Clothing
Posture
Hair
Ambulation
Jewelry
Touching
Body art
Personal distance
Cosmetics
Eye contact
Automobile
Breathing
House
Hand gestures
Perfume or cologne
Facial expressions
Listening Skills
Five Levels of Listening
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Communication and Interpersonal Skills
 EXERCISE 1
EXERCISE 1
Get Clinical Tree app for offline access
