Communicating With the Health Team
Objectives
• Define the key terms and key abbreviations in this chapter.
• Explain why health team members need to communicate.
• Describe the rules for good communication.
• Explain the purpose, parts, and information found in the medical record.
• Describe the legal and ethical aspects of medical records.
• Describe the purpose of the Kardex and care summary.
• List the information you need to report to the nurse.
• List the rules for recording.
• Explain how computers and other electronic devices are used in health care.
• Explain how to protect the right to privacy when using computers and other electronic devices.
• Describe how to answer phones.
• Use the 24-hour clock, medical terminology, and medical abbreviations.
• Explain how to promote PRIDE in the person, the family, and yourself.
Key Terms
Key Abbreviations
| ADL | Activities of daily living |
| EHR | Electronic health record |
| EMR | Electronic medical record |
| EPHI; ePHI | Electronic protected health information |
| PHI | Protected health information |
Health team members communicate with each other to give coordinated and effective care. They share information about:
For example, the doctor ordered a blood test for Mr. Bloom. Food and fluids affect the test results. Mr. Bloom must fast for 10 hours before the blood is drawn. A nurse tells the dietary department that Mr. Bloom will have breakfast later. She explains the breakfast delay to you and Mr. Bloom. A technician tells the nurse the blood sample was drawn. The nurse orders the meal. A dietary worker brings the tray to the nursing unit. You serve Mr. Bloom’s tray. When he is done eating, you remove the tray and observe what he ate. You report your observations to the nurse. The nurse records your observations in Mr. Bloom’s medical record.
Team members communicated with each other and Mr. Bloom. His care was coordinated and effective. He knew that he was not neglected or forgotten.
You need to understand the aspects and rules of communication. Then you can learn how to communicate with the nursing and health teams.
Communication
Communication is the exchange of information—a message sent is received and correctly interpreted by the intended person. For good communication:
The Medical Record
The medical record (chart, clinical record) is the legal account of a person’s condition and response to treatment and care. Medical records are written using paper forms or electronically through the use of computers (Fig. 7-1). An electronic health record (EHR) or electronic medical record (EMR) is an electronic version of a person’s medical record. More and more agencies are using EHRs (EMRs). In time, all medical records will be electronic.

The health team uses the medical record to share information about the person. The record is a permanent legal document. Often it is used months or years later if the person’s health history is needed. It can be used in court as legal evidence of the person’s problems, treatment, and care.
The record is organized into sections. Each page has the person’s name, room and bed number, and other identifying information. Common parts of the record include:
• Physical examination results
• Progress notes (nursing team and health team)
• Graphic sheets and flow sheets
• Therapy records: intravenous (IV), respiratory, and others
• Assessments from nursing, social services, dietary services, and recreational therapy
The health team records on forms for their departments. Other team members read the information. It tells the care provided and the person’s response.
Agencies have policies about medical records and who can see them. Policies address:
Some agencies allow nursing assistants to record observations and care. Others do not. You must follow your agency’s policies.
Professional staff involved in a person’s care can review charts. Cooks and laundry, housekeeping, and office staff do not need to read charts. Some agencies let nursing assistants read charts. If not, the nurse shares needed information.
You have an ethical and legal duty to keep the person’s information confidential. You may know someone in the agency. If not involved in the person’s care, you have no right to review the person’s chart. Doing so is an invasion of privacy.
Patients and residents have the right to the information in their medical records. The person or the person’s legal representative may ask to see the chart. Report the request to the nurse. The nurse handles the request.
The following parts of the medical record relate to your work. They may be paper forms or electronic records.
The Admission Record
The admission record is completed when the person is admitted to the agency. It has the person’s identifying information—legal name, birth date, age, gender (male or female), address, and marital status. Nearest relative and legal representative names are included. Other information includes known allergies, diagnoses, date and time of admission, and doctor’s name. Religion, place of worship, and employer are often included.
Each person receives an identification (ID) number. It is on the admission record and ID bracelet (Chapter 13). So is information about advance directives. An advance directive is a document stating a person’s wishes about end-of-life care (Chapter 55).
Use the admission record for forms needing the same information. That way the person does not have to answer the same question many times.
Health History
The health history (nursing history) is completed when the person is admitted. The nurse interviews the person. You can use the form to learn about the person’s background and health history. It contains information about:
The Graphic Sheet
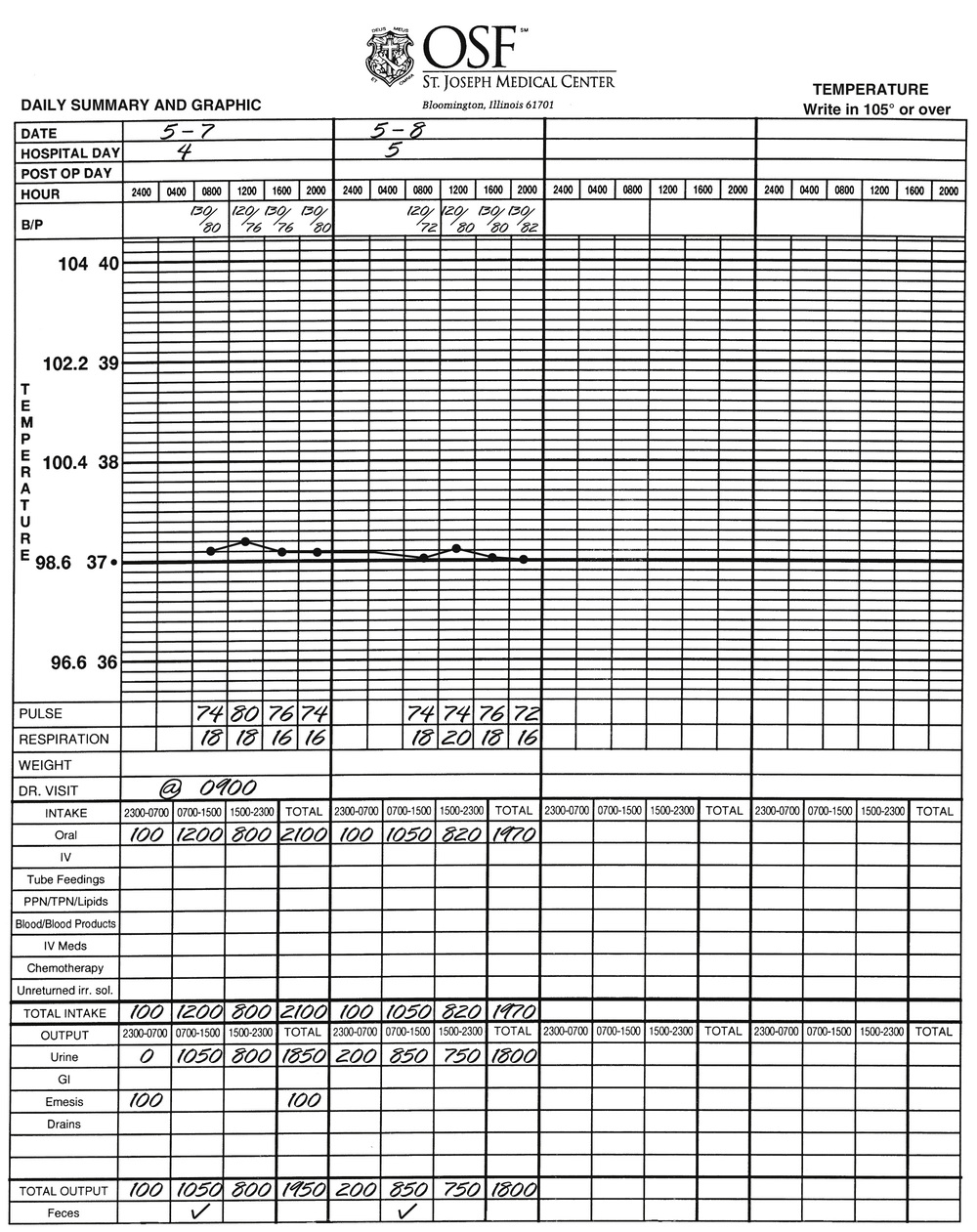
The graphic sheet is used to record measurements and observations made daily, every shift, or 3 to 4 times a day (Fig. 7-2, p. 70). Information includes vital signs—blood pressure, temperature, pulse, respirations. It also includes weight, intake and output (Chapter 27), bowel movements (feces), and doctor’s visits.
Progress Notes
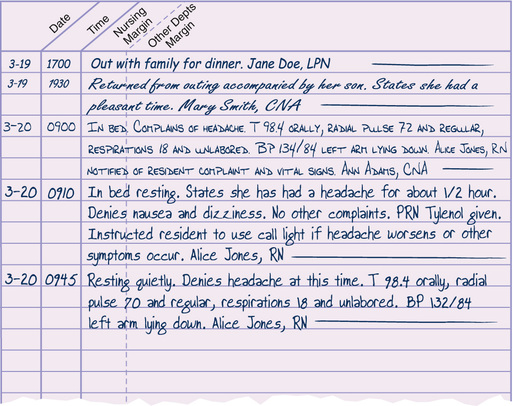
The progress note describes the care given and the person’s response and progress (Fig. 7-3, p. 71). The nurse records:
• Information about treatments and drugs
• Information about teaching and counseling
• Procedures performed by the doctor
See Focus on Long-Term Care and Home Care: Progress Notes.
Flow Sheets
Flow sheets are used to record frequent measurements or observations. For example, vital signs are measured every 30 minutes. A vital signs flow sheet is used. The bedside intake and output record is another flow sheet (Chapter 27).
See Focus on Long-Term Care and Home Care: Flow Sheets.
Focus on Long-Term Care and Home Care
Flow Sheets
Long-Term Care
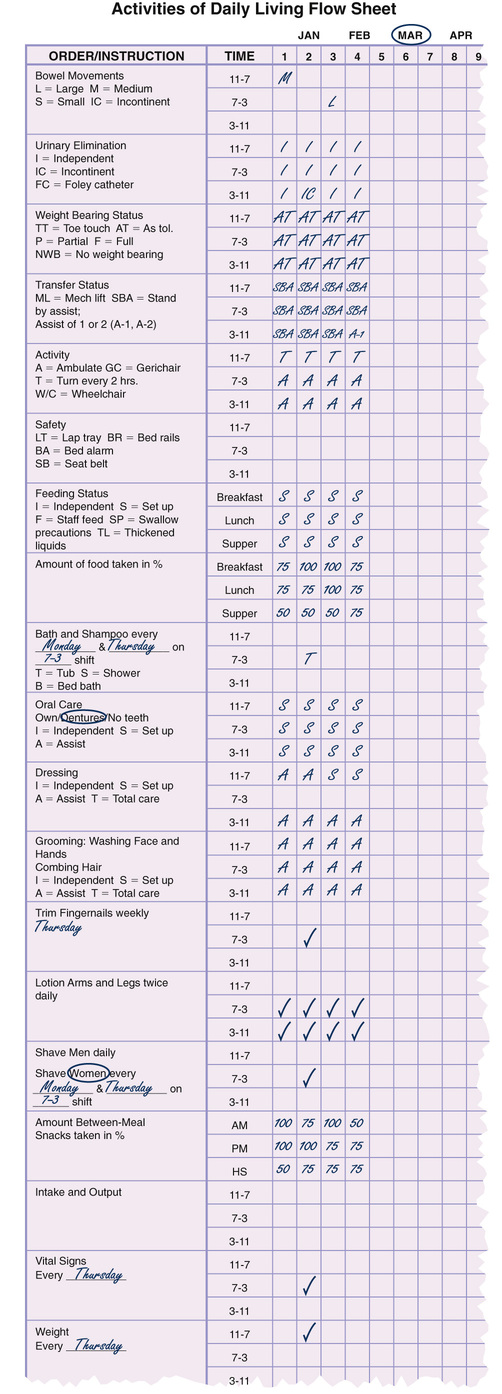
An activities of daily living (ADL) flow sheet is used to record a person’s ability to perform ADL (Fig. 7-4). This flow sheet addresses hygiene and grooming, feeding, elimination, activity and transfers, and safety.
Home Care
In home care, a weekly record has sections for each day and for care activities. There are sections for vital signs and weight, bathing, hygiene and grooming, activity, procedures, and nutrition. You record on the day care was given.
The Kardex or Care Summary
The Kardex is a type of card file. It summarizes information in the medical record—drugs, treatments, diagnoses, routine care measures, equipment, and special needs. The Kardex is a quick, easy source of information about the person (Fig. 7-5). It is not part of the permanent medical record.
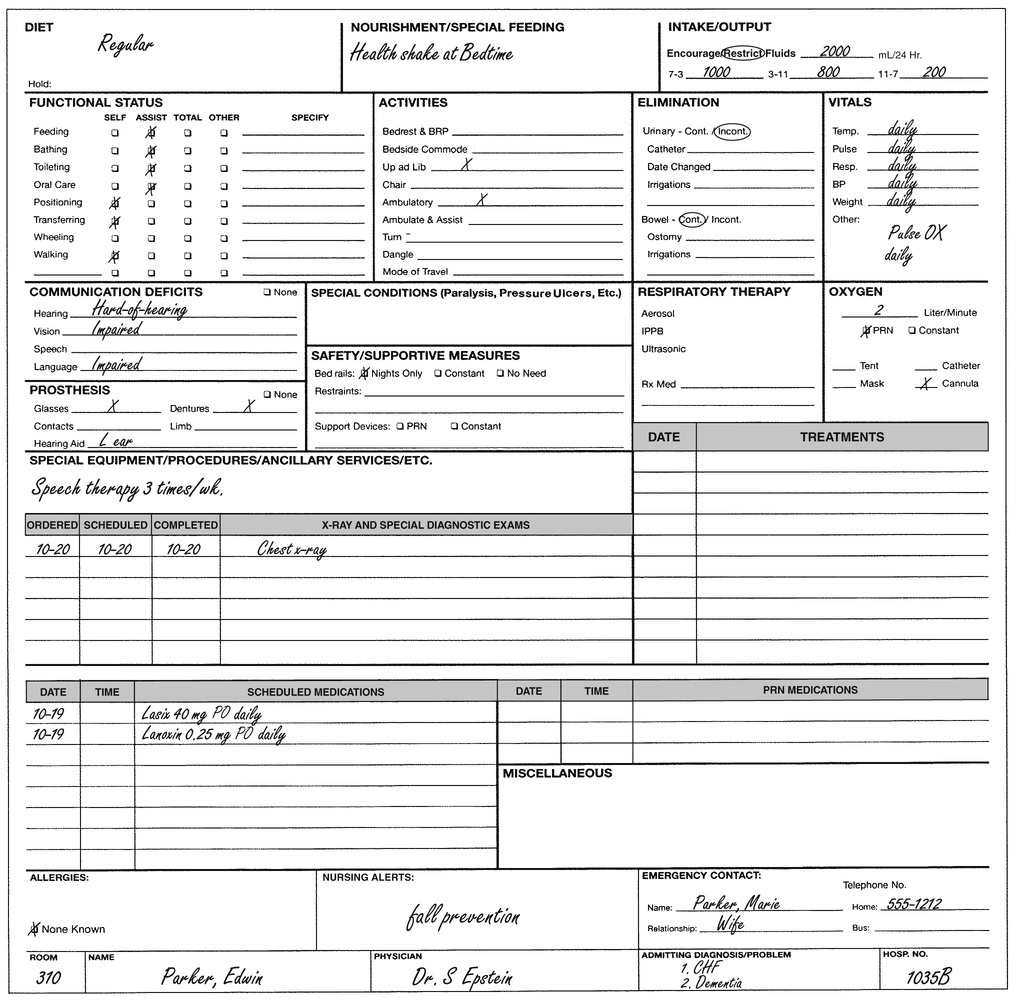
With computer systems, the person’s information is organized in an electronic care summary. Summaries can often be printed for reference.
Reporting and Recording
The health team communicates by reporting and recording. Reporting is the oral account of care and observations. Recording (charting, documentation) is the written account of care and observations.
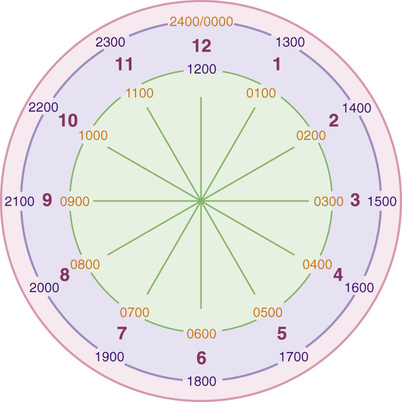
Reporting and Recording Time
The 24-hour clock (military time or international time) has 4 digits (Fig. 7-6). The first 2 digits are for the hours: 0100 = 1:00 AM; 1300 = 1:00 PM. The last 2 digits are for minutes: 0110 = 1:10 AM. Colons and AM and PM are not used. Box 7-1 shows how “conventional time” is written in “24-hour time.”
See Focus on Math: Reporting and Recording Time.
See Focus on Communication: Reporting and Recording Time.
 Focus on Math
Focus on Math
Reporting and Recording Time
A digit is any number from 0 to 9. With conventional time, 3 or 4 digits are used. With 24-hour time, 4 digits are used. To change conventional time to 24-hour time with 4 digits, do the following.
• When an AM time has 3 digits (from 1:00 AM to 9:59 AM), remove the colon and add 0 as the first digit. For example:
• When an AM or 12:00 PM time has 4 digits (10:00 AM to 12:59 PM), simply remove the colon. For example:
• For PM times, remove the colon and add 1200 to the time. For example:
• 1:00 PM becomes 1300 by adding 100 and 1200.
• 4:30 PM becomes 1630 by adding 430 and 1200.
• 10:40 PM becomes 2240 by adding 1040 and 1200.
Some agencies use 0000 for midnight. Others use 2400. For example:
Follow agency policy.
Reporting
Report care and observations to the nurse:
When reporting, follow the rules in Box 7-2, p. 74.
Box 7-2
Rules for Reporting
• Be prompt, thorough, and accurate.
• Give the person’s name and room and bed number.
• Report only what you observed and did yourself.
• Report expected changes in the person’s condition. For example, the person may be tired after lunch.
• Give reports as often as the person’s condition requires. Or give them when the nurse asks you to.
• Report at once any changes from normal or changes in the person’s condition. See Chapter 8.
• Use your written notes to give a specific, concise, and clear report (Fig. 7-7).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


