53 Care of the patient with thermal imbalance
Active Warming Measures: Include the application of forced air convective warming, circulating-water mattresses, resistive heating blankets, radiant warmers, negative-pressure warming systems, and warmed humidified oxygen.
Core Thermal Compartment: Consists of the organs of the trunk and head, which compose 50% to 60% of the body mass. Tissues are well perfused and maintain a relatively uniform temperature.
Malignant Hyperthermia: A hereditary abnormality of muscle metabolism caused by certain triggering agents and resulting in a life-threatening pharmacogenetic disorder.
Normothermia: A core temperature range of 36° to 38° C.
Passive Insulation: Warmed cotton blankets, reflective blankets, socks, head covering, and limited skin exposure.
Perioperative Hypothermia: A core body temperature less than 36° C.
Peripheral Thermal Compartment: Consists of the arms and legs. Temperature is not homogenous and varies over time.
Preventative Warming: Initiation of passive insulation or active warming measures to maintain normothermia.
Thermal Comfort: A patient’s subjective description of temperature comfort level.
Patients admitted to the postanesthesia care unit (PACU) usually have some form of thermal imbalance. Thermal imbalance is defined as body core temperature that is outside the normothermic rage of 36° to 38° C.1,2 This chapter reviews the physiology of thermoregulation, the concepts of perioperative thermoregulation and hypothermia, malignant hyperthermia, and the effect of these issues on the care of the patient in the PACU.
Overview of thermoregulation
The body maintains its temperature between the narrow range of 36° to 38° C.1–3 Although the peripheral thermal compartment (consisting of the arms and legs) temperatures can vary with environmental and thermoregulatory responses, temperature in the core body compartment is controlled within a 0.2° C range by a balance of heat production and heat loss typically regulated by thermoregulatory mechanisms in the central nervous system (CNS). These mechanisms receive input from various thermoreceptors located in the skin, nose, oral cavity, thoracic viscera, and spinal cord. These thermoreceptors send sensory information in hierarchical order: spinal cord, reticular formation, and primary control in the preoptic hypothalamic region of the brain.3–6
The central temperature controls maintain body temperature with two primary responses: physiologic and behavioral. The physiologic thermoregulatory response consists of sweating, shivering, and alterations in the peripheral vasomotor tone. These responses control the regulatory process of body temperature; consequently, heat loss is reduced with vasoconstriction and increased with vasodilation and sweating. The responses also work by reducing heat production, lowering the metabolic rate, and increasing muscle tone and shivering to enhance heat production. Behavioral thermoregulation is triggered by subjective feelings of discomfort or comfort. For example, in a hot environment, a person seeks air conditioning; in a cold environment, the person seeks heat. The response mechanism is stronger, but does not exhibit fine motor control as in the physiologic thermoregulatory response system.3,4,6
Body heat is produced by metabolism and has a circadian cycle, with the core temperature lower in the morning than in the afternoon.7 Body heat is removed with four methods of heat transfer: radiation, conduction, convection, and evaporation, all of which play a significant role in the development of perioperative hypothermia (Fig. 53-1).
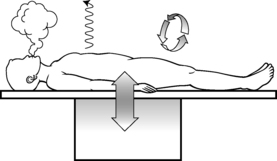
Radiation
Radiation involves the loss of energy, in this case heat, through the radiant electromagnetic waves in the infrared spectrum. It involves no direct contact between the objects involved, but simply occurs as heat radiates from a warmer object to a cooler one. Radiation heat loss accounts for 40% to 60% of all heat loss and occurs in the operating room (OR) as the uncovered skin of the surgical patient radiates energy away from the patient, resulting in a drop in body temperature. Neonates and older adults are particularly prone to heat loss via this mechanism.2–6
Conduction
Conduction involves the transfer of heat energy through direct contact between objects. Conduction loss accounts for as much as 10% of heat loss in the OR and can occur via several mechanisms, including patient contact with a cold OR table, skin preparation solutions, intravenous (IV) fluids, irrigants, and cold sheets and drapes.2–6
Convection
Convection involves the loss of body heat via transfer to the surrounding cooler air and occurs with a temperature gradient between the body and surrounding air. It accounts for 25% to 50% of heat loss in the OR. This transfer can occur in two ways. Passive movement occurs as a loss of body heat from basic skin exposure as warm air rises. Active movement, which can be facilitated by the laminar flow systems in an OR, occurs as a loss of body heat from a fan or wind blowing across the body surface.2–6
Temperature measurement
Patients have rapid core temperature changes during the perioperative period. During such periods of rapid temperature fluctuation, a core temperature measurement provides the most accurate indication of body temperature. Temperature measurement during this period must be accurate and consistent and provide a true reflection of the core temperature. The relationship between temperatures measured at various body sites during this period, however, may differ significantly from a true core reading. Consideration of the best method for obtaining a temperature must also account for accessibility of the measurement site, patient comfort and safety, and the practitioner’s ability to consistently use the device correctly.1,2,4,6,8 The same route of temperature measurement should be used throughout the perianesthesia period to allow for accurate temperature comparisons across the surgical continuum, and any extreme temperature (hypothermic or hyperthermic) detected with a noncore measurement instrument should be interpreted with caution.1
The most accurate core temperature measurement is obtained via use of a pulmonary artery (PA) catheter, because the artery bathes the catheter with blood from the core compartment and its surroundings. Temperature readings at the site can be affected by the rapid infusion of large amounts of warmed or cold IV fluids, by respiratory cycles, and by lower limb pneumatic compression devices. Readings from the distal esophagus and nasopharynx provide accurate alternatives to the PA catheter and are commonly used during surgery; however, like the PA catheter, these methods are invasive in nature and are not appropriate outside the operative setting after the patient has been extubated.2,4,6,8
Oral temperature measurement with electronic digital thermometers is a popular method of temperature measurement that is easily accessible, is less prone to operator error, and quickly reflects changes in core body temperature. Oral temperature readings vary based on placement in the oral cavity (Fig. 53-2).9 Oral temperature measurement taken in the right or left posterior sublingual (buccal) pocket provides an accurate reflection of core temperature, even in the presence of oxygen therapy, warmed and cooled inspired gases, and varied respiratory rates.1,8,10
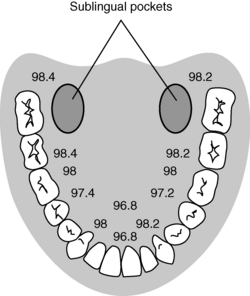
FIG. 53-2 Temperature variations in oral cavity.
(From Nicoll LH: Heat in motion: evaluating and managing temperature, Nursing 32:s12, 2002; Schick L, Windle PE, editors: Perianesthesia nursing core curriculum: preprocedure, phase I and phase II PACU nursing, ed 2, St. Louis, 2010, Saunders.)
Temporal artery thermometry is a noninvasive radiation thermometer used with a scanner probe to scan the forehead and capture the infrared heat from the arterial blood supply and record the highest temperature sensed. Current evidence supports the accuracy of temporal artery readings as a core temperature measurement at normothermic temperatures; however, the accuracy of temporal artery measures at temperature extremes has not been established.1,11–13
Infrared tympanic thermometry, previously considered a preferred method for noninvasive core temperature measurement, can be adversely affected by common sources of instrument error, including poor operator technique, patient anatomy (site), and the calibration, accuracy, and inherent instrument error of the thermometer used.8 Given the issues surrounding temperature measurement with this instrument, it is no longer recommended as an accurate means of temperature measurement during the perianesthesia period.1
Implications for practice
Consistent temperature measurement is critical to the diagnosis and subsequent management of thermoregulatory disturbances in the perianesthesia patient. Invasive core temperature measurement is preferred because it yields the most accurate temperatures; however, such methods are generally not plausible in the preoperative and postoperative periods. Noninvasive core temperature measurement methods vary in their relationship to invasive core temperature measurements. As such, nurses should use the same temperature measurement approach throughout a patient’s perianesthesia experience to establish accurate temperature trends.
Source: Fetzer SJ, Lawrence A: Tympanic membrane versus temporal artery temperatures of adult perianesthesia patients, J Perianesth Nurs 23(4):230–236, 2008.
Perioperative hypothermia
Perioperative hypothermia is defined as a core body temperature less than 36° C.1 As many as 70% of surgical patients have hypothermia in the course of the surgical experience.5 All patients undergoing general or regional anesthesia are at risk for developing unplanned perioperative hypothermia. Additional risk factors include1:
• Systolic blood pressure less than 140 mm Hg
• Length and type of surgical procedure
• Normal or below normal body mass index
• Body surface or wound area uncovered
• History of diabetes with autonomic dysfunction
Adverse effects associated with perioperative hypothermia include1,2:
The typical temperature drop associated with perioperative hypothermia is between 1° and 3° C and depends on the type and dose of anesthesia, amount of surgical exposure, and ambient room temperature. This temperature drop occurs from a loss of normal physiologic thermoregulatory mechanisms that are impaired by anesthetic drugs. As a result, the patient becomes poikilothermic and, without intervention, takes on the cooler temperature of the operative environment.3,14
Intraoperative temperature loss typically occurs in a characteristic pattern as a result of core-to-peripheral redistribution (Fig. 53-3). Redistribution occurs as a result of a reduction in the vasoconstriction threshold from the inhibitory impact of general anesthesia, resulting in a drop in core temperature, and peripheral vasodilation triggered by both general and regional anesthesia, which causes an increase in the blood flow to the skin and a resulting loss in core body heat. An initial heat loss of 1° to 1.5° C occurs during the first hour of surgery, followed by a slower more linear drop over the next 2 to 3 hours. Core temperature loss generally does not stabilize until 2 to 4 hours into the surgical procedure (Fig. 53-4). Postoperative return to normothermia occurs when the brain anesthetic concentration decreases enough to allow a normal thermoregulatory response. This response can take as long as 2 to 5 hours to occur and may be inhibited by residual anesthetics and postoperative opioids.2–4,6,14
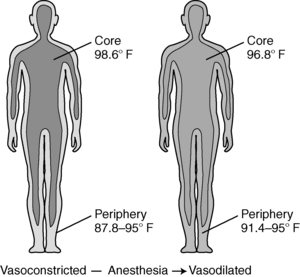
FIG. 53-3 Core-to-peripheral redistribution after administration of anesthesia.
(From Sessler DI: Perioperative heat balance, Anesthesiology 92:583, 2000. In Schick L, Windle PE, editors: Perianesthesia nursing core curriculum: preprocedure, phase I and phase II PACU nursing, ed 2, St. Louis, 2010, Saunders.)
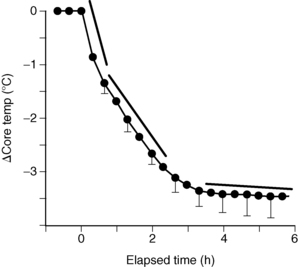
FIG. 53-4 Perioperative heat loss over time.
(From Sessler DI: Perioperative heat balance, Anesthesiology 92:583, 2000. In Schick L, Windle PE, editors: Perianesthesia nursing core curriculum: preprocedure, phase I and phase II PACU nursing, ed 2, St. Louis, 2010, Saunders.)
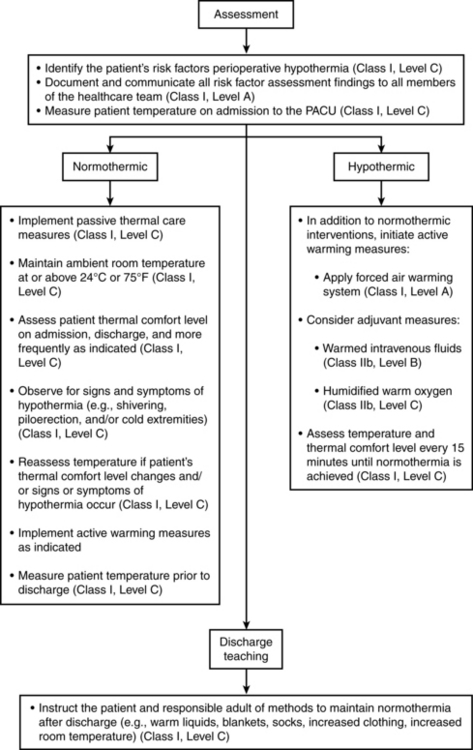
Every patient should be assessed for hypothermia on arrival in the PACU, and postoperative care should be provided per the multidisciplinary American Society of PeriAnesthesia Nurses (ASPAN) Clinical Guideline for the Maintenance of Perioperative Normothermia (Fig. 53-5).1 In the case of normothermia, preventative warming measures and passive insulation should be instituted. The ambient room temperature should be maintained at or greater than 24° C, and the patient’s thermal comfort level should be assessed at least on admission and discharge. In addition to constant observation for the signs and symptoms of hypothermia, the patient’s temperature should be reassessed when the thermal comfort level decreases, with any emerging signs or symptoms of hypothermia, and on discharge from the PACU. In addition to the previous measures, active warming should be initiated for any patient with hypothermia who is admitted. In addition, IV fluids should be warmed; all gases (oxygen) should be humidified and warmed; and temperature should be monitored at least every 15 minutes until normothermia is achieved. The expected outcomes for all patients in PACU Phase I include a return to normothermia (minimum discharge temperature of 36° C), resolution of the signs and symptoms of hypothermia, and patient verbalization of an acceptable level of warmth. Preventative warming measures and continued assessment for hypothermia should continue at whatever location to which the patient is discharged.1
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


