Cherie R. Rebar and Donna D. Ignatavicius
Care of Patients with Malnutrition and Obesity
Learning Outcomes
Safe and Effective Care Environment
Health Promotion and Maintenance
Psychosocial Integrity
Physiological Integrity
9 Interpret findings of a nutrition screening and assessment.
10 Calculate body mass index (BMI), and interpret findings.
11 Describe the risk factors for malnutrition, especially for older adults.
12 Explain why serum visceral protein levels indicate change in nutritional status.
13 Identify the role of nutritional supplements in restoring or maintaining nutrition.
14 Describe complications of total enteral nutrition (TEN).
15 Explain how to prevent complications of total parenteral nutrition (TPN).
16 Explain how to maintain enteral tube patency.
17 Describe evidence-based practices to prevent aspiration for patients with nasoenteric tubes.
18 Explain the medical complications associated with obesity.
19 Identify the role of drug therapy in the management of obesity.
20 Prioritize nursing care for patients having bariatric surgery.
21 Develop a discharge teaching plan for patients having bariatric surgery.

http://evolve.elsevier.com/Iggy/
Answer Key for NCLEX Examination Challenges and Decision-Making Challenges
Audio Glossary
Concept Map Creator
Key Points
Review Questions for the NCLEX® Examination
Carbohydrates, protein, and fat are nutrients in food that supply the body with energy. In healthy people, most of this energy undergoes digestion and is absorbed from the GI tract. Food energy is used to maintain body temperature, respiration, cardiac output, muscle function, protein synthesis, and the storage and metabolism of food sources. Therefore proper nutrition plays a major role in promoting and maintaining health.
Energy balance refers to the relationship between energy used and energy stored. Weight loss occurs when energy used is more than intake. If food intake is more than energy used, weight is gained. Body proteins are used for energy when calorie intake is insufficient. The body attempts to meet its calorie requirements even if it is at the expense of protein needs.
Nutrition Standards for Health Promotion and Maintenance
The role of nutrition in disease has been a subject of interest for many years. The current focus is on health promotion and the prevention of disease by healthy eating and exercise. In the United States, the Dietary Guidelines for Americans are revised by the U.S. Department of Agriculture (USDA) and the U.S. Department of Health and Human Services (DHHS) every 5 years. The most recent guidelines (2010) emphasize the need to include preferences of specific racial/ethnic groups, vegetarians, and other populations when selecting foods to maintain a healthful diet that is balanced with moderation and variety. If alcohol is consumed, it should be limited to one drink per day for women and two drinks for men (USDA, 2010). Examples of other guidelines are listed in Table 63-1.
TABLE 63-1
EXAMPLES OF 2010 DIETARY GUIDELINES FOR AMERICANS

Source: Dietary Guidelines for Americans Council. (2010). Retrieved March 31, 2011, from www.cnpp.usda.gov/Publications/DietaryGuidelines/2010/DGAC/Report/A-ExecSummary.pdf.
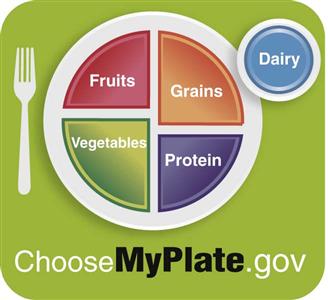
The USDA also recently designed a picture to remind people about the good foods to increase and the foods that should be reduced in the daily diet. Fig. 63-1 illustrates the USDA’s MyPlate to show that half of each meal should consist of fruits and vegetables. When grains are consumed, half of them should be whole grains rather than refined grain products.
An increasing number of people are adopting a variety of vegetarian diet patterns for health, environmental, or moral reasons. In general, vegetarians are leaner than those who consume meat. The lacto-vegetarian eats milk, cheese, and dairy foods but avoids meat, fish, poultry, and eggs. The lacto-ovo-vegetarian includes eggs in his or her diet. The vegan eats only foods of plant origin. Some people among these groups eat fish as well. Vegans can develop anemia as a result of vitamin B12 deficiency. Therefore they should include a daily source of vitamin B12 in their diets, such as a fortified breakfast cereal, fortified soy beverage, or meat substitute. All vegetarians should ensure that they get adequate amounts of calcium, iron, zinc, and vitamins D and B12. Well-planned vegetarian diets can provide adequate nutrition. The National Agriculture Library (2008) publishes a Vegetarian Nutrition Resource List that provides credible resources regarding vegetarian health.
 Cultural Awareness
Cultural Awareness
Many people have specific food preferences based on their ethnicity or race. For example, for people of Hispanic descent, tortillas, beans, and rice may be desired over pasta, risotto, and potatoes. Never assume that a person’s racial or ethnic background means that he or she eats only foods associated with his or her primary ethnicity. Health teaching about nutrition should incorporate any cultural preferences (also see Chapter 4).
Some people have food allergies or intolerances. For instance, lactose intolerance (lactose is found in milk and milk products) is a common problem that occurs in a number of ethnic groups. It is found more often in Mexican Americans and black people as well as in some American Indian groups, Asian Americans, and Ashkenazi Jews. A small percentage of white people, particularly those of Mediterranean descent (e.g., Greek, Italian), are also lactose intolerant. The cause of lactose intolerance is an inadequate amount of the lactase enzyme, which converts lactose into absorbable glucose. Patients may benefit from learning more about the management of lactose intolerance from resources provided by organizations such as the American Dietetic Association.
One of the most recent publications from Health Canada on nutrition is the Canada Food Guide. Compared with previous documents, it includes more culturally diverse foods, information on trans fats, customized individual recommendations, and exercise guidelines. Several booklets can be purchased to help people select the best foods and nutrients from the new Guide, such as Eating Well with Canada’s Food Guide. In addition, Canada has published a separate booklet to address the special needs of some of its indigenous people. The Eating Well with Canada’s Food Guide—First Nations, Inuit, and Métis includes berries, wild plants, and wild game to reflect the values and traditions for aboriginal people living in Canada (Health Canada, 2007).
Nutritional Assessment
Malnutrition (also called undernutrition) and obesity are common nutritional health problems. These problems lead to deficits that cause many comorbidities and complications, including death.
Nutritional status reflects the balance between nutrient requirements and intake. Common factors that affect these requirements include age, gender, disease, infection, and psychological stress. Nutrient intake is influenced by eating behavior, economic factors, emotional stability, disease, drug therapy, and cultural factors.
Evaluation of nutritional status is an important part of total patient assessment and includes:
• Review of the nutritional history
• Food and fluid intake record
• Health history and physical assessment
Monitor the nutritional status of a patient during hospitalization as an important part of your initial assessment. Collaborate with the interdisciplinary health care team to identify patients at risk for nutritional problems.
Initial Nutritional Screening
Not every patient needs a complete nutritional assessment, but it is important to identify those at risk for problems through screening. An initial screening provides an inexpensive, quick way of determining which patients need more extensive nutritional assessment by the health care team. The Joint Commission Patient Care Standards require that a nutritional screening occur within 24 hours of the patient’s hospital admission. If indicated, an in-depth nutritional assessment should be performed. When patients are in the hospital more than a week, nutritional assessment should be part of the daily plan of care.
The initial nutritional screening includes inspection, measured height and weight, weight history, usual eating habits, ability to chew and swallow, and any recent changes in appetite or food intake. Examples of questions that help identify patients at risk for nutritional problems are part of the history and physical assessment (Chart 63-1).
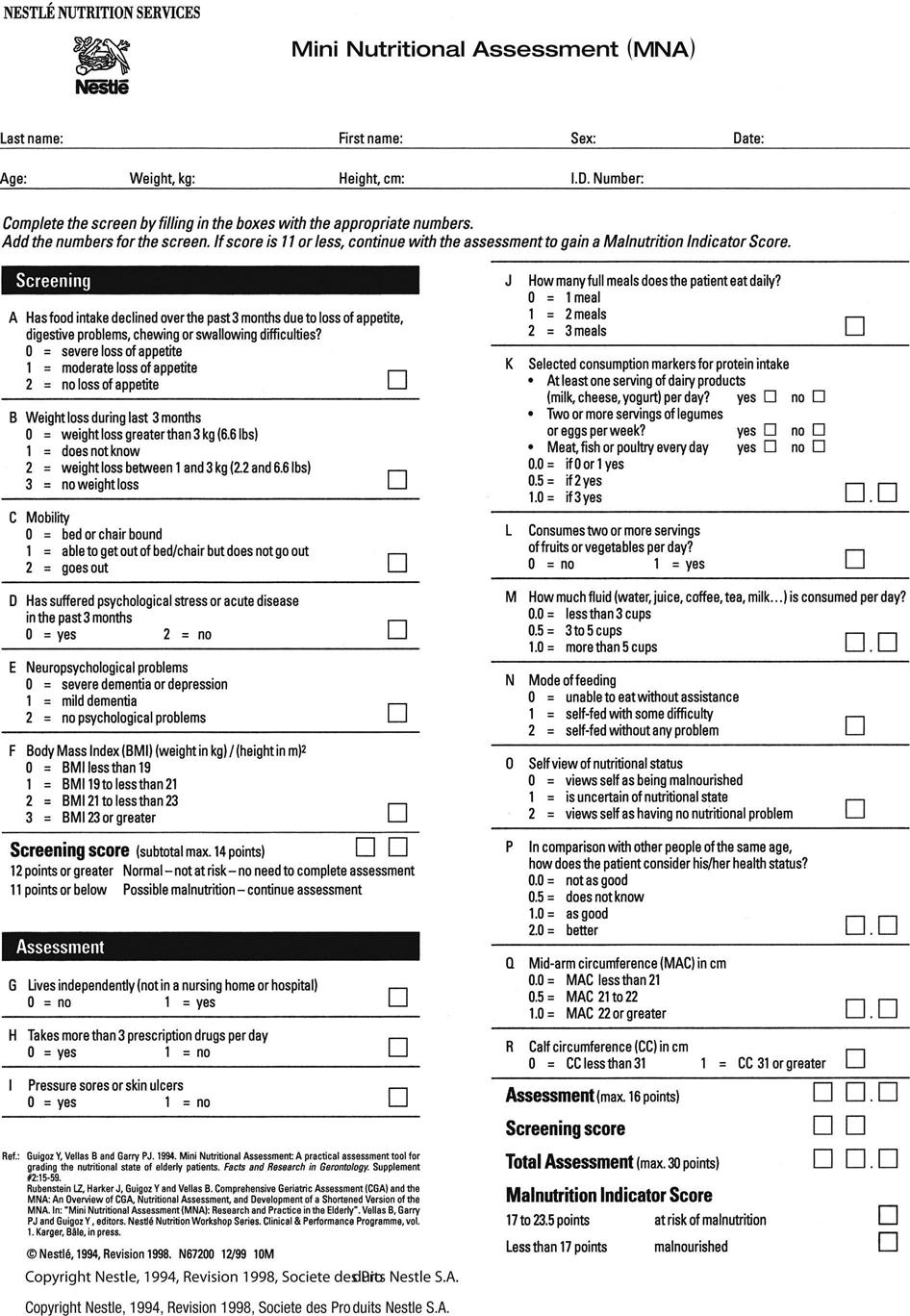
The Mini Nutritional Assessment (MNA), a two-part tool that has been tested worldwide, provides a reliable, rapid assessment for patients in the community and in any health care setting. The first part (A-F) is a screening section that takes 3 minutes to complete and asks about food intake, mobility, and body mass index (BMI) (described on p. 1339). It also screens for weight loss, acute illness, and psychological health problems. If the patient scores 11 points or less, the second part (G-R) of the MNA is completed, for an additional 12 questions. The entire assessment takes less than 15 minutes (Fig. 63-2) (DiMaria-Ghalili & Guenter, 2008). A new MNA® Short Form can be used as a stand-alone tool to evaluate whether the older patient is well-nourished, at risk for malnutrition, or malnourished. The alternative is to take the patient’s calf circumference, which can be a reliable alternative if BMI is unavailable.
Anthropometric Measurements
Anthropometric measurements are noninvasive methods of evaluating nutritional status. These measurements include height and weight and assessment of body fat.
Obtain a current height and weight to provide a baseline. Be sure to obtain accurate measurements because patients tend to overestimate height and underestimate weight. Measurements taken days or weeks later may indicate an early change in nutritional status. You may delegate this activity to unlicensed assistive personnel (UAP) under your supervision.
Patients should be measured and weighed while wearing minimal clothing and no shoes. Determine the height in inches or centimeters using the measuring stick of a weight scale if the patient can stand. He or she should stand erect and look straight ahead, with the heels together and the arms at the sides. For patients who cannot stand or those who cannot stand erect (e.g., some older adults), use a sliding-blade knee height caliper, if available. This device uses the distance between the patient’s patella and heel to estimate height. It is especially useful for patients who have knee or hip contractures.
UAP weigh ambulatory patients with an upright balance-beam scale. Non-ambulatory patients can be weighed with a movable wheelchair balance-beam scale or a bed scale.
 Nursing Safety Priority
Nursing Safety Priority
Action Alert
Be sure that the manufacturer calibrates weight scales twice yearly for accurate readings. For daily or sequential weights, obtain the weight at the same time each day, if possible, preferably before breakfast. Conditions such as congestive heart failure and renal disease cause weight gain; dehydration and conditions such as cancer cause weight loss. Weight is the most reliable indicator of fluid gain or loss, so accurate weights are essential!
Normal weights for adult men and women are available from several reference standards, including the revised Metropolitan Life tables. Some health care professionals prefer these tables because they consider body-build differences by gender and body frame size.
Changes in body weight can be expressed by three different formulas:
1 Weight as a percentage of ideal body weight (IBW):

2 Current weight as a percentage of usual body weight (UBW):


An unintentional weight loss of 10% over a 6-month period at any time significantly affects nutritional status and should be evaluated. Depending on the patient’s needs, weights may need to be taken daily, several times a week, or weekly for monitoring status and the effectiveness of nutritional support.
In the health care setting, assessment of body fat is usually calculated by the dietitian. For people who participate in a structured exercise program in the community, this assessment is typically performed by a fitness trainer or physical therapist.
The body mass index (BMI) is a measure of nutritional status that does not depend on frame size. It indirectly estimates total fat stores within the body by the relationship of weight to height. Therefore an accurate height is as important as an accurate weight.
A simple calculation for estimating BMI can be programmed into handheld computers or calculators using one of these two formulas:
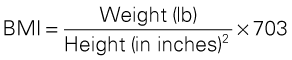
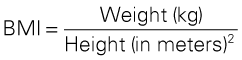
BMI can also be determined using a table that is linked with height and weight. The least risk for malnutrition is associated with scores between 18.5 and 25. BMIs above and below these values are associated with increased health risks (Centers for Disease Control and Prevention [CDC], 2009).
 NCLEX examination challenge
NCLEX examination challenge
Health Promotion and Maintenance
An older adult is admitted to the hospital with pressure ulcers and septicemia. His height is 5 feet, 10 inches (1.78 meters), and he weighs 342 pounds (155 kg). His current body mass index (BMI) is _______. (Your answer should be rounded to the nearest tenth.)
Skinfold measurements estimate body fat and can be measured by either the nurse or the dietitian. The triceps and subscapular skinfolds are most commonly measured using a special caliper. Both are compared with standard measurements and recorded as percentiles.
The midarm circumference (MAC) and calf circumference (CC) can be obtained to measure muscle mass and subcutaneous fat. These measurements are needed if the Mini Nutritional Assessment tool is used. To measure MAC, place a flexible tape around the upper arm at the midpoint, taking care to hold the tape firmly but gently to avoid compressing the tissue. This measurement is usually recorded in centimeters. The midarm muscle mass (MAMM) measures the amount of muscle in the body and is a sensitive indicator of protein reserves. It can be computed from the MAC and the triceps skinfold measure. The CC is obtained using a similar procedure on the calf.
Malnutrition
Pathophysiology
Protein-energy malnutrition (PEM), also known as protein-calorie malnutrition (PCM), may present in three forms: marasmus, kwashiorkor, and marasmic-kwashiorkor. Marasmus is generally a calorie malnutrition in which body fat and protein are wasted. Serum proteins are often preserved. Kwashiorkor is a lack of protein quantity and quality in the presence of adequate calories. Body weight is more normal, and serum proteins are low. Marasmic-kwashiorkor is a combined protein and energy malnutrition. This problem often presents clinically when metabolic stress is imposed on a chronically starved patient. The outcome of unrecognized or untreated PEM is often dysfunction or disability and increased morbidity and mortality.
Malnutrition (also called undernutrition) is a multinutrient problem because foods that are good sources of calories and protein are also good sources of other nutrients. In the malnourished patient, protein catabolism exceeds protein intake and synthesis, resulting in negative nitrogen balance, weight loss, decreased muscle mass, and weakness.
The function of the liver, heart, lungs, GI tract, and immune system decreases in the patient with malnutrition. A decrease in serum proteins (hypoproteinemia) occurs as protein synthesis in the liver decreases. Vital capacity is also reduced as a result of respiratory muscle atrophy. Cardiac output diminishes. Malabsorption occurs because of atrophy of GI mucosa and the loss of intestinal villi.
Other common complications of severe malnutrition in adults include:
• Leanness and cachexia (muscle wasting with prolonged malnutrition)
• Decreased activity tolerance
• Lethargy
• Edema
• Dry, flaking skin and various types of dermatitis
• Infection, particularly postoperative infection and sepsis
Malnutrition results from inadequate nutrient intake, increased nutrient losses, and increased nutrient requirements. Inadequate nutrient intake can be linked to poverty, lack of education, substance abuse, decreased appetite, and a decline in functional ability to eat independently, particularly in older adults. Infectious diseases, such as tuberculosis and human immune deficiency virus (HIV) infection, can also cause PEM. Diseases that produce diarrhea and infections leading to anorexia result in negative calorie and protein balance. Anorexia then leads to poor food intake. Vomiting causes decreased intestinal absorption with increased nutrient losses. Medical treatments such as chemotherapy can also cause malnutrition. In addition, catabolic processes, such as that caused by prolonged immobility, increase nutrient requirements and metabolic losses.
Inadequate nutrient intake can result also when a person is admitted to the hospital or long-term care facility. For example, decreased staffing may not allow time for patients who need to be fed, especially older adults, who may eat slowly. Many diagnostic tests, surgery, trauma, and unexpected medical complications require a period of NPO or cause anorexia (loss of appetite).
 Cultural Awareness
Cultural Awareness
In some cases, malnutrition results when the provided meals are different from what the patient usually eats. Be sure to identify specific food preferences that the patient can eat and enjoy that are in keeping with his or her cultural practices.
Acute PEM may develop in patients who were adequately nourished before hospitalization but experience starvation while in a catabolic state from infection, stress, or injury. Chronic PEM can occur in those who have cancer, end-stage kidney or liver disease, or chronic neurologic disease.
Eating disorders, such as anorexia nervosa and bulimia nervosa seen most often in teens and young adults, also lead to malnutrition. Anorexia nervosa is a self-induced starvation resulting from a fear of fatness, even though the patient is underweight. Bulimia nervosa is characterized by episodes of binge eating in which the patient ingests a large amount of food in a short time. The binge eating is followed by some form of purging behavior, such as self-induced vomiting or excessive use of laxatives and diuretics. If not treated, death can result from starvation, infection, or suicide. Information about eating disorders can be found in textbooks on mental/behavioral health nursing.
Patient-Centered Collaborative Care
Assessment
History
Review the medical history to determine the possibility of increased metabolic needs or nutritional losses, chronic disease, trauma, recent surgery of the GI tract, drug and alcohol abuse, and recent significant weight loss. Each of these conditions can contribute to malnutrition. For older adults, explore mental status changes and note poor eyesight, diseases affecting major organs, constipation or incontinence, and slowed reactions. Review prescription and over-the-counter (OTC) drugs, including vitamin, mineral, herbal, and other nutritional supplements.
For patients who live independently in the community, the nurse may assess their performance of instrumental activities of daily living (IADLs). Functional status can best be evaluated for institutionalized patients by assessing their ADL performance. Poor nutrition is a major contributing factor to decreased functional ability.
In collaboration with the dietitian, obtain information about the patient’s usual daily food intake, eating behaviors, change in appetite, and recent weight changes. If the patient is able to communicate, ask him or her to describe the usual foods eaten daily, cultural food preferences, and the times of meals and snacks. If available, ask the family these questions if the patient cannot communicate. If the patient cannot understand the questions due to language differences, locate an interpreter to assist with communication. The dietitian can more thoroughly analyze the diet, if necessary, based on your initial nutritional screening.
Ask about changes in eating habits as a result of illness, and document any change in appetite, taste, and weight loss. A weight loss of 5% or more in 30 days, a weight loss of 10% in 6 months, or a weight that is below ideal may indicate malnutrition.
 Nursing Safety Priority
Nursing Safety Priority
Action Alert
When assessing for malnutrition, assess for difficulty or pain in chewing or swallowing. Unrecognized dysphagia is a common problem among nursing home residents and can cause malnutrition, dehydration, and aspiration pneumonia. Ask the patient whether any foods are avoided and why. Ask UAP to report any choking while the patient eats. Record the occurrence of nausea, vomiting, heartburn, or any other symptoms of discomfort with eating.
Ask the patient about dental health problems, including the presence of dentures. Dentures or partial plates that do not fit well interfere with food intake. Dental caries (decay) or missing teeth may also cause discomfort while eating.
Physical Assessment/Clinical Manifestations
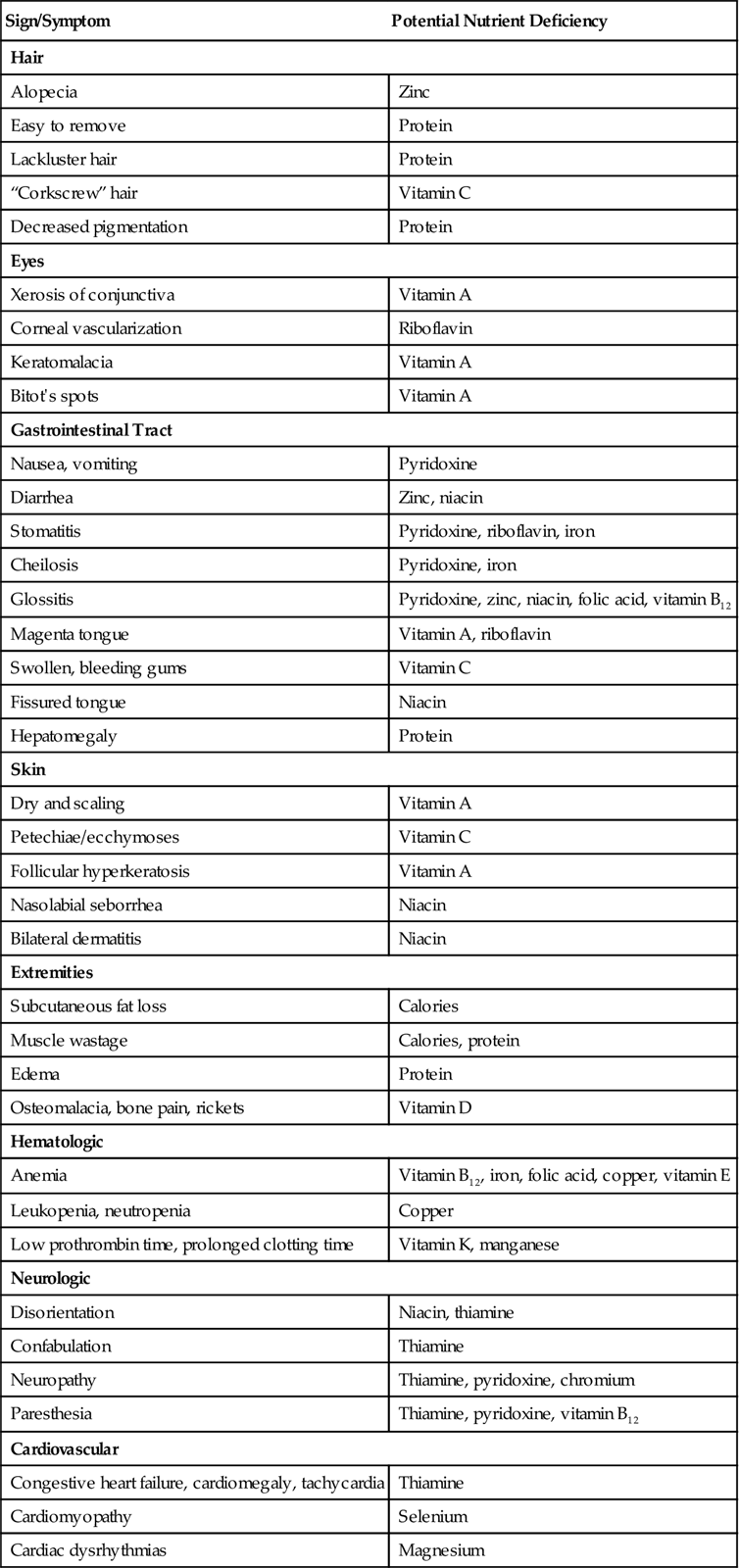
Assess for manifestations of various nutrient deficiencies (Table 63-2). Inspect the patient’s hair, eyes, oral cavity, nails, and musculoskeletal and neurologic systems. Examine the condition of the skin, including any reddened or open areas. The previously described anthropometric measurements may also be obtained. The nurse or UAP should monitor all food and fluid intake and note any mouth pain or difficulty in chewing or swallowing. A 3-day caloric intake may be collected and then calculated by the dietitian.
TABLE 63-2
MANIFESTATIONS OF NUTRIENT DEFICIENCIES
| Sign/Symptom | Potential Nutrient Deficiency |
| Hair | |
| Alopecia | Zinc |
| Easy to remove | Protein |
| Lackluster hair | Protein |
| “Corkscrew” hair | Vitamin C |
| Decreased pigmentation | Protein |
| Eyes | |
| Xerosis of conjunctiva | Vitamin A |
| Corneal vascularization | Riboflavin |
| Keratomalacia | Vitamin A |
| Bitot’s spots | Vitamin A |
| Gastrointestinal Tract | |
| Nausea, vomiting | Pyridoxine |
| Diarrhea | Zinc, niacin |
| Stomatitis | Pyridoxine, riboflavin, iron |
| Cheilosis | Pyridoxine, iron |
| Glossitis | Pyridoxine, zinc, niacin, folic acid, vitamin B12 |
| Magenta tongue | Vitamin A, riboflavin |
| Swollen, bleeding gums | Vitamin C |
| Fissured tongue | Niacin |
| Hepatomegaly | Protein |
| Skin | |
| Dry and scaling | Vitamin A |
| Petechiae/ecchymoses | Vitamin C |
| Follicular hyperkeratosis | Vitamin A |
| Nasolabial seborrhea | Niacin |
| Bilateral dermatitis | Niacin |
| Extremities | |
| Subcutaneous fat loss | Calories |
| Muscle wastage | Calories, protein |
| Edema | Protein |
| Osteomalacia, bone pain, rickets | Vitamin D |
| Hematologic | |
| Anemia | Vitamin B12, iron, folic acid, copper, vitamin E |
| Leukopenia, neutropenia | Copper |
| Low prothrombin time, prolonged clotting time | Vitamin K, manganese |
| Neurologic | |
| Disorientation | Niacin, thiamine |
| Confabulation | Thiamine |
| Neuropathy | Thiamine, pyridoxine, chromium |
| Paresthesia | Thiamine, pyridoxine, vitamin B12 |
| Cardiovascular | |
| Congestive heart failure, cardiomegaly, tachycardia | Thiamine |
| Cardiomyopathy | Selenium |
| Cardiac dysrhythmias | Magnesium |
Courtesy of Ross Products Division, Abbott Laboratories, Columbus, OH.
Psychosocial Assessment
The psychosocial history provides information about the patient’s economic status, occupation, educational level, gender orientation, ethnicity/race, living and cooking arrangements, and mental status. Determine whether financial resources are adequate for providing the necessary food. If resources are inadequate, the social worker or case manager may refer the patient and family to available community services. Chapter 3 discusses nutrition in older adults in more detail.
Laboratory Assessment
Laboratory tests supply objective data that can support subjective data and identify preclinical deficiencies. However, they must be carefully interpreted with regard to the total patient; an isolated value may yield an inaccurate conclusion.
A low hemoglobin level may indicate anemia, recent hemorrhage, or hemodilution caused by fluid retention. Hemoglobin may also be low secondary to conditions such as low serum albumin, infection, catabolism, or chronic disease. High levels may indicate hemoconcentration or dehydration, or they may be secondary to liver disease.
Low hematocrit levels may reflect anemia, hemorrhage, excessive fluid, renal disease, or cirrhosis. High hematocrit levels may indicate dehydration or hemoconcentration.
Serum albumin, thyroxine-binding prealbumin, and transferrin are measures of visceral proteins. Serum albumin is a plasma protein that reflects the nutritional status of the patient a few weeks before testing and is therefore not the most sensitive test. In addition, patients who are dehydrated often have high levels of albumin and those with fluid excess have a lowered value. The normal serum albumin level for men and women is 3.5 to 5.0 g/dL or 35 to 50 g/L (SI units) (Pagana & Pagana, 2010).
Thyroxine-binding prealbumin (PAB) is a plasma protein that provides a more sensitive indicator of nutritional deficiency because of its short half-life of 2 days. Depending on the laboratory test used, the normal PAB range is 15 to 36 mg/dL or 150 to 360 mg/L (SI units) (Pagana & Pagana, 2010). PAB can also assess improvement in nutritional status with refeeding; levels can increase by 1 mg/dL daily with adequate nutritional support.
Although not used as commonly, serum transferrin, an iron-transport protein, can be measured directly or calculated as an indirect measurement of total iron-binding capacity (TIBC). It has a short half-life of 8 to 10 days and therefore is also a more sensitive indicator of protein status than albumin.
Cholesterol levels normally range between 160 and 200 mg/dL in adult men and women. Values are typically low with malabsorption, liver disease, pernicious anemia, end-stage cancer, or sepsis. A cholesterol level below 160 mg/dL has been identified as a possible indicator of malnutrition. Cholesterol testing is discussed in more detail in Chapter 35.
Total lymphocyte count (TLC) can be used to assess immune function. Malnutrition suppresses the immune system and leaves the patient more likely to get an infection. When a patient is malnourished, the TLC is usually decreased to below 1500/mm3.
Analysis
The priority problem for the patient with malnutrition is:
Planning and Implementation
Improving Nutrition
Planning: Expected Outcomes.
The patient with malnutrition is expected to have nutrients available to meet his or her metabolic needs as evidenced by normal serum proteins and adequate hydration.
Interventions.
The preferred route for nutritional intake is through the GI tract because it enhances the immune system and is safer, easier, less expensive, and more enjoyable.
Nutrition Management.
The dietitian calculates the nutrients required daily and plans the patient’s diet. In collaboration with the health care provider and dietitian, provide high-calorie, nutrient-rich foods (e.g., milkshakes, cheese, supplement drinks like Boost or Ensure). Assess the patient’s food likes and dislikes. A feeding schedule of six small meals may be tolerated better than three large ones. A pureed or dental soft diet may be easier for those who have problems chewing or are edentulous (toothless).
 Nursing Safety Priority
Nursing Safety Priority
Action Alert
Malnourished ill patients often need to be encouraged to eat. Instruct UAP who are feeding patients to keep food at the appropriate temperature and to provide mouth care before feeding. Assess for other needs, such as pain management, and provide interventions to make the patient comfortable. Pain can prevent patients from enjoying their meals. Remove bedpans, urinals, and emesis basins from sight. Provide a quiet environment, which is conducive to eating. Soft music may calm those with advanced dementia or delirium. Appropriate time should be taken so that the patient does not feel rushed through a meal.
Considerations for Older Adults
Some patients, especially older adults, may take a long time to eat even small quantities of food because they tend to be less hungry than younger adults. If available, suggest that family members bring in favorite or ethnic foods that the patient might be more likely to eat. Teach them about ways to encourage the patient to increase food intake. Chart 63-3 describes additional interventions to promote nutritional intake in older adults.
Chart 63-3
Nursing Focus on the Older Adult
Promoting Nutritional Intake
• Be sure patient is toileted and receives mouth care before mealtime.
• Make sure that patient has glasses and hearing aids in place, if appropriate, during meals.
• Be sure that bedpans, urinals, and emesis basins are removed from sight.
• Give analgesics to control pain and/or antiemetics for nausea at least 1 hour before mealtime.
• Remind unlicensed assistive personnel (UAP) to have patient sit in chair, if possible, at mealtime.
• If needed, open cartons and packages and cut up food at the patient’s and/or family’s request.
• Observe the patient during meals for food intake.
• Ask the patient about food likes and dislikes and ethnic food preferences.
• Encourage self-feeding, or feed the patient slowly; delegate this activity to UAP if desired.
• If feeding patient, sit at eye-level if culturally appropriate.
• Create an environment that is conducive to eating and socialization and relaxation, if possible.
• Decrease distractions, such as environmental noise from television, music, or other people.
• Provide adequate, nonglaring lighting.
• Keep patient away from offensive or medicinal odors.
• Keep eye contact with the patient during the meal if culturally appropriate.
• Do not interrupt patients during mealtimes for nonurgent procedures or rounds.
• Assess for need for supplements between meals and at bedtime.
• If the patient is depressed, be sure that the depression is treated by the health care provider.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


