James G. Sampson and M. Linda Workman
Care of Patients with HIV Disease and Other Immune Deficiencies
Learning Outcomes
Safe and Effective Care Environment
Health Promotion and Maintenance
Psychosocial Integrity
Physiological Integrity
9 Compare primary and secondary immune deficiencies for cause and onset of problems.
12 Describe the ways in which HIV is transmitted.
13 Coordinate nursing care for the patient with AIDS who has impaired gas exchange.

http://evolve.elsevier.com/Iggy/
Answer Key for NCLEX Examination Challenges and Decision-Making Challenges
Audio Glossary
Concept Map Creator
Key Points
Review Questions for the NCLEX® Examination
Immune system function is concerned with helping the body stay healthy by preventing the growth of infectious organisms and abnormal cells, such as cancer cells. It assists the body to monitor and maintain those cells and substances that are considered “self,” belonging to the body. For example, newly made cells and compatible blood transfusions are deemed self and safe by the immune system. However, when the immune system detects the presence of a protein or cell that does not belong to the body and represents a potential threat, its job is then to attack and destroy the “non-self” or “foreign” substance. Infection is a major threat. We are exposed to many organisms every day. The efficiency of the immune system prevents disease despite this exposure.
When the immune system fails to recognize infectious agents, severe local and systemic infections are not suppressed or controlled. Immune system failure can be the result of a primary (congenital) immune deficiency in which one or more parts of the system are not functioning properly from birth. These problems are usually genetic mutations that are discovered in the infant or child who is repeatedly sick. Immune system failure can also be secondary (acquired after birth) as the result of viral infection, contact with a toxin, or medical therapy. These problems can cause a normal immune system to stop functioning or to function less efficiently. In either case, the immune system can no longer distinguish what should be in the body from a foreign invader. The consequences for the immune-deficient patient can range from mild, localized health problems to total immune system failure, leaving the body open to attack from any foreign pathogen.
Acquired (Secondary) Immune Deficiencies
HIV InFection and AIDS
Pathophysiology
Human immune deficiency virus (HIV) infection can progress to acquired immune deficiency syndrome (AIDS), which is the most common secondary immune deficiency disease in the world (World Health Organization [WHO], 2010). First identified in 1981, HIV/AIDS is now a serious worldwide epidemic.
Etiology and Genetic Risk
The cause of HIV infection is a virus—the human immune deficiency virus. Like most viruses, HIV is a parasite looking for a way into a cell, to take over the cell, and to force the cell into making more copies of the virus. These new virus particles then look for additional cells to infect, repeating the cycle as long as there are new host cells to infect.
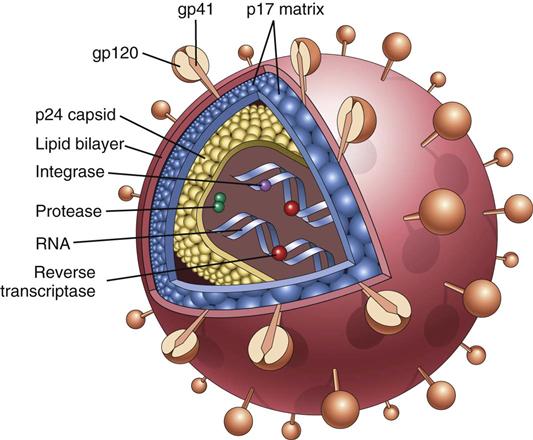
The HIV Infectious Process.
Viral particle features include an outer envelope with special “docking proteins,” known as gp41 and gp120, that assist in finding a host (Fig. 21-1). Inside, the virus has two protein coatings and the genetic material along with the enzymes reverse transcriptase (RT) and integrase. The first challenge is for the HIV particle to get inside a host cell. HIV accomplishes this task by first finding a way into the host’s bloodstream. Once in the blood, HIV “hijacks” certain cells. One of the cells that it hijacks is the CD4 T-cell, also known as the CD4 cell, helper/inducer T-cell, or T4-cell (Kaufman, 2011) (see Chapter 19). This cell directs immune system defenses and regulates the activity of all immune system cells. If HIV successfully enters a CD4 T-cell, it can then create more virus particles.
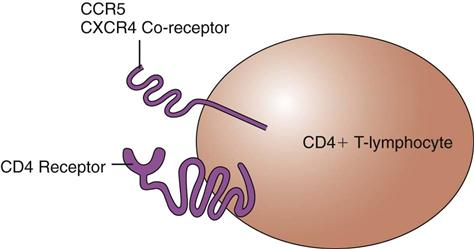
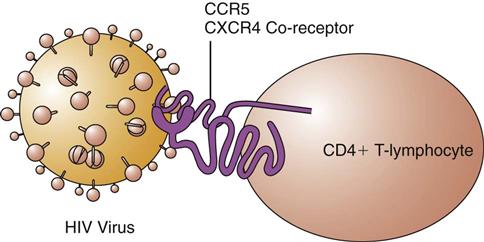
Virus-host interactions are needed for disease development. When a person is infected with HIV, the virus randomly “bumps” into many cells. The docking proteins on the outside of the virus try to find special receptors on a host cell that will allow the virus to bind and then enter the cell. The CD4+ T-cell has receptors on its surface known as CD4, CCR5, and CXCR4 (Fig. 21-2). Proteins on the HIV particle surface, known as gp120 and gp41, recognize these receptors on the CD4+ T-cell. For the virus to enter this cell, both the gp120 and the gp41 must bind to the receptors. The gp120 first binds to the primary CD4 receptor, which changes its shape and allows the gp41 to bind to one of the co-receptors (either the CCR5 receptor or the CXCR4 receptor). This attachment allows the virus to then enter the CD4+ T-cell (Fig. 21-3). Viral binding to the CD4 receptor and to either of the co-receptors is needed to enter the cell. (The new drug class known as entry inhibitors works here to block the receptor and prevent the interaction needed for entry of HIV into the CD4+ T-cell.)
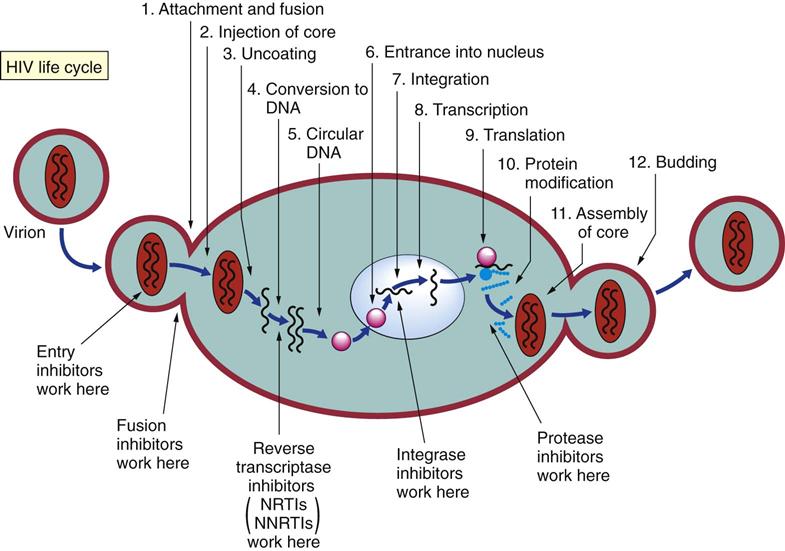
Viruses, like human cells, have genetic material. After entering a host cell, HIV must get its genetic material into the host cell’s DNA. HIV belongs to a family of viruses called retroviruses. The genetic material of the human cell is double-stranded DNA (ds-DNA). The genetic material of HIV is single-stranded ribonucleic acid (RNA) (ss-RNA). To infect and take over a human cell, the genetic material must be the same. HIV overcomes this problem by bringing along an enzyme at the time of infection, reverse transcriptase (RT). RT takes HIV’s ss-RNA and converts it into ds-DNA, which makes the viral genetic material the same as human DNA. (The drug classes known as nucleoside analog reverse transcriptase inhibitors [NRTIs] and non-nucleoside reverse transcriptase inhibitors [NNRTIs] work here to inhibit HIV reverse transcriptase.) Then HIV must get its DNA into the nucleus of the CD4+ T-cell and place it within the human DNA. HIV also brings an enzyme called integrase. This enzyme allows the viral ds-DNA to be inserted into the host ds-DNA, which completes the infection of the CD4+ T-cell. (The drug class known as integrase inhibitors works here to prevent viral DNA from integrating into the cell’s normal human DNA.)
HIV particles are made within the infected CD4+ T-cell, using all the metabolic machinery of the host. The new virus particle is made in the form of one long protein strand. The strand is clipped, using chemical enzyme scissors called HIV protease, into several small functional pieces. These pieces are formed into a new finished viral particle. (The drug class known as protease inhibitors works here to inhibit HIV protease.) Once the new virus particle is finished, it fuses with the infected cell’s membrane and then buds off in search of another CD4+ T-cell to infect (Fig. 21-4).
Effects of HIV infection are related to the new genetic instructions that now direct CD4+ T-cells to change their role in immune system defenses. The new role is to be an “HIV factory.” The immune system is made weaker by removing some CD4+ T-cells from circulation, and the most important cell in the immune system becomes an HIV factory. Up to 10 billion virus particles are made daily. In early HIV infection, the immune system can still attack and destroy most of the newly created virus particles. With time, however, the number of HIV particles overwhelms the immune system. Gradually, CD4+ T-cell counts fall, viral numbers (viral load) rise, and without treatment, the patient eventually dies of opportunistic infections or cancer.
Everyone who has AIDS has HIV infection; however, not everyone who has HIV infection has AIDS. The distinction rests with the number of CD4+ T-cells the patient has and whether any opportunistic infections have occurred. A healthy adult usually has at least 800 to 1000 of these cells per cubic millimeter (mm3) of blood. The number of CD4+ T-cells is reduced in the person with HIV disease.
About 50% to 90% of people who are first infected with HIV develop an acute infection within 4 weeks. Manifestations of this acute HIV infection can be fever, night sweats, chills, headache, and muscle aches. All of these problems can be caused by exposure to almost any virus (e.g., influenza)—not just to HIV. Many people with this acute HIV infection also have a rash and a sore throat, which is often confused with mononucleosis and viral meningitis. With time, these symptoms cease and the person feels well again. Actually, a “war is going on” in the body between HIV and the immune system.
As time passes, with more CD4+ T-cells infected and taken out of service, this cell count drops to below normal levels and those that remain may not function normally. Poor CD4+ T-cell function as a result of HIV infection leads to these immune system abnormalities:
• Lymphocytopenia (decreased numbers of lymphocytes)
• Increased production of incomplete and nonfunctional antibodies
As the CD4+ T-cell level drops, the patient is at risk for bacterial, fungal, and viral infections, as well as opportunistic cancers. Opportunistic infections are those caused by organisms that are present as part of the body’s normal environment and are kept in check by normal immune function. They occur because of the profound immunosuppression in the person with AIDS. These infections may result from a newly acquired infection or reactivation of an old infection.
A diagnosis of AIDS requires that the person be HIV positive and have either a CD4+ T-cell count of less than 200 cells/mm3 or an opportunistic infection. Once AIDS is diagnosed, even if the patient’s cell count goes higher than 200 cells/mm3 or the infection is successfully treated, the AIDS diagnosis remains and the patient never reverts to being just HIV positive.
HIV Classification.
The Centers for Disease Control and Prevention (CDC), in a 1993 definition, classified HIV infection by correlating clinical conditions with three ranges of CD4+ T-cell counts. This classification was replaced in 2008 by defining four stages of the disease. In this new definition, laboratory confirmation of HIV infection (by enzyme-linked immunosorbent assay [ELISA] and Western blot analysis) plus CD4+ T-lymphocyte count or percentage and the presence or absence of the 26 AIDS-defining conditions (Table 21-1) determine the classification (CDC, 2008). The person with HIV infection can transmit the virus to others at all stages of disease, but the recently infected person with a high viral load and those at end stage without drug therapy can be particularly infectious.
TABLE 21-1
CENTERS FOR DISEASE CONTROL AND PREVENTION CLASSIFICATION OF AIDS-DEFINING CONDITIONS IN ADULTS
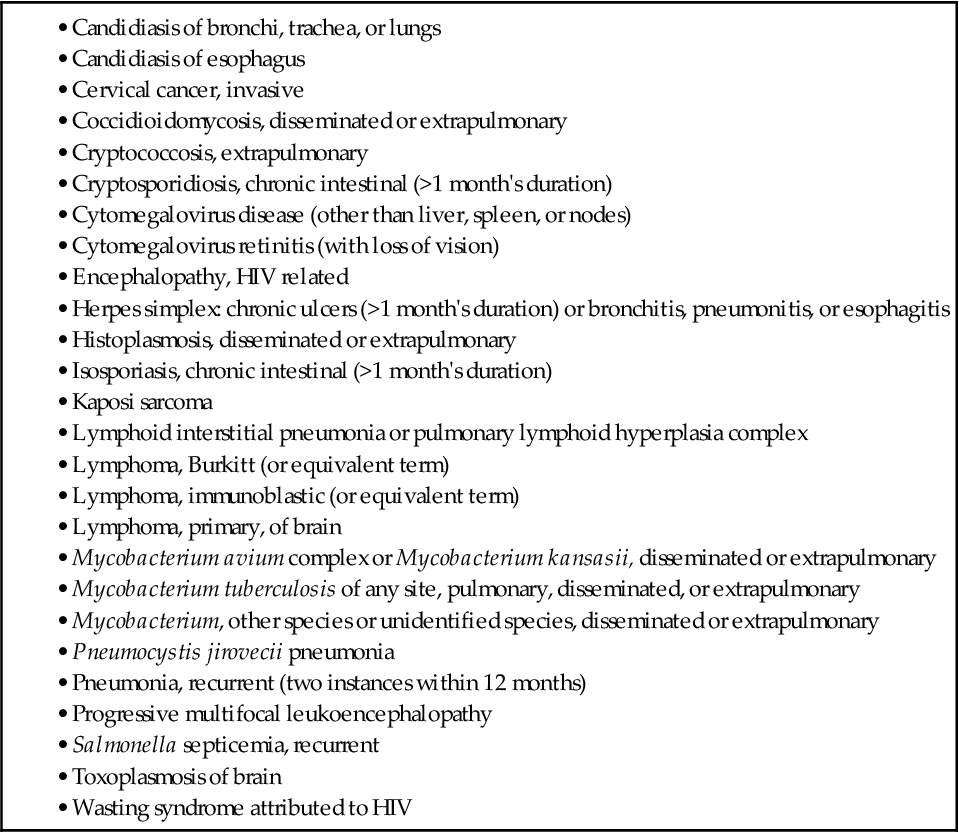
Centers for Disease Control and Prevention. (2008). Recommendations and reports: Appendix A—AIDS-defining conditions. Morbidity and Mortality Weekly Report, 57(RR-10), 9.
HIV Progression.
The time from the beginning of HIV infection to development of AIDS ranges from months to years. The range depends on how HIV was acquired, personal factors, and interventions. For people who have been transfused with HIV-contaminated blood, for example, AIDS often develops quickly. For those who become HIV positive as a result of a single sexual encounter, the period is much longer before progression to AIDS. Other personal factors that may influence progression to AIDS include frequency of re-exposure to HIV, presence of other sexually transmitted diseases (STDs), nutritional status, and stress.
Incidence/Prevalence
Since the beginning of the epidemic in the United States, more than 1.2 million cases of HIV/AIDS have been diagnosed, and more than 617,025 people have died of AIDS. Currently, more than 600,000 people in the United States are living with HIV/AIDS (CDC, 2011). This number is less than the total number of people in the United States estimated to be infected with HIV (1.1 million to 1.8 million). Worldwide, about 40 to 60 million people are currently infected with HIV, at least 30 million deaths from AIDS have occurred, and 33 million people are living with AIDS (WHO, 2010).
AIDS hits hardest among people between 21 and 44 years of age. The loss of productivity and wage-earning power among this group devastates the patient and strains the insurance and health care industry.
Most AIDS cases in North America occur among men who have had sex with other men (MSM) (53%) or individuals of either gender who have used injection drugs (16%) (CDC, 2011). The changing demographics of the infection indicate that the perception that HIV/AIDS is only a problem for homosexual white men is false (Kirton, 2011).
 Cultural Awareness
Cultural Awareness
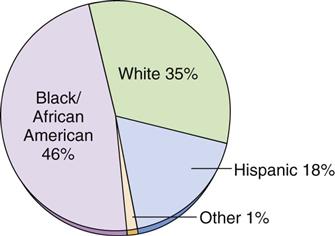
Most new HIV infections reported in the United States occur in racial and ethnic minority groups, particularly among Blacks/African Americans and Hispanics (CDC, 2011) (Fig. 21-5). These two groups show an increasing trend in HIV infection compared with a leveling off among white people. Factors that may increase the incidence of HIV infection and progression to AIDS among minority groups include:
• Fear of or lack of faith in the U.S. health care system
• Poverty and limited access to high-cost drugs
• Homophobia leading to increased bisexual activity among men of color
AIDS is a disease with a high mortality rate. The fatality rate is at least 60% for adults and, to date, there is no cure (WHO, 2010). Thus a major focus for health care in North America and worldwide is prevention of HIV infection. For those infected with HIV, drug therapy slows disease progression and, to be effective, it must be taken as prescribed for the rest of the patient’s life.
Health Promotion and Maintenance
HIV has been found in most body fluids of infected patients, including blood, semen, vaginal secretions, breast milk, amniotic fluid, urine, feces, saliva, tears, cerebrospinal fluid, lymph nodes, cervical cells, corneal tissue, and brain tissue. The fluids with the highest concentrations of HIV are the semen and the blood. It is also present in vaginal fluids and breast milk. Thus HIV is transmitted most often in these three ways:
Teach everyone about the transmission routes and ways to reduce their exposure (discussed next). Also stress that HIV is not transmitted by casual contact in the home, school, or workplace. Sharing household utensils, towels and linens, and toilet facilities does not transmit HIV. In addition, HIV is not spread by mosquitoes or other insects.
 Nursing Safety Priority
Nursing Safety Priority
Action Alert
Teach all people, regardless of age, gender, ethnicity, or sexual orientation, that they are susceptible to HIV infection.
Sexual Transmission
The CDC describes the ABC safer sex methods as A, abstinence; B, be faithful; and C, condoms (CDC, 2009b). Abstinence and mutually monogamous sex with a noninfected partner are the only absolutely safe methods of preventing HIV infection from sexual contact. Many forms of sexual expression can spread HIV infection if one partner is infected. The risk for becoming infected from a partner who is HIV positive is always present, although some sexual practices are more risky than others. The virus concentrates most heavily in blood and seminal fluid, although it is also present in vaginal secretions. Thus risk differs by gender, sexual act, and the viral load of the infected partner.
Gender affects HIV transmission. HIV is most easily transmitted when infected body fluids come into contact with mucous membranes or nonintact skin. The vagina has much more mucous membrane than does the penis. Thus HIV, like all other sexually transmitted diseases (STDs), is more easily transmitted from infected male to uninfected female than vice versa. Teach women the importance of always either using a vaginal or dental dam or female condom, or having their male partners use a condom.
Sexual acts or practices that permit infected seminal fluid to come into contact with mucous membranes or nonintact skin are the most risky for sexual transmission of HIV. The practice with the highest risk is anal intercourse. In anal intercourse, the risk increases when the penis and seminal fluid of an infected person come into contact with the mucous membranes of the uninfected partner’s rectum. Anal intercourse in which the semen depositor (inserting or active partner) is infected is a very risky sexual practice regardless of whether the semen receiver (receiving partner) is male or female. Anal intercourse not only allows seminal fluid to make contact with the mucous membranes of the rectum but also tears the mucous membranes, making infection more likely. Teach patients who engage in anal intercourse that the safer sex practice is for the semen depositor to wear a condom during this act.
Viral load, or the amount of virus present in blood and other body fluids, affects transmission. The higher the blood level of HIV (viremia), the greater the risk for sexual and perinatal transmission. Current highly active antiretroviral therapy (HAART) has caused the viral load of some infected patients to drop below detectable levels. Although there is less virus in seminal or vaginal fluids of people receiving HAART, the risk for transmission still exists (Kirton, 2011).
Safer sex practices are those that reduce the risk for nonintact skin or mucous membranes coming in contact with infected body fluids and blood. Teach everyone the importance of consistently using these safer sex practices:
• A latex or polyurethane condom for genital and anal intercourse (Chart 21-1)
• Latex gloves for finger or hand contact with the vagina or rectum
A promising area of research for prevention of sexual transmission is the use of vaginal gels that contain an antiretroviral agent (tenofovir or raltegravir). Early results indicate that if the gel is used before and after intercourse, new infections among women can be reduced by as much as 50% (Abdool Karim et al., 2010).
For those who believe they have been exposed to HIV as a result of sexual relations or other types of nonoccupational exposure, the CDC has guidelines for postexposure prophylaxis. The length and type of prophylaxis therapy depend on the nature of the exposure (Chart 21-2).
Chart 21-2
Patient and Family Education: Preparing for Self-Management
Nonoccupational Postexposure Prophylaxis (nPEP) to HIV
| Recommendations for nPEP with a substantial risk for HIV exposure is a 28-day course of the preferred regimen of HAART*† | |
| NNRTI-based | Efavirenz plus either lamivudine or emtricitabine plus either zidovudine or tenofovir |
| or | |
| PI-based | Lopinavir/ritonavir plus either lamivudine or emtricitabine plus zidovudine |
| A substantial risk is exposure of any of these: | |
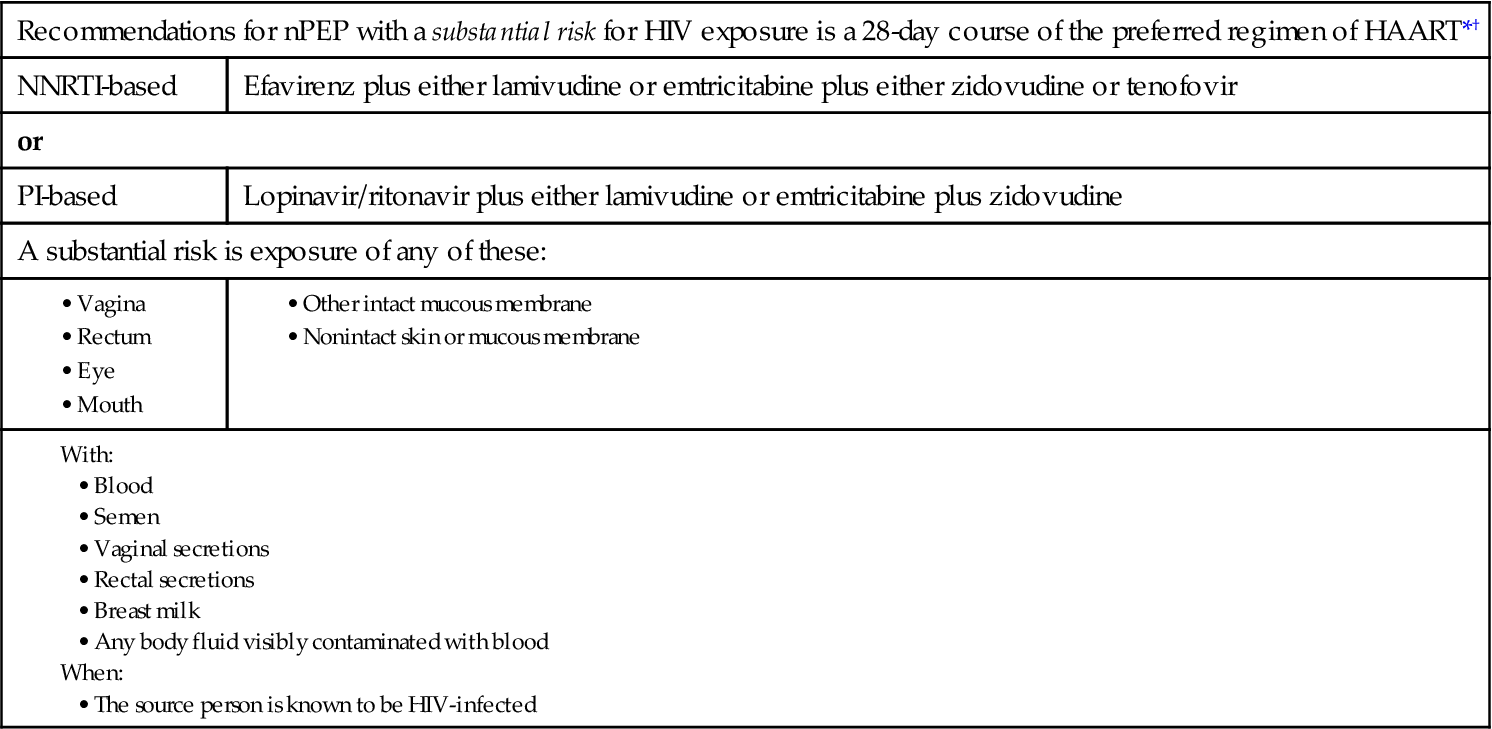
*Either when a substantial risk has occurred and more than 72 hours has passed since the exposure or when the exposure is considered to be a negligible risk, nPEP is not recommended.
†When a substantial risk has occurred and less than 72 hours has passed since the exposure but the HIV-infection status of the source person is not known, nPEP is determined on a case-by-case basis.
Data from Centers for Disease Control and Prevention. (2005). Antiretroviral postexposure prophylaxis after sexual, injection-drug use, or other nonoccupational exposure to HIV in the United States. Morbidity and Mortality Weekly Report, 54(RR-2), 1-27.
Parenteral Transmission
Preventive practices to reduce transmission among injection drug users (IDUs) include the use of proper cleaning of “works” (needles, syringes, other drug paraphernalia). Instruct IDUs to clean a used needle and syringe by first filling and flushing them with clear water. Next, the syringe should be filled with ordinary household bleach. The bleach-filled syringe should be shaken for 30 to 60 seconds. Advise IDUs to carry a small container with this solution whenever sharing needles. Some communities have a needle exchange program in which needles and syringes are used only once and are then exchanged for clean ones.
The risk for AIDS transmission through blood and blood products has been reduced to a national average of 0.02%. Several measures are used to protect the nation’s blood supply. All donated blood in North America is screened for the HIV antibody, and blood that is positive for HIV antibodies is discarded. Because of the time lag in antibody production (seroconversion) after exposure to HIV, infected blood can test negative for HIV antibodies. False-negative and false-positive results also can occur for other reasons. Inform patients that there is a small but real possibility of HIV transmission through blood and blood products. As a result, methods for reducing transfusion-related infections have included less reliance on standard transfusion therapy through more stringent criteria for transfusion, the use of growth factors to promote more rapid blood production in the patient, and an increase in autologous transfusion in which the patient donates his or her own blood to be transfused back at a later time.
Perinatal Transmission
The risk for perinatal transmission to infants in pregnant patients with HIV infection is about 25% in woman who are not using drug therapy for the disease compared with about 8% for women who are using drug therapy for HIV. Therefore encourage HIV-positive women who are pregnant to continue the therapy or, if they are not on antiviral therapy, to start the therapy as soon as possible.
HIV transmission can occur across the placenta during pregnancy, with infant exposure to blood and vaginal secretions during birth, or with exposure after birth through breast milk. Inform women of childbearing age with HIV infection about the risks for perinatal transmission. Consult a maternal-child textbook for more information about reducing perinatal transmission of HIV.
Transmission and Health Care Workers
Needle stick or “sharps” injuries are the main means of occupation-related HIV infection for health care workers. In addition, health care workers can be infected through exposure of nonintact skin and mucous membranes to blood and body fluids. Because of the time lag between the time of infection with HIV and the production of serum antibodies (seroconversion), infected people can test negative for HIV and still transmit the virus. The best prevention for health care providers is the consistent use of Standard Precautions for all patients as recommended by the CDC and required by The Joint Commission (TJC) (see Chapter 25). Chart 21-3 lists the recommended actions for prevention of HIV infection after a needle stick or other occupational exposure (postexposure prophylaxis [PEP]). When the source patient is known to be HIV negative, PEP is not recommended.
Chart 21-3
Best Practice for Patient Safety & Quality Care
Postexposure Prophylaxis (PEP) for Occupational HIV Exposure*

*When PEP therapy is instituted, the recommended course is 28 days.
†Basic PEP = Two drugs: (zidovudine plus lamivudine or emtricitabine); or (stavudine plus lamivudine or emtricitabine); or (tenofovir plus lamivudine or emtricitabine).
‡Expanded PEP = Three or more drugs: (zidovudine plus lamivudine or emtricitabine plus lopinavir/ritonavir); or (stavudine plus lamivudine or emtricitabine plus lopinavir/ritonavir); or (tenofovir plus lamivudine or emtricitabine plus lopinavir/ritonavir).
Data from Centers for Disease Control and Prevention. (2005). Updated Public Health Service guidelines for the management of health-care worker exposure to HIV and recommendations for postexposure prophylaxis. Morbidity and Mortality Weekly Report, 54(RR-9), 1-22.
The public may be concerned about HIV transmission by health care workers. Health care workers should wear gloves when in contact with patients’ mucous membranes or nonintact skin. Infected workers with weeping dermatitis or open lesions should not perform direct care. The CDC guidelines for preventing HIV transmission by health care workers during exposure-prone invasive procedures are listed in Chart 21-4. These include any procedure in which there is a risk for broken skin injury to the health care worker and the worker’s blood is likely to make contact with the patient’s body cavity, subcutaneous tissues, or mucous membranes. The purpose of these guidelines is to reduce the risk for HIV transmission to patients.
 Decision-Making Challenge
Decision-Making Challenge
Teamwork and Collaboration; Safety
You have just changed jobs and are working in the day-surgery and procedure center of a large hospital. You recognize from your former place of employment one of the gastroenterologists as a patient who is under treatment for HIV disease. He is performing short procedures, including endoscopy and colonoscopy.
Testing
Testing for HIV antibodies or other features of the virus is complex, requiring interpretation, counseling, and confidentiality. Testing plays a role in prevention because tests are a way of diagnosing HIV infection before immune changes or symptoms develop. A primary health care focus for testing is to teach those who test positive to modify their behaviors to prevent transmission to others. Therefore all sexually active people should know their HIV status. Chart 21-5 lists additional conditions for which HIV antibody testing is advised.
Pretest and post-test counseling must be performed by personnel trained in HIV issues. These counselors may be nurses, physicians, social workers, health educators, or even lay educators who have specialized training. Counseling helps the patient make an informed decision about testing and provides an opportunity to teach risk-reduction behaviors. Post-test counseling is needed to interpret the results, discuss risk reduction, and provide psychological support and health promotion information for the patient with a positive test result. People who test positive should also be counseled on how to inform sexual partners and those with whom they have shared needles. Testing methods, their accuracy, and indications are presented on pp. 368-369 in the Laboratory Assessment section.
Patient-Centered Collaborative Care
Assessment
The person who has HIV disease is monitored on a regular basis for changes in immune function or health status that indicate disease progression and warrant prophylaxis or intervention. The frequency of monitoring and reassessment varies from every 2 to 6 months based on disease progression and responses to treatment. This comprehensive and continuing assessment of the patient with HIV infection is crucial, because he or she may have problems related to disease in many organ systems. Assess subtle changes so that infections and other problems can be found early and treated.
History
Ask specifically about age, gender, occupation, and where the person lives. Thoroughly assess the current illness, including its nature, when it started, the severity of symptoms, associated problems, and any interventions to date. Ask the patient about when the HIV infection was diagnosed and what clinical symptoms led to that diagnosis. Ask him or her to give a chronologic history of infections and clinical problems since the diagnosis. Assess the patient’s health history, including whether he or she received a blood transfusion between 1978 and 1985 in the United States (before routine blood testing for HIV contamination). Blood testing for HIV contamination is not consistently performed in all parts of the world and is a source of infection for immigrants. Ask the immigrant patient about his or her history of transfusion therapy before coming to the United States.
Ask the patient about sexual practices, sexually transmitted diseases (STDs), and any major infectious diseases, including tuberculosis and hepatitis. If the patient has hemophilia, ask about treatment with clotting factors. Determine whether the patient has engaged in past or present injection drug use, including needle exposure and needle sharing. Assess the patient’s level of knowledge regarding the diagnosis, symptom management, diagnostic tests, treatments, community resources, and modes of HIV transmission. Also assess his or her understanding and use of safer sex practices. If knowledge deficits are found, provide the appropriate patient teaching.
Physical Assessment/Clinical Manifestations
HIV disease and AIDS are a progression continuum. The patient with HIV disease may either have few manifestations and problems or may have problems that are acute rather than chronically present. As the disease progresses, however, more health problems of long duration and greater severity occur. He or she may not realize that the disease is progressing. Assess for manifestations that cluster as symptoms of disease progression and may indicate that the treatment regimen needs to be modified (Chart 21-6).
Opportunistic Infections.
The patient with HIV/AIDS often develops pathogenic infections and opportunistic infections. Pathogenic infections are caused by virulent organisms and occur even among people whose immune systems are functioning normally. Opportunistic infections are those caused by organisms that are present as part of the body’s normal environment and are kept in check by normal immune function. Only when immune function is depressed are such organisms capable of causing infection.
Opportunistic infections occur because of the profound immunosuppression of the person with HIV infection. They may result from primary infection or reactivation of a latent infection. Opportunistic infections account for many of the clinical symptoms observed in HIV infection and can be protozoan, fungal, bacterial, or viral. More than one infection may be present at the same time. The presence of opportunistic infections may represent disease progression or a temporary further reduction of immune status. In either case, these infections can result in death if appropriate treatment is not started quickly. Priority nursing actions when caring for a patient who is HIV positive are continually assessing for the presence of an opportunistic infection and monitoring the patient’s response to therapy. Document all assessment findings in the patient’s medical record, and report to the health care provider those manifestations that may indicate an infection.
Opportunistic infections do not pose a threat to the immunocompetent health care worker caring for a patient with HIV infection or AIDS. When the patient with HIV infection or AIDS has a pathogenic infection, however, health care personnel must use precautions appropriate to the specific disease to prevent disease spread. For example, when the person with HIV/AIDS also has tuberculosis at a transmissible stage, Airborne Precautions are needed in addition to Standard Precautions. See Chapter 25 for a more complete discussion on Transmission-Based Precautions for specific infectious diseases.
Protozoal infections are common among patients with AIDS. Pneumocystis jiroveci pneumonia (PCP) (at one time thought to be the protozoa Pneumocystis carinii) is the most common opportunistic infection in persons infected with HIV. This organism is considered a protozoa by some scientists and a fungus by others. Assess for dyspnea on exertion, tachypnea, a persistent dry cough, and fever (usually low-grade and persistent). The patient with PCP may report fatigue and weight loss. Listen to breath sounds for crackles that may be present on lung auscultation.
Toxoplasmosis encephalitis, caused by Toxoplasma gondii, is acquired through contact with contaminated cat feces or by ingesting infected, undercooked meat. Assess the patient for subtle changes in mental status, neurologic deficits, headaches, and fever. Other symptoms to assess include difficulties with speech, gait, and vision; seizures; lethargy; and confusion. Perform a comprehensive baseline mental status examination and monitor the patient to detect subtle changes.
Cryptosporidiosis is an intestinal infection caused by Cryptosporidium organisms. In AIDS, this illness ranges from a mild diarrhea to a severe wasting with electrolyte imbalance. Diarrhea may result in fluid loss of up to 15 to 20 L/day. Ask the patient about the presence of diarrhea and whether he or she has had an unplanned weight loss of 5 pounds or more.
Fungal infections occur by overgrowth of normal body flora. Candida albicans is part of the natural flora of the intestinal tract. In the person with AIDS, candidiasis (overgrowth of the Candida fungus) occurs because the weakened immune system can no longer control fungal growth. Candida stomatitis or esophagitis is a frequent finding in AIDS. Patients may report food tasting “funny,” mouth pain, difficulty in swallowing, and retrosternal pain (pain behind the sternum). On examination of the mouth and the back of the throat, you may see cottage cheese–like, yellowish white plaques and inflammation (Fig. 21-6). Esophagitis is diagnosed by endoscopic biopsy and culture. Women with HIV disease or AIDS may have persistent vaginal candidiasis with severe pruritus (itching), perineal irritation, and a thick, white vaginal discharge.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


