Linda Laskowski-Jones
Care of Patients with Common Environmental Emergencies
Learning Outcomes
Safe and Effective Care Environment
Health Promotion and Maintenance
Physiological Integrity
5 Assess patients at high risk for environmental emergencies.
7 Prioritize first aid/prehospital interventions for patients who have arthropod bites.
8 Prioritize first aid/emergency care interventions for patients who have venomous snakebites.
10 Develop an evidence-based plan of care for a patient who is allergic to bees and is stung.
11 Prioritize care for patients who have been struck by lightning.
12 Prioritize care for patients who survive a drowning incident.
13 Explain best practices for patients who are at risk for or experience altitude-related illnesses.

http://evolve.elsevier.com/Iggy/
Answer Key for NCLEX Examination Challenges and Decision-Making Challenges
Audio Glossary
Key Points
Review Questions for the NCLEX® Examination
Recreational activities, as well as home and work responsibilities, make people of all ages leave their homes to go outdoors. However, seemingly harmless outside activities can have associated environmental risks, especially for older adults. Some risks, such as insect bites or stings, reptile bites, and environmental conditions, may also pose threats indoors. This chapter provides an overview of selected environmental emergencies, their initial emergency management (first aid), and acute care interventions. Illness and injury prevention strategies for nurses to incorporate into their own lifestyle and health teaching opportunities are also discussed.
Heat-Related Illnesses
High environmental temperature (above 95° F) and high humidity (above 80%) are the most common environmental factors causing heat-related illnesses. These illnesses include heat exhaustion and heat stroke. Some of the most vulnerable, at-risk populations for these problems are:
• People who work outside, such as construction and agricultural workers (more men than women)
• Illicit drug users (especially cocaine users)
• Outdoor athletes (recreational and professional)
Older adults have less body fluid volume and can easily become dehydrated when exposed to excessive heat and humidity. Heatstroke affects all races equally, given the same individual risk factors and the same environmental conditions. Because of socioeconomic disparities that disproportionatelyaffect black Americans, however, the annual death rate from heat-related illnesses in blacks is more than three times higher than in whites.
A patient’s health status can also increase the risk for heat-related illness, especially obesity, heart disease, fever, strenuous exercise, seizures, and all degrees of burns (even sunburn). In addition, the use of certain prescribed drugs such as beta-adrenergic blockers, angiotensin-converting enzyme (ACE) inhibitors, and diuretics increases the risk for heat-related illness (Auerbach et al., 2008).
Health Promotion and Maintenance
Teach older adults before participating in any hot weather activity how to consider their risks and to take steps to eliminate or minimize them whenever possible. Ask them to have a family member, friend, or neighbor check on them several times each day to ensure that there are no signs of heat-related illness. Chart 11-1 lists other essential heat-related illness prevention strategies for older adults, many of which apply to adults of any age.
Heat Exhaustion
Pathophysiology
Heat exhaustion is a syndrome resulting primarily from dehydration. It is caused by heavy perspiration, as well as inadequate fluid and electrolyte intake during heat exposure over hours to days. Patients feel ill, and their clinical manifestations resemble the flu. Although not a true emergency condition, if untreated, heat exhaustion can lead to heat stroke, a much more serious problem.
Patient-Centered Collaborative Care
In heat exhaustion, patients usually have flu-like symptoms with headache, weakness, nausea, and/or vomiting. Body temperature is not significantly elevated in this condition. The patient may continue to perspire despite dehydration.
 Nursing Safety Priority
Nursing Safety Priority
Action Alert
Assess the patient for orthostatic hypotension and tachycardia, especially the older adult who is predisposed to rapid dehydration. Older adults who are already dehydrated often experience acute confusion and are at risk for falls.
Ask the person experiencing heat exhaustion to immediately stop physical activity; move him or her to a cool place, and use cooling measures. Effective cooling measures include placing cold packs on the neck, chest, abdomen, and groin; soaking the person in cool water; or fanning him or her while spraying water on the skin (Auerbach et al., 2008). Remove any constrictive clothing. Provide an oral rehydrating solution such as a sports drink. Do not give salt tablets—they can cause stomach irritation, nausea, and vomiting. If these signs and symptoms persist, call an ambulance to transport the patient to the hospital.
In the clinical setting, monitor vital signs. Rehydrate the patient with IV 0.9% saline solution if nausea or vomiting persists. Draw blood for serum electrolyte analysis. Hospital admission is indicated only for patients who have other health problems that are worsened by the heat-related illness or for those with severe dehydration. The management of hypovolemic dehydration is discussed in more detail in Chapter 13.
Heat Stroke
Pathophysiology
Heat stroke is a true medical emergency in which body temperature may exceed 104° F (40° C). It has a high mortality rate if not treated in a timely manner. The victim’s heat regulatory mechanisms fail and cannot adjust for a critical elevation in body temperature (Laskowski-Jones, 2010). If the condition is not treated or the patient does not respond to treatment, organ dysfunction and death can result. In their cohort study of 16 emergency departments, Hausfater et al. (2010b) found that nine factors help predict mortality in patients admitted to emergency departments with non-exertional heat stroke (see Evidence-Based Practice box on p. 138).
The two major types of heat stroke are exertional and classic. Exertional heat stroke has a sudden onset and is often the result of strenuous physical activity in hot, humid conditions. Not being used to hot weather and wearing clothing too heavy for the environment are common contributing factors. Classic heat stroke, also referred to as non-exertional heat stroke, occurs over a period of time as a result of chronic exposure to a hot, humid environment, such as a home without air-conditioning in the high heat of the summer. It generally affects ill and older adults and causes several hundred deaths in the United States every year. The risk factors for heat stroke are similar to those for heat exhaustion.
Patient-Centered Collaborative Care
Assessment
Victims of heat stroke have a profoundly elevated body temperature (above 104° F [40° C]). Although the patient’s skin is hot and dry, the presence of sweating does not rule out heat stroke—people with heat stroke may continue to perspire.
Mental status changes occur as a result of thermal injury to the brain. Manifestations can include confusion, bizarre behavior, seizures, or even coma (Chart 11-2). Vital sign abnormalities may include hypotension, tachycardia, and tachypnea. Recent research demonstrates that cardiac troponin I (cTnI) is frequently elevated during non-exertional heat-related illnesses. A severe increase (>1.5 ng/mL) indicates severe myocardial damage and decreases the chance of patient survival 1 year after the event (Hausfater et al., 2010a).
Complications of classic heat stroke include multiple organ dysfunction syndrome (MODS), renal impairment, electrolyte and acid-base disturbances, coagulopathy (abnormal clotting), pulmonary edema, and cerebral edema (Johnson et al., 2008). Any of these problems can lead to death and are described in detail elsewhere in this book.
Interventions
Coordinate care with the health care team to recognize and treat immediately and aggressively to achieve optimal patient outcomes. Chart 11-3 lists evidence-based emergency care of patients with heat stroke.
First Aid/Prehospital Care
 Nursing Safety Priority
Nursing Safety Priority
Critical Rescue
After ensuring that the patient has a patent airway, effective breathing, and adequate circulation, use rapid cooling as the first priority for care. Methods for rapidly cooling include:
Drenching the victim with large amounts of icy water may be the fastest, most effective means to reduce core body temperature (Auerbach, 2009).
Do not give food or liquid by mouth because vomiting and aspiration are risks in patients with neurologic impairment, especially those older than 65 years. Immediate medical care using advanced life support is essential.
Hospital Care
The first priority for collaborative care is to monitor and support the patient’s airway, breathing, and circulatory status. Provide high-concentration oxygen therapy, start several IV lines with 0.9% saline solution, and insert a urinary catheter. Continue aggressive interventions to cool the patient until the rectal temperature is 100° F (37.8° C) (Auerbach, 2009). External continuous cooling methods include using cooling blankets and applying ice packs in the axilla and groin and on the neck and head. Internal cooling methods may include iced gastric and bladder lavage. Use a continuous core temperature–monitoring device (e.g., rectal or esophageal probe) or a temperature-monitoring urinary bladder catheter to prevent hypothermia.
If shivering occurs during the cooling process, give a parenteral benzodiazepine such as diazepam (Valium). Chlorpromazine (Thorazine) is an alternative agent. Because seizure activity can further elevate body temperature, be sure to have an IV benzodiazepine immediately available. Once the patient is stabilized, admission to a critical care unit is usually needed to monitor for complications such as multi-system organ dysfunction syndrome and severe electrolyte imbalances; these problems can lead to death.
 NCLEX Examination Challenge
NCLEX Examination ChallengeSnakebites
Although most snake species are nonvenomous (nonpoisonous) and harmless, there are two families of poisonous snakes in North America: pit vipers (Crotalidae) and coral snakes (Elapidae).
Pit vipers are named for the characteristic depression between each eye and nostril that serves as a heat-sensitive organ for locating warm-blooded prey. They include various species of rattlesnakes, copperheads, and cottonmouths and account for the majority of the poisonous snakebites in the United States (Figs. 11-1 and 11-2).


Coral snakes are found from North Carolina to Florida and in the Gulf states through Texas and the southwestern United States. They have broad bands of red and black rings, separated by yellow or cream rings. These nonaggressive snakes have short, fixed fangs and inject highly neurotoxic venom into prey.
Most snakes fear humans and attempt to avoid contact with them. Sudden, unexpected confrontations at close range often lead to defensive strikes. Awareness is the key to snakebite prevention.
Health Promotion and Maintenance
Chart 11-4 provides common-sense actions to avoid being bitten by a poisonous snake. Teach people who own snakes to follow these precautions. Remind them that snakebites can be life threatening.
North American Pit Vipers
North American pit vipers can be differentiated from harmless snakes by these key anatomic features:
• A triangular head that indicates the presence of venom glands and elliptical pupils
• Two retractable, curved fangs that have canals for venom flow
• Up to three sets of developing “replacement” fangs behind the primary fangs
Unlike copperheads and cottonmouths, rattlesnakes also have interlocking horny rings in their tails that vibrate and serve as a characteristic warning signal. Pit vipers can regulate the amount of venom flow through their fangs, depending, in part, on the size of the prey. The amount of venom injected in bites to humans varies. A bite might actually be “dry,” meaning there is no envenomation (venom injection), yet there are distinctive fang marks on the patient. In contrast, “harmless” snakes do not have venom glands or fangs but can bite and leave skin marks.
Pathophysiology
When providing emergency care to a victim of snakebite, determine if the venom has been injected into the body. The primary functions of venom are to immobilize, kill, and aid in digestion of prey. Therefore venom causes local and systemic toxic effects. The enzymes in venom break down human tissue proteins, alter membrane integrity, and impair blood clotting. The pathophysiologic effects of pit viper envenomation can lead to local tissue necrosis, massive tissue swelling, intravascular fluid shifts and hypovolemic shock, pulmonary edema, renal failure, hemorrhagic complications from disseminated intravascular coagulation (DIC), and death. These complications are discussed elsewhere in this book.
Patient-Centered Collaborative Care
Assessment
The clinical manifestations of venom release are based on the type and amount of venom injected; the bite location; and the age, size, and health status of the victim. Puncture wounds in the skin are a key local sign of pit viper envenomation. One or more puncture wounds may be present, depending on how many fangs the snake has and how many times the snake struck the patient. Severe pain, swelling, and redness or ecchymosis (bruising) in the area around the bite are common. Hours later, vesicles or hemorrhagic bullae may form. Systemic responses to venom must be distinguished from the effects of anxiety and panic related to being bitten by a snake. Commonly reported complaints include a minty, rubbery, or metallic taste in the mouth and tingling or paresthesias of the scalp, face, and lips. Other effects include muscle fasciculations (twitching) and weakness, nausea, vomiting, hypotension, seizures, and coagulopathy (clotting abnormalities) or DIC. If the bite site does not show evidence of local tissue swelling or redness within 8 hours, systemic effects are less likely to develop.
Interventions
First Aid/Prehospital Care
First aid interventions for snakebite should begin in the field and can improve the victim’s outcome.
 Nursing Safety Priority
Nursing Safety Priority
Critical Rescue
The first priority is to move the person to a safe area away from the snake and encourage rest to decrease venom circulation. Next, remove jewelry and constricting clothing before swelling worsens.
Immobilizing the affected extremity in a position of function with a splint helps limit the spread of the venom. Maintain the extremity at the level of the heart (Auerbach et al., 2008). Keep the person warm, and provide calm reassurance. Do not offer any alcohol because it can cause the venom to spread through vasodilation (Bledsoe et al., 2009). Do not incise or suck the wound, apply ice to it, or use a tourniquet!
Hospital Care
Acute care in a hospital is required as soon as possible because envenomation is a medical emergency. Supportive care includes supplemental oxygen, two large-bore IV lines, and infusion of crystalloid fluids such as normal saline solution or Ringer’s lactate solution. Apply continuous cardiac and blood pressure monitoring equipment to quickly detect clinical deterioration. Because venom can cause severe pain at the bite site, opioids are indicated. Provide tetanus prophylaxis and wound care as part of the collaborative plan of care.
Severe pit viper bites cause coagulopathy and promote hemorrhage and tissue destruction. Along with typical baseline laboratory studies, anticipate obtaining specimens for a coagulation profile, complete blood count (CBC), creatine kinase (CK), type and crossmatch for possible blood transfusion, and urinalysis. An electrocardiogram (ECG) is necessary to detect evidence of myocardial ischemia or other cardiac abnormalities.
Obtain pertinent patient history related to the event, including a full description of the snake’s appearance, the time the bite occurred, prehospital interventions, and any past incidence of snakebite or antivenom use. To accurately assess the development of tissue edema at the bite site, measure and record the circumference of the bitten extremity every 15 to 30 minutes.
Venom potency varies. Not all snakebite victims need antivenom administration. The decision whether or not to give antivenom is based on the severity of the snakebite. Table 11-1 classifies envenomation severity. Contact the regional poison control center so that toxicologists can provide specific advice for antivenom dosing and medical management.
TABLE 11-1
GRADES OF PIT VIPER ENVENOMATION
| ENVENOMATION | CHARACTERISTICS |
| None | Fang marks, but no local or systemic reactions |
| Minimal | Fang marks, local swelling and pain, but no systemic reactions |
| Moderate | Fang marks and swelling progressing beyond the site of the bite; systemic signs and symptoms, such as nausea, vomiting, paresthesias, and hypotension |
| Severe | Fang marks present with marked swelling of the extremity, subcutaneous ecchymosis, severe symptoms, including manifestations of coagulopathy |
From Auerbach, P.S., Donner, H.J., & Weiss, E.A. (2009). Field guide to wilderness medicine (3rd ed.). St. Louis: Mosby.
The newest and safest antivenom for pit viper bites is Crotalidae Polyvalent Immune Fab (CroFab), which is derived from sheep (ovine). This drug consists of specific antibody fragments of immunoglobulin G (IgG) that bind, neutralize, and redistribute toxins in pit viper venom so that they may be removed from the patient’s body (Schaeffer & Badillo, 2009). Unlike the older antivenoms that were derived from horse serum, serum sickness rarely occurs after IV CroFab administration. Serum sickness is a type III hypersensitivity reaction that develops within 3 to 21 days, first as a skin rash with progression to fever, joint pain, and pruritus (itching). Although mild to moderate allergic reactions such as pruritus and urticaria (hives) can occur, anaphylaxis is rare. If the patient has a known hypersensitivity to papain or papaya, which is used during the manufacturing process, CroFab is contraindicated unless the benefits are believed to outweigh the risks (Protherics, Inc., 2008). Give CroFab cautiously to patients who have:
• A previous allergic reaction to antivenom therapy
• A hypersensitivity to bromelain (a pineapple-derived enzyme) or sheep protein
• Sensitivity to mercury-containing products (the antivenom contains mercury)
CroFab should be given to patients as soon as possible, with the optimal timing within 6 hours of the bite (Protherics, Inc., 2008). The recommended initial IV dose is 4 to 6 vials infused over 60 minutes. During the first 10 minutes, the infusion should be slow (25-50 mL/hr). Monitor the patient closely for an allergic reaction (e.g., hives, rash, difficulty breathing). If symptoms are not effectively controlled with the first dose, an additional 4 to 6 vials are recommended. Once the symptoms are under control, 2 more vials of CroFab are administered every 6 hours for a total of 18 hours of administration (Protherics, Inc., 2008).
Coral Snakes
Pathophysiology
North American coral snakes are found in the southeastern and southwestern United States (Fig. 11-3). These snakes burrow into the ground and are nonaggressive. Coral snakes account for less than 1% of venomous snakebites in the United States (Norris, 2008). Their ability to inject venom is less efficient than that of the pit vipers. Their maxillary fangs are small and fixed in an upright position. Most bites occur when people attempt to handle the snake. Coral snake venom has two toxins: a nerve toxin and a muscle toxin. The amount of venom in an adult coral snake is enough to kill an adult.
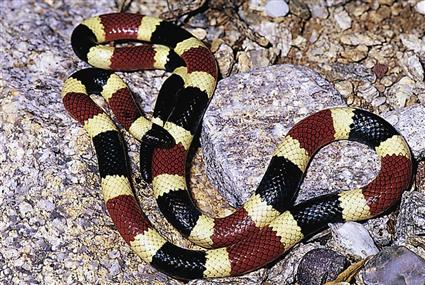
Coral snakes can be recognized by bands of black, red, and yellow that circle around the body of the snake. If a black band lies between the red and yellow bands, the snake is often nonvenomous. Several harmless species closely resemble the coral snake. A helpful memory aid for identifying coral snakes is “red on yellow can kill a fellow” and “red and black, venom lack.” Be aware that this saying applies only to coral snakes found in the United States!
Patient-Centered Collaborative Care
Assessment
Manifestations of coral snake envenomation are the result of its neurotoxic properties. The physiologic effect is to block neurotransmission, which produces ascending paralysis, reduced perception of pain, and, ultimately, respiratory paralysis (Wozniak et al., 2006). Unlike the pain from pit viper bites, pain at the coral snakebite site may be only mild and transient. The venom is spread via the lymphatic system, but swelling is unlikely. Fang marks may be difficult to find because of the coral snake’s small teeth. The toxic effects of coral snake venom also may be delayed up to 12 to 18 hours after a bite but then produce rapid clinical deterioration. Early signs and symptoms are nausea, vomiting, headache, pallor, and abdominal pain. Assess for neurologic manifestations, such as paresthesias (painful tingling), numbness, and mental status changes, as well as cranial nerve and peripheral nerve deficits. Total flaccid paralysis may occur later, and the patient may have difficulty speaking, swallowing, and breathing. Clotting changes do not occur.
Respiratory problems and cardiovascular collapse can occur in severe cases (Norris, 2008). Arterial blood gas analysis reveals respiratory insufficiency. The muscle toxin in the venom can cause an elevation in creatine kinase (CK) levels from muscle breakdown and produce myoglobinuria (release of muscle myoglobulin into the urine). Despite these clinical effects, death is rare if the patient receives timely management.
Interventions
First Aid/Prehospital Care
Because several varieties of harmless snakes resemble the coral snake, the first priority, if possible, is to identify the snake as a coral snake. However, if the snake cannot be positively identified, the victim should be treated as if venom has been injected. Because coral snake venom does not destroy tissue, the field treatment to limit the spread of venom includes the use of pressure immobilization techniques (Auerbach et al., 2008). The affected extremity is encircled snugly with an elastic bandage or roller gauze dressing to impede lymphatic flow and then splinted (Wozniak et al., 2006). This compression bandage must not be so tight that it impairs arterial flow. It should not be removed until the victim is managed at an acute care facility (Norris, 2008).
Hospital Care
Once in an acute care setting, patients who have had an actual or potential coral snake envenomation will have continuous cardiac, blood pressure, and pulse oximetry monitoring and are admitted to a critical care unit. Prepare to provide aggressive airway management via endotracheal intubation if respiratory insufficiency or severe neurologic impairment occurs. Aspiration of secretions is a significant risk for this patient.
Early antivenom administration is recommended (Auerbach et al., 2008). The onset of symptoms after coral snake bites can be delayed but can persist for a week in spite of treatment (Norris, 2008). The antivenom for the North American coral snake is Antivenin Micrurus fulvius (Wyeth). However, this drug is no longer in active production by any drug manufacturer; only very limited supplies are available. Contact the regional poison control center immediately for specific advice on antivenom administration and patient management. The same precautions are applied when administering coral snake antivenom as with Crotalidae (pit viper) antivenom.
 Nursing Safety Priority
Nursing Safety Priority
Drug Alert
The most significant risk to the victim is an anaphylactic response to the antivenom. Therefore ensure that the patient’s IV lines are patent and that emergency drugs (e.g., epinephrine, antihistamines, steroids) and resuscitation equipment are immediately available.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


