M. Linda Workman
Care of Patients with Cancer
Learning Outcomes
Safe and Effective Care Environment
Health Promotion and Maintenance
Psychosocial Integrity
Physiological Integrity
13 Prioritize nursing interventions for the patient with neutropenia or thrombocytopenia.
14 Prioritize nursing care for the patient receiving radiation therapy.
15 Explain the rationale for hormonal manipulation therapy.
17 Explain the basis and effects of targeted therapy for cancer.
18 Identify patients at risk for oncologic emergencies.

http://evolve.elsevier.com/Iggy/
Answer Key for NCLEX Examination Challenges and Decision-Making Challenges
Audio Glossary
Concept Map Creator
Key Points
Review Questions for the NCLEX® Examination
Cancer is a common problem in North America and other affluent societies. Most people fear cancer and consider a cancer diagnosis to involve suffering and death. In affluent countries, more than 50% of people diagnosed with cancer are cured and thousands of others live 5 years or longer (American Cancer Society, 2011; Canadian Cancer Society, 2010). Regardless of treatment type, cancer always affects a person’s physical and psychological functioning.
Providing care to patients and families experiencing cancer is complex and challenging. This chapter describes the general interventions for cancer and the problems associated with cancer treatment. For specific treatment regimens and patient problems that occur with specific cancer types, consult the chapters in which the cancer is described. Table 24-1 lists common cancer types and the specific locations within this text where the interventions are presented.
TABLE 24-1
TEXT LOCATION OF SPECIFIC CANCER CONTENT
| CANCER TYPE | CHAPTER | pages |
| Bladder (urolithial) | 69 | 1512-1515 |
| Brain | 47 | 1031-1036 |
| Breast | 73 | 1591-1608 |
| Cervical | 74 | 1624-1626 |
| Colorectal | 59 | 1245-1254 |
| Esophageal | 57 | 1211-1217 |
| Head and Neck | 31 | 590-600 |
| Leukemia | 42 | 880-889 |
| Lung | 32 | 632-640 |
| Lymphoma | 42 | 892-894 |
| Ovarian | 74 | 1626-1627 |
| Prostate | 75 | 1637-1642 |
| Renal cell carcinoma | 70 | 1532-1533 |
| Skin | 27 | 502-505 |
| Stomach (gastric) | 58 | 1234-1238 |
General Disease-Related Consequences of Cancer
Cancer can develop in any organ or tissue and destroys normal tissue, which decreases function of that tissue or organ. Even when cancers occur in nonvital tissues or organs, they can cause death by metastasizing (spreading) into vital organs and disrupting critical physiologic processes (see Chapter 23). Cancers that are left untreated often cause:
These impairments cause great physical and emotional distress. Without intervention, cancer invasion of normal tissues leads to death.
Reduced Immunity and Blood-Producing Functions
Impaired immune and blood-producing functions occur most often in patients with leukemia and lymphoma but also can occur with any cancer that invades the bone marrow. Tumor cells enter the bone marrow and reduce the production of healthy white blood cells (WBCs), which are needed for normal immune function. Thus patients who have cancer, especially leukemia, are at an increased risk for infection.
When cancer invades the bone marrow, it also causes anemia by decreasing the number of red blood cells (RBCs) and causes thrombocytopenia by decreasing the number of platelets (Fitch et al., 2009). These changes may be caused by the cancer itself or by cancer treatment, especially chemotherapy. The patient feels weak and fatigued and is at risk for bleeding.
Altered Gi Structure and Function
Cancer can alter GI function and impair nutrition. Abdominal tumors may obstruct or compress structures anywhere in the GI tract, reducing the ability to absorb nutrients and eliminate wastes. Tumors often also increase metabolic rate and increase the need for nutrients at a time when the patient has less energy for meal preparation or eating.
Tumors that invade the liver profoundly damage this organ, which has many important metabolic functions. Cancer-related reduced liver function leads to malnutrition and death.
Many patients with cancer have anorexia that often interferes with their ability to meet energy needs. Cachexia (extreme body wasting and malnutrition) develops from an imbalance between food intake and energy use (increased catabolism). This problem may occur even when nutritional intake appears adequate (Granda-Cameron et al., 2010). Changes in taste can result from the cancer or the treatment and reduce appetite.
Nutritional support for the patient with cancer, especially one undergoing cancer therapy, is complex. A diet high in protein and carbohydrates is often prescribed to help him or her maintain weight and to provide the nutrients needed for energy and cellular repair. Patients and families often believe cancer can be cured more easily if weight is gained or maintained. Currently no one nutritional plan meets the needs of all patients with cancer.
Motor and Sensory Deficits
Motor and sensory deficits occur when cancers invade bone or the brain or compress nerves. In patients with bone metastasis, the primary cancer started in another organ (e.g., lung, prostate, breast). The bone sites most often affected are the vertebrae, ribs, pelvis, humerus, scapula, sternum, skull, and clavicle. Bone metastasis causes pain, fractures, spinal cord compression, and hypercalcemia, each of which reduces mobility.
Patients may have sensory changes if the spinal cord is damaged or if nerves are compressed. Sensory, motor, and cognitive functions are impaired when cancer spreads to the brain. Any tumor, benign or malignant, growing in the brain can destroy healthy brain tissue and cause death.
The patient with cancer may also have pain, especially chronic pain. Pain does not always accompany cancer, but it can be a major problem for those with terminal cancer. Chapter 5 provides an in-depth discussion of the causes and management of cancer pain. The Concept Map on p. 42 presents nursing care issues related to chronic cancer pain.
Reduced Oxygenation
Cancer can disrupt oxygenation in several ways and often results in death. For example, tumors in the airways cause airway obstruction. If lung tissue is involved, lung capacity is decreased. Tumors can also press on blood and lymph vessels in the chest, blocking blood flow through the chest and lungs, which results in pulmonary edema and dyspnea. Tumors can thicken the alveolar membrane and damage pulmonary blood vessels, reducing gas exchange. With any lung tumor (primary or metastatic), patients have hypoxia and poor tissue oxygenation.
 NCLEX Examination Challenge
NCLEX Examination ChallengeCancer Management
The purpose of cancer management is to prolong survival time or improve quality of life. Without cancer therapy, most patients with cancer would die within months of diagnosis. Cancer therapy includes surgery, radiation, chemotherapy, hormonal manipulation, photodynamic therapy, immunotherapy, and targeted therapy. These therapies may be used separately or in combination to kill cancer cells. The types of therapy used depend on the specific type of cancer, whether the cancer has spread, and the health of the patient. Treatment regimens (protocols) have been established for most types of cancer. These regimens are based on experiments with cancer cells and animals and on experience with other patients with cancer.
Surgery
Overview
Surgery for cancer involves the removal of diseased tissue. If cancer is confined to the removed tissue, surgery alone can result in a “cure” for that cancer. Although many cancers have spread too far at the time of diagnosis for surgery alone to result in a cure, it is often a useful part of diagnosis, treatment, follow-up, and rehabilitation.
Cancer surgery may be used for prophylaxis, diagnosis, cure, control, palliation, assessing therapy effectiveness, and reconstruction. Prophylactic surgery removes “at-risk” tissue to prevent cancer development. It is performed when a patient has either an existing premalignant condition or a family history that strongly predisposes the person to development of a specific cancer. For example, removing a benign polyp from the colon before it can develop into colon cancer is a prophylactic action. Diagnostic surgery (biopsy) is the removal of all or part of a suspected lesion for examination and testing. It provides proof of the presence of cancer. Curative surgery removes all cancer tissue. Surgery alone can result in a cure rate of 27% to 30% when all visible and microscopic tumor is removed or destroyed. Cancer control, or cytoreductive surgery, removes part of but not the entire tumor. It is also known as “debulking” surgery and alone cannot result in a cure. It decreases the number of cancer cells and increases the chances that other therapies can be successful. Palliative surgery focuses on improving the quality of life during the survival time, not on cure. Examples include removal of tumor tissue that is causing pain, obstruction, or difficulty swallowing. The specific procedure used depends on the patient’s specific problem. Second-look surgery is a “rediagnosis” after treatment. The purpose is to assess the disease status in patients who have been treated and have no symptoms of remaining tumor. The results of this surgery are used to determine whether a specific therapy should be continued or discontinued. This type of surgery is most commonly used with ovarian cancer. Reconstructive or rehabilitative surgery increases function, enhances appearance, or both. Examples include breast reconstruction after mastectomy, replacement of the esophagus, bowel reconstruction, revision of scars, and placement of penile implants.
Side Effects of Surgical Therapy
Unlike surgery performed for many other reasons, cancer surgery often involves the loss of a specific body part or its function. Sometimes whole organs are removed, such as the kidney, lung, breast, testes, leg, or tongue. Any organ loss reduces function. The amount of function lost and how much the loss affects patients depend on the location and extent of the surgery. Some cancer surgery results in major scarring or disfigurement. Patients are anxious about the chances of surviving the cancer and also may be grieving about a change in appearance or lifestyle.
Patient-Centered Collaborative Care
The physical care needs of the patient having surgery for cancer are similar to those related to surgery for other reasons (see Chapters 16, 17, and 18). For cancer surgery, two additional priority care needs are psychosocial support and assisting the patient to achieve or maintain maximum function.
Often cancer surgery occurs within days of the diagnosis, before the patient and family have time to adjust. Assess the patient’s and family’s ability to cope with the uncertainty of cancer and its treatment and with the changes in body image and role. For example, surgery involving the genitals, urinary tract, colon, and rectum may permanently damage these organs, resulting in changes in the patient’s means of sexual expression or control of elimination. Procedures to create a urinary or fecal diversion may damage nerves, causing erectile dysfunction in men and painful intercourse in women. Removal of a lung reduces the patient’s respiratory capacity and forever limits his or her ability to engage in physical activities.
Coordinate with the health care team to support the patient. Encourage the patient and family to express their concerns. Help the patient accept changes in appearance or function by encouraging him or her to look at the surgical site, touch it, and participate in dressing changes. Provide information about support groups such as those sponsored by the American Cancer Society (www.cancer.org) or Canadian Cancer Society (www.cancer.ca). Some cancer organizations have support groups for patients and separate support groups for patients’ spouses and children. Discuss having a person who has coped with the same issues come for a visit. Such visits can be valuable in showing the patient that many aspects of life can be the same after cancer treatment. If the patient is open to this type of support, arrange for a visit. For patients who have persistent sadness or depression as a result of appearance changes from cancer surgery, a referral to a mental health counselor and drug therapy may be needed (Weaver, 2009).
Reduced function may be an outcome for some types of cancer surgery. For example, a modified radical mastectomy for breast cancer can lead to muscle weakness and reduced arm function on the surgical side. Performing specific exercises after surgery can reduce functional loss. These exercises can be painful, and the patient needs encouragement to perform them. Teach the patient about the importance of performing and increasing the intensity of the exercises to regain as much function as possible and prevent complications. Coordinate with the physical therapist, occupational therapist, and family members to plan strategies individualized to each patient to regain or maintain optimal function.
Radiation Therapy
Overview
The purpose of radiation therapy for cancer is to destroy cancer cells and have minimal damaging effects on the surrounding normal cells. The effects of radiation are seen only in the tissues in the path of the radiation beam; thus this type of therapy is a local treatment. For example, radiation to the chest for breast cancer or lung cancer causes skin changes and hair loss only on the area of the chest actually being irradiated. The person does not lose his or her scalp hair. Some effects are apparent within days or weeks, whereas other effects on deeper tissues may not be apparent for months to years after radiation therapy is completed.
Most radiation therapy for cancer is ionizing radiation. When cells are exposed to it, particles within the cell’s nucleus are rearranged, resulting in a tremendous release of intracellular energy. Ionizing radiation is given off by many elements, including radium, and radioactive isotopes of specific elements. For example, a radioactive isotope of cobalt is used in radiation therapy for cancer.
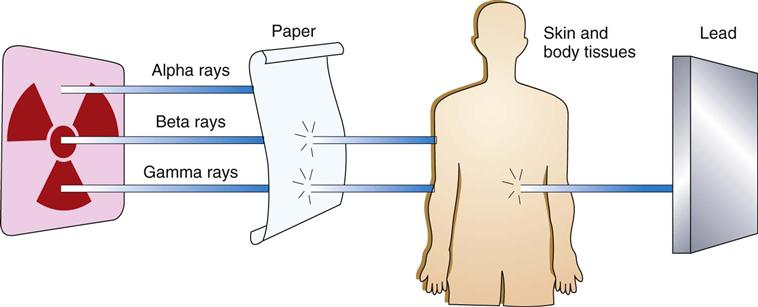
As a radioactive element breaks down (decays), radiation energy is released as high energy particles (alpha particles and beta particles) and high energy photons (gamma rays). X-rays are radiation that is generated by machine. X-ray photons and gamma ray photons are identical in their effects on cells.
Cells damaged by radiation either die outright or become unable to divide. Radiation damage can occur anytime a cell is exposed to radiation, not just when it is actively dividing. However, the damage is greater to dividing cells than to non-dividing cells when exposed to radiation.
Three different types of energy, or rays, are produced by radioactive elements: gamma rays, alpha particles, and beta particles. These energies vary in their ability to penetrate tissues and damage cells (Fig. 24-1). Gamma rays are used most commonly for radiation therapy because of their ability to deeply penetrate tissues (Camporeale, 2008). Beta particles are weaker and must be placed within or very close to the cancer cells for cancer therapy (see discussion of brachytherapy on pp. 412-413). Alpha particles are not used as cancer therapy.
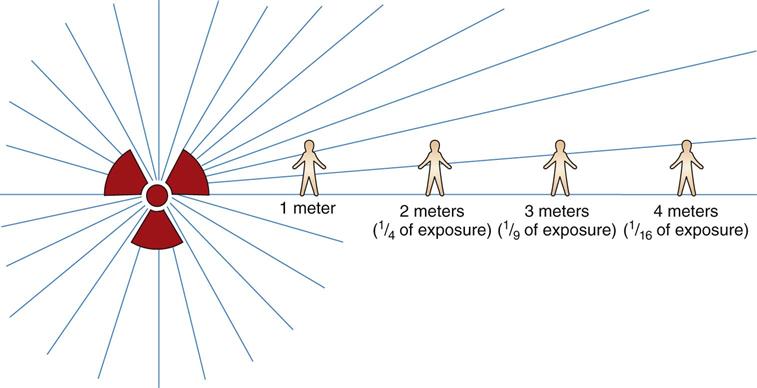
The amount of radiation delivered to a tissue is called the exposure; the amount of radiation absorbed by the tissue is called the radiation dose. The dose is always less than the exposure because some energy is lost as scatter on the way to the tissue. The three factors determining the absorbed dose are the intensity of exposure, the duration of exposure, and the closeness of the radiation source to the cells (Camporeale, 2008).
The intensity of the radiation decreases with the distance from the radiation source (Fig. 24-2). This factor is known as the inverse square law. For example, the radiation dose received at a distance of 2 meters from the radiation source is only one fourth of the dose received at a distance of 1 meter from the radiation source; the dose of radiation received at 3 meters is only one ninth of the dose received at 1 meter.
If the dose of radiation is high enough, all cells are killed immediately. This does not happen with cancer radiation therapy because cells within a tumor absorb the radiation dose slightly differently. Therefore their overall response to the radiation is slightly different. A few cells die immediately, and more die within the next 24 hours as they attempt to divide. Some cells become sterile as a result of this single treatment. Still other cells repair the radiation-induced damage and recover.
Radiation therapy usually is given as a series of divided doses because of the varying responses of all cancer cells within a given tumor. Most often, small doses of radiation are given on a daily basis for a set time period to allow greater destruction of cancer cells while reducing the damage to normal tissues. Absorbed radiation doses are described in units called gray (gy). (The older term for radiation dose was rad for radiation absorbed dose. One gy is the same as 100 rad.) One gy is equal to one joule of energy absorbed by one kg of a material. The total dose of radiation used depends on tumor size and location and on the radiation sensitivity of the tumor and nearby tissues. Some normal tissues are more sensitive than others to radiation. For example, breast tissue tolerates much higher doses of radiation than the liver does. A total dose of 50 to 60 gy might be prescribed for a breast cancer. However, only 12 gy might be prescribed for a liver tumor, because a higher dose would destroy healthy liver cells as well as the tumor.
Radiation Delivery Methods and Devices
Radiation delivery types for cancer therapy are teletherapy and brachytherapy. The type used depends on the patient’s general health and on the shape, size, and location of the tumor to be irradiated. The ideal radiation dose is one that can kill the cancer cells with an acceptable level of damage to normal tissues (damage to normal tissues cannot be avoided).
Teletherapy is radiation delivered from a source outside of the patient. Because the source is external, the patient is not radioactive and is not hazardous to others.
One newer method of teletherapy is intensity modulated radiation therapy (IMRT). This type of radiation breaks up the single beam into thousands of smaller beams that allow better focus on the tumor.
Another newer method of teletherapy is stereotactic body radiotherapy (SBRT). This method uses three-dimensional tumor imaging to identify the exact tumor location, which allows more precise delivery of higher radiation doses and spares more of the surrounding tissue. Usually, the total dosage is delivered in one to five separate treatment sessions. Currently, this approach is most commonly used for small, localized lung cancers (Smink & Schneider, 2008).
Regardless of the teletherapy delivery method, the exact location of the tumor is determined for therapy accuracy. Once the pattern of radiation delivery is determined, the patient must always be in exactly the same position for all treatments (Camporeale, 2008). Ensure that the patient can get into and maintain this position. Position-fixing devices and markings, either on the patient’s body or on the devices, ensure the proper position each day of treatment. The markings may be small permanent “tattoos,” ink outlines on the skin, or a marked covering laid over the skin during positioning. Position-fixing devices include customized external vacuum-type body molds, foam-based body molds, and fiberglass splints (Smink & Schneider, 2008).
Brachytherapy means “short” or “close” therapy. The radiation source comes into direct, continuous contact with the tumor tissues for a specific time period. This method provides a high dose of radiation in tumor tissues and a very limited dose in surrounding normal tissues.
Brachytherapy uses radioactive isotopes either in solid form or within body fluids. Isotopes can be delivered to the tumor tissues in several ways. With all types of brachytherapy, the radiation source is within the patient. Therefore the patient emits radiation for a period of time and is a hazard to others (Waring & Gosselin, 2010). When the isotopes used are unsealed and suspended in a fluid, they are given by the oral or IV routes or instilled within body cavities. An example of brachytherapy with soluble isotopes is the ingestion or injection of the radionuclide iodine-131 (131I) (an iodine base with a half-life of 8.05 days) to treat some thyroid cancers. The iodine concentrates in the thyroid gland and destroys the thyroid cancer cells. When the isotopes are unsealed, they enter body fluids and eventually are eliminated in waste products, which are radioactive and should not be directly touched by other people. After the isotope is completely eliminated from the body, neither the patient nor the body wastes are radioactive.
Solid or sealed radiation sources are implanted within or near the tumor. These sources can be temporary or permanent. Most implants emit continuous, low-energy radiation to tumor tissues. Some devices (e.g., seeds or needles) can be placed into the tissues and stay in place by themselves. Some devices are so small and the half-life of the isotope so short that the device is permanently left in place (most often for prostate cancer) and, over time, completely loses its radioactivity. Other devices are removed and reused in other patients. Some sources must be held in place during therapy using special applicators. While the solid implants are in place, the patient emits radiation but excreta are not radioactive and do not pose a hazard to anyone.
Traditional implants deliver “low-dose rates” (LDRs) of radiation continuously and patients are hospitalized for several days. “High-dose rate” (HDR) implant radiation is another delivery type. The patient comes into the radiation therapy department several times a week, and a stronger radiation implant is placed for only an hour or so each time. The patient goes home between treatments and is radioactive only when the implant is in place (Waring & Gosselin, 2010). Chart 24-1 lists the best practices for care of the patient with sealed implant radiation sources and for the safety of the personnel providing the care.
Side Effects of Radiation Therapy
The immediate and long-term side effects of all types of radiation are limited to the tissues exposed to the radiation. Therefore the side effects vary according to the site (Ruppert, 2011). Skin changes and hair loss are local but are often permanent depending on the total absorbed dose.
Altered taste sensations and fatigue are two common systemic side effects noted by patients receiving teletherapy, regardless of the radiation site. Taste changes are thought to be caused by metabolites released from dead and dying cells. Many patients develop an aversion to the taste of red meats. Fatigue may be related to the increased energy demands needed to repair damaged cells. Regardless of the cause, radiation-induced fatigue can be debilitating and may last for months (Kuchinski et al., 2009).
Radiation damage to normal tissues during cancer therapy can start inflammatory responses that lead to tissue fibrosis and scarring. These effects may appear years after radiation treatment. For example, women who receive HDR therapy for uterine cancer may develop radiation-induced changes in the colon (which also was irradiated) years later, resulting in constipation and obstruction.
Patient-Centered Collaborative Care
Most patients are anxious about radiation and look to the nurse to explain the purpose and side effects of radiation therapy. Accurate, objective information about radiation therapy helps patients cope with the treatment and continue to participate in normal activities.
Skin in the path of radiation becomes very dry and may break down. Teaching patients about skin care needs during radiation therapy is a priority nursing intervention. Chart 24-2 lists skin care and other precautions needed with external radiation therapy. Instruct the patient to not remove any temporary ink markings when cleaning the skin until the entire course of radiation therapy is completed. At one time, patients were told to avoid using lotions or other skin care products within 4 hours of the radiation therapy; however, this practice is not evidence-based and is now controversial (Bieck, Phillips, & Steele-Moses, 2010). Teach patients to follow the radiation-oncology department’s policy regarding the use and timing of skin care products. Use of skin care products designed to manage or protect the skin from radiation damage does reduce the degree of skin problems that develop during a full course of radiation therapy (Gosselin et al., 2010) (see the Evidence-Based Practice box on p. 414).
 Nursing Safety Priority
Nursing Safety Priority
Action Alert
Skin in the radiation path is more sensitive to sunburn and damage. Advise against direct skin exposure to the sun during treatment and for at least 1 year after completing radiation therapy.
The normal tissues most sensitive to external radiation are bone marrow cells, skin, mucous membranes, hair follicles, and germ cells (ova and sperm). When possible, these tissues are shielded from radiation during therapy. At times, they are in the radiation path and cannot be protected from exposure. Some changes caused by radiation are permanent. The long-term problems vary with the location and dose of radiation received. For example, radiation to the throat and upper chest can cause difficulty in swallowing. Combined with taste alteration, this problem can lead to reduced nutrition. A registered dietitian is part of the radiation oncology team (Gosselin et al., 2008). Head and neck radiation may damage the salivary glands and cause dry mouth (xerostomia), which increases the patient’s lifelong risk for tooth decay. Bone exposed to radiation therapy is less dense and breaks more easily. Teach about the symptoms that might be expected from the location and dose of radiation (see Table 24-1 for the location of this information for different cancer types).
 NCLEX Examination Challenge
NCLEX Examination ChallengeChemotherapy
Overview
Chemotherapy, the treatment of cancer with chemical agents, is used to cure and to increase survival time. It has some selectivity for killing cancer cells over normal cells. This killing effect on cancer cells is related to the ability of chemotherapy to damage DNA and interfere with cell division. Tumors with rapid growth are most sensitive to chemotherapy.
As described in Chapter 23, cancer cells can separate from the original tumor, spread to new areas, and establish new cancers at distant sites (metastasize). Patients with metastatic cancer will die unless treatment eliminates the metastatic cancer cells along with the original cancer cells. Chemotherapy is useful in treating cancer because its effects are systemic, providing the opportunity to kill metastatic cancer cells that may have escaped local treatment. Chemotherapy used along with surgery or radiation is termed adjuvant therapy.
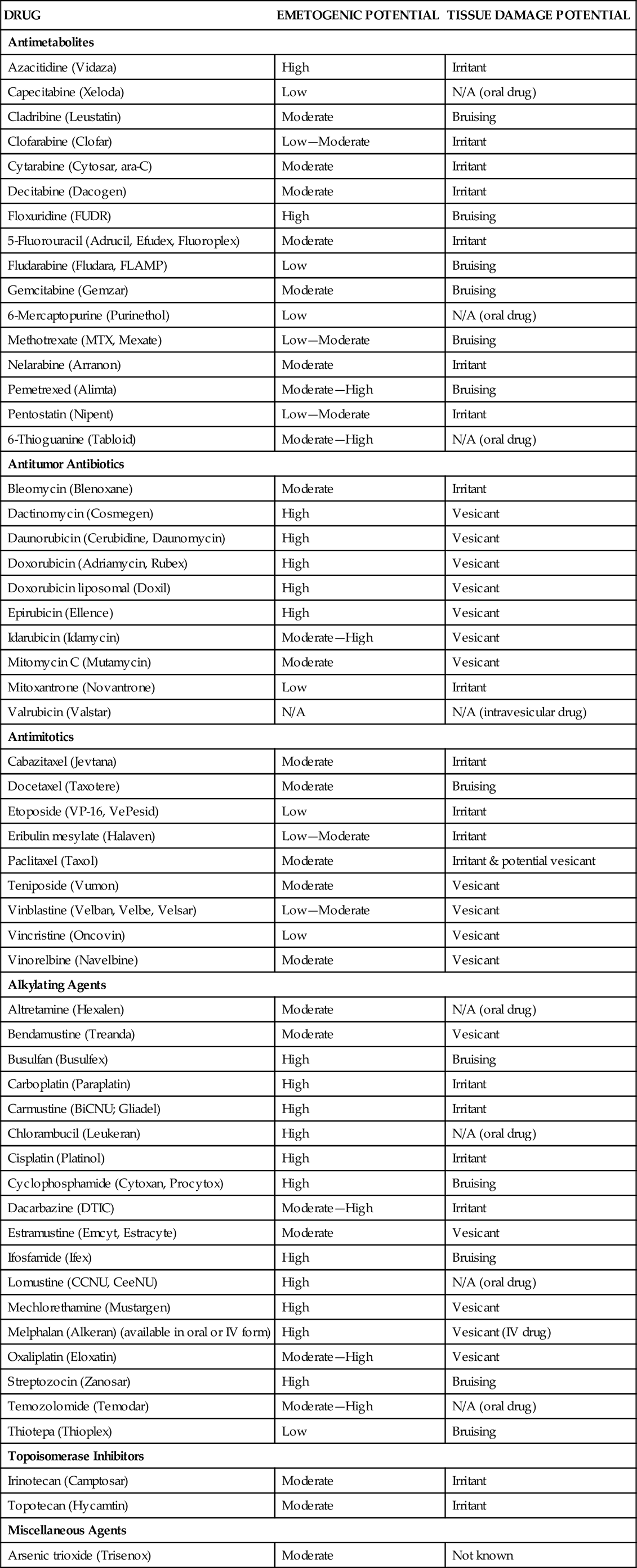
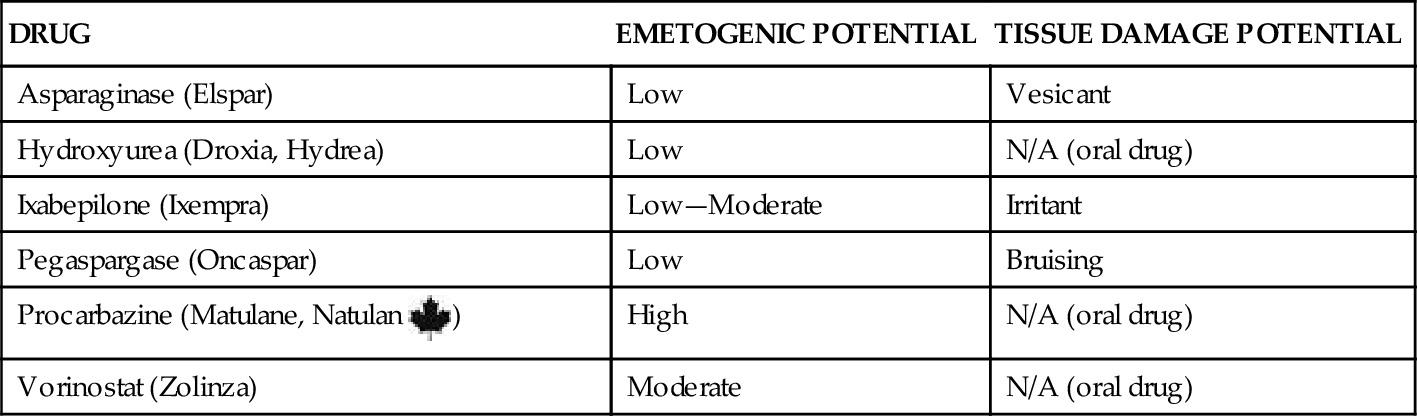
Drugs used for chemotherapy usually are given systemically and exert their cell-damaging (cytotoxic) effects against healthy cells as well as cancer cells. The normal cells most affected by chemotherapy are those that divide rapidly, including skin, hair, intestinal tissues, spermatocytes, and blood-forming cells. These drugs are classified by the specific types of action they exert in the cancer cell. Table 24-2 lists categories, drugs, and their potential to induce nausea and vomiting (emetogenic) or to damage surrounding tissue.
TABLE 24-2
CATEGORIES OF CHEMOTHERAPEUTIC DRUGS
| DRUG | EMETOGENIC POTENTIAL | TISSUE DAMAGE POTENTIAL |
| Antimetabolites | ||
| Azacitidine (Vidaza) | High | Irritant |
| Capecitabine (Xeloda) | Low | N/A (oral drug) |
| Cladribine (Leustatin) | Moderate | Bruising |
| Clofarabine (Clofar) | Low—Moderate | Irritant |
| Cytarabine (Cytosar, ara-C) | Moderate | Irritant |
| Decitabine (Dacogen) | Moderate | Irritant |
| Floxuridine (FUDR) | High | Bruising |
| 5-Fluorouracil (Adrucil, Efudex, Fluoroplex) | Moderate | Irritant |
| Fludarabine (Fludara, FLAMP) | Low | Bruising |
| Gemcitabine (Gemzar) | Moderate | Bruising |
| 6-Mercaptopurine (Purinethol) | Low | N/A (oral drug) |
| Methotrexate (MTX, Mexate) | Low—Moderate | Bruising |
| Nelarabine (Arranon) | Moderate | Irritant |
| Pemetrexed (Alimta) | Moderate—High | Bruising |
| Pentostatin (Nipent) | Low—Moderate | Irritant |
| 6-Thioguanine (Tabloid) | Moderate—High | N/A (oral drug) |
| Antitumor Antibiotics | ||
| Bleomycin (Blenoxane) | Moderate | Irritant |
| Dactinomycin (Cosmegen) | High | Vesicant |
| Daunorubicin (Cerubidine, Daunomycin) | High | Vesicant |
| Doxorubicin (Adriamycin, Rubex) | High | Vesicant |
| Doxorubicin liposomal (Doxil) | High | Vesicant |
| Epirubicin (Ellence) | High | Vesicant |
| Idarubicin (Idamycin) | Moderate—High | Vesicant |
| Mitomycin C (Mutamycin) | Moderate | Vesicant |
| Mitoxantrone (Novantrone) | Low | Irritant |
| Valrubicin (Valstar) | N/A | N/A (intravesicular drug) |
| Antimitotics | ||
| Cabazitaxel (Jevtana) | Moderate | Irritant |
| Docetaxel (Taxotere) | Moderate | Bruising |
| Etoposide (VP-16, VePesid) | Low | Irritant |
| Eribulin mesylate (Halaven) | Low—Moderate | Irritant |
| Paclitaxel (Taxol) | Moderate | Irritant & potential vesicant |
| Teniposide (Vumon) | Moderate | Vesicant |
| Vinblastine (Velban, Velbe, Velsar) | Low—Moderate | Vesicant |
| Vincristine (Oncovin) | Low | Vesicant |
| Vinorelbine (Navelbine) | Moderate | Vesicant |
| Alkylating Agents | ||
| Altretamine (Hexalen) | Moderate | N/A (oral drug) |
| Bendamustine (Treanda) | Moderate | Vesicant |
| Busulfan (Busulfex) | High | Bruising |
| Carboplatin (Paraplatin) | High | Irritant |
| Carmustine (BiCNU; Gliadel) | High | Irritant |
| Chlorambucil (Leukeran) | High | N/A (oral drug) |
| Cisplatin (Platinol) | High | Irritant |
| Cyclophosphamide (Cytoxan, Procytox) | High | Bruising |
| Dacarbazine (DTIC) | Moderate—High | Irritant |
| Estramustine (Emcyt, Estracyte) | Moderate | Vesicant |
| Ifosfamide (Ifex) | High | Bruising |
| Lomustine (CCNU, CeeNU) | High | N/A (oral drug) |
| Mechlorethamine (Mustargen) | High | Vesicant |
| Melphalan (Alkeran) (available in oral or IV form) | High | Vesicant (IV drug) |
| Oxaliplatin (Eloxatin) | Moderate—High | Vesicant |
| Streptozocin (Zanosar) | High | Bruising |
| Temozolomide (Temodar) | Moderate—High | N/A (oral drug) |
| Thiotepa (Thioplex) | Low | Bruising |
| Topoisomerase Inhibitors | ||
| Irinotecan (Camptosar) | Moderate | Irritant |
| Topotecan (Hycamtin) | Moderate | Irritant |
| Miscellaneous Agents | ||
| Arsenic trioxide (Trisenox) | Moderate | Not known |
| Asparaginase (Elspar) | Low | Vesicant |
| Hydroxyurea (Droxia, Hydrea) | Low | N/A (oral drug) |
| Ixabepilone (Ixempra) | Low—Moderate | Irritant |
| Pegaspargase (Oncaspar) | Low | Bruising |
Procarbazine (Matulane, Natulan  ) ) | High | N/A (oral drug) |
| Vorinostat (Zolinza) | Moderate | N/A (oral drug) |
Data from www.fda.gov/cder/index.html; and www.mdconsult.com/php/82925233-2/homepage.
Chemotherapy Drug Categories
Alkylating agents cross-link DNA, making the two DNA strands bind tightly together. This tight binding prevents proper DNA and ribonucleic acid (RNA) synthesis, which inhibit cell division.
Antimetabolites are similar to normal metabolites needed for vital cell processes. Most cell reactions require metabolites in order to begin or continue the reaction. Antimetabolites closely resemble normal metabolites and are “counterfeit” metabolites that fool cancer cells into using the antimetabolites in cellular reactions. Because antimetabolites cannot function as proper metabolites, their presence impairs cell division.
Antimitotic agents interfere with the formation and actions of microtubules so cells cannot complete mitosis during cell division. As a result, the cancer cell either does not divide at all or divides only once, resulting in two daughter cells that cannot continue to divide.
Antitumor antibiotics damage the cell’s DNA and interrupt DNA or RNA synthesis. Exactly how the interruptions occur varies with each agent.
Topoisomerase inhibitors disrupt an enzyme (topoisomerase) needed for DNA synthesis and cell division. The enzyme nicks and straightens the DNA helix, allowing the DNA to be copied, and then reattaches the DNA together. Topoisomerase inhibitors prevent proper DNA maintenance, causing DNA breakage and cell death.
Miscellaneous chemotherapy drugs are those with mechanisms of action that are either unknown or do not fit those of other drug categories.
Combination Chemotherapy
Successful cancer chemotherapy involves giving more than one specific anticancer drug in a timed manner. This technique is called combination chemotherapy. Using more than one drug is more effective in killing cancer cells than using only a single drug. However, the side effects and damage caused to normal tissues also increase with combination chemotherapy.
The selection of drugs is based on known tumor sensitivity to the drugs and the degree of side effects expected. For example, most chemotherapy drugs suppress bone marrow activity and immune function to some degree, but some agents cause more bone marrow suppression than others. There is also variation in the timing of drug-induced suppression and neutropenia.
The time when bone marrow activity and white blood cell counts are at their lowest levels after chemotherapy is the nadir. It occurs at different times for different drugs. To reduce immunosuppression, combination chemotherapy avoids using drugs with nadirs that occur at or near the same time.
Treatment Issues
Dosages for most chemotherapy drugs are calculated according to the type of cancer and the patient’s size. Usually, calculations are based on milligrams per square meter of total body surface area (TBSA), which considers both the patient’s height and weight.
Chemotherapy drugs are given on a regular basis and are timed to maximize cancer cell kill and minimize damage to normal cells. The schedule may vary somewhat to accommodate a patient’s response to therapy, but chemotherapy is usually scheduled every 3 to 4 weeks for a specified number of times (on average, 4 to 12 times). Newer protocols of giving higher doses of chemotherapy more often, called dose-dense chemotherapy, are often used for aggressive cancer treatment, especially for breast cancer. This dose-dense chemotherapy also results in more intense side effects than traditional dosing schedules.
Most chemotherapy drugs are given IV, although other routes may be used. For specific cancer types, the chemotherapy may be infused or instilled into a body cavity. The intrathecal route delivers drugs into the spinal canal, and the intraventricular route delivers drugs directly into the ventricles of the brain. Intraperitoneal instillations place the drugs within the abdominal cavity, most often for ovarian cancer (Karius, 2010). Drugs for bladder cancer can be instilled directly into the bladder (intravesicular route). For a few cancer types, intra-arterial infusions may be used to deliver a higher dose locally. This technique is not common and is used mostly for bone cancers and, on a limited basis, for head and neck cancer. The techniques and care needs for different routes are described with the specific cancer type most commonly associated with the specific administration route.
The IV route is the most preferred route for chemotherapy. The standard of care designated by the Oncology Nursing Society (ONS) and supported by the American Society of Clinical Oncologists (ASCO) for safe administration of IV chemotherapy is that administration of these drugs requires special education (Polovich et al., 2009). Special education for competency does not mean that only an advanced practice nurse can perform this function; however, it does mean that the person should be a registered nurse who has completed an approved chemotherapy course. Responsibility for monitoring the patient during chemotherapy administration, however, rests with all nurses providing patient care.
A serious complication of IV infusion is extravasation, which occurs when drug leaks into the surrounding tissues (also called infiltration). When the drugs given are vesicants (chemicals that damage tissue on direct contact), the results of extravasation can include pain, infection, and tissue loss (Fig. 24-3). Surgical intervention is sometimes needed for severe tissue damage. See Table 24-2 for a listing of known vesicant and irritant chemotherapy drugs.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


