Laura M. Dechant
Care of Patients with Acute Coronary Syndromes
Learning Outcomes
Safe and Effective Care Environment
Health Promotion and Maintenance
Psychosocial Integrity
Physiological Integrity
6 Compare and contrast the clinical manifestations of stable angina, unstable angina, and MI.
7 Interpret physical and diagnostic assessment findings in patients who have CAD.
8 Prioritize nursing care for patients who have chest pain.
9 Teach patients and families about drug therapy for CAD.
10 Explain the nursing care for patients who have thrombolysis for an MI.
11 Develop a plan of care for the patient who has a percutaneous transluminal coronary angioplasty.
13 Identify the special needs of older adults having coronary artery bypass graft (CABG) surgery.

http://evolve.elsevier.com/Iggy/
Animation: Acute Coronary Syndrome
Animation: Coronary Artery Bypass Graft
Answer Key for NCLEX Examination Challenges and Decision-Making Challenges
Audio Glossary
Concept Map Creator
Key Points
Review Questions for the NCLEX® Examination
Coronary artery disease (CAD), also called coronary heart disease (CHD) or simply heart disease, is the single largest killer of American men and women in all ethnic groups. When the arteries that supply the myocardium (heart muscle) are diseased, the heart cannot pump blood effectively to adequately perfuse vital organs and peripheral tissues. The organs and tissues need oxygen in arterial blood for survival. When oxygenation and perfusion are impaired, the patient can have life-threatening clinical manifestations and possibly death.
The incidence of CAD has declined over the past decade. This decline is due to many factors, including increasingly effective treatment and an increased awareness and emphasis on reducing major cardiovascular risk factors (e.g., hypertension, smoking, high cholesterol). Some coronary events occur in patients without traditional risk factors.
Pathophysiology
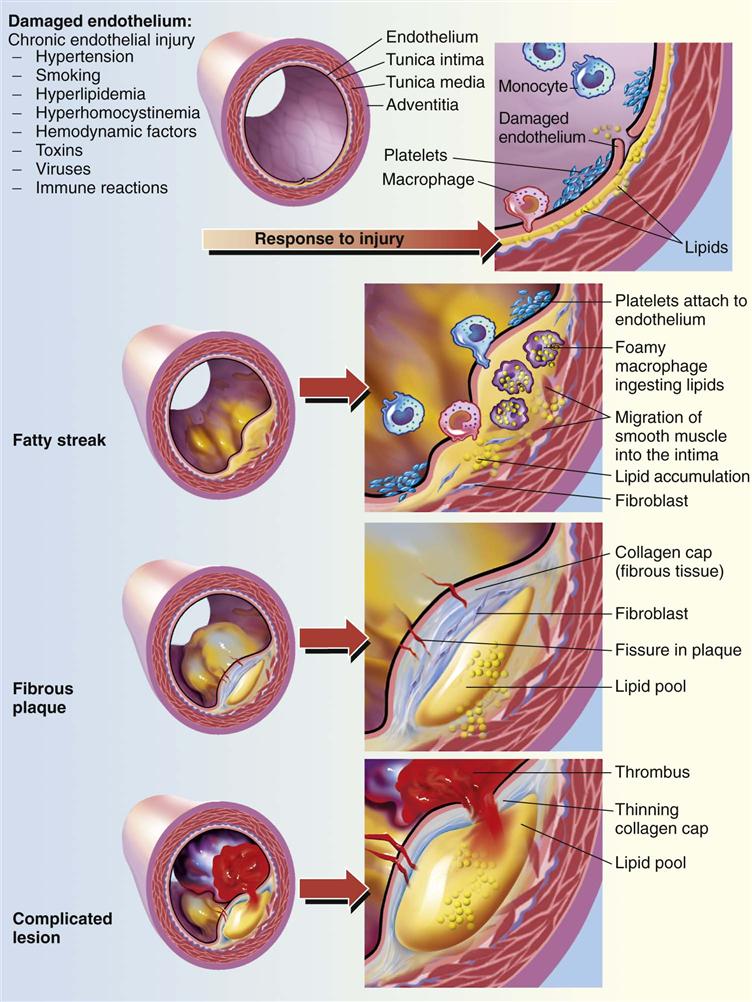
Coronary artery disease (CAD) is a broad term that includes chronic stable angina and acute coronary syndromes. It affects the arteries that provide blood, oxygen, and nutrients to the myocardium. When blood flow through the coronary arteries is partially or completely blocked, ischemia and infarction of the myocardium may result. Ischemia occurs when insufficient oxygen is supplied to meet the requirements of the myocardium. Infarction (necrosis, or cell death) occurs when severe ischemia is prolonged and decreased perfusion causes irreversible damage to tissue.
Chronic Stable Angina Pectoris
Angina pectoris is chest pain caused by a temporary imbalance between the coronary arteries’ ability to supply oxygen and the cardiac muscle’s demand for oxygen. Ischemia (lack of oxygen) that occurs with angina is limited in duration and does not cause permanent damage of myocardial tissue.
Angina may be of two main types: stable angina and unstable angina. Chronic stable angina (CSA) is chest discomfort that occurs with moderate to prolonged exertion in a pattern that is familiar to the patient. The frequency, duration, and intensity of symptoms remain the same over several months. CSA results in only slight limitation of activity and is usually associated with a fixed atherosclerotic plaque. It is usually relieved by nitroglycerin or rest and often is managed with drug therapy. Rarely does CSA require aggressive treatment. Unstable angina is discussed in the following Acute Coronary Syndromes section.
Acute Coronary Syndromes
The term acute coronary syndrome (ACS) is used to describe patients who have either unstable angina or an acute myocardial infarction. In ACS, it is believed that the atherosclerotic plaque in the coronary artery ruptures, resulting in platelet aggregation (“clumping”), thrombus (clot) formation, and vasoconstriction (Fig. 40-1). The amount of disruption of the atherosclerotic plaque determines the degree of coronary artery obstruction (blockage) and the specific disease process. The artery has to have at least 40% plaque accumulation before it starts to block blood flow.
Historically, an acute myocardial infarction (MI) was diagnosed by the presence of ST-segment elevation on the 12-lead electrocardiogram (ECG) (see discussion of the normal ECG in Chapter 36). However, all patients do not present with this finding. Instead, they are classified into one of three categories according to the presence or absence of ST-segment elevation on the ECG and positive troponin markers (see Chapter 35 for discussion of troponins):
• ST-elevation MI (STEMI) (traditional manifestation)
• Non–ST-elevation MI (NSTEMI) (common in women)
Unstable Angina Pectoris.
Unstable angina (the most commonly used term) is chest pain or discomfort that occurs at rest or with exertion and causes severe activity limitation. An increase in the number of attacks and in the intensity of the pressure indicates unstable angina. The pressure may last longer than 15 minutes or may be poorly relieved by rest or nitroglycerin. Unstable angina describes a variety of disorders, including new-onset angina, variant (Prinzmetal’s) angina, and pre-infarction angina. Patients with unstable angina will present with ST changes on a 12-lead ECG but will not have changes in troponin or creatine kinase (CK) levels.
New-onset angina describes the patient who has his or her first angina symptoms, usually after exertion or other increased demands on the heart. Variant (Prinzmetal’s) angina is chest pain or discomfort resulting from coronary artery spasm and typically occurs after rest. Pre-infarction angina refers to chest pain that occurs in the days or weeks before an MI.
Myocardial Infarction.
The most serious acute coronary syndrome is myocardial infarction (MI), often referred to as acute MI or AMI. Undiagnosed or untreated angina can lead to this very serious health problem. AMI is further divided by the American College of Cardiology (ACC)/AHA into non–ST-elevation MI (NSTEMI) and ST-elevation MI (STEMI) (Anderson, 2007). Patients presenting with NSTEMI typically have ST and T-wave changes on 12-lead ECG. This indicates myocardial ischemia. Cardiac enzymes may be initially normal but elevate over the next 6 to 12 hours. Patients presenting with STEMI typically have ST elevation in two contiguous leads on a 12-lead ECG. This indicates myocardial infarction/necrosis and requires immediate treatment.
Myocardial infarction (MI) occurs when myocardial tissue is abruptly and severely deprived of oxygen. When blood flow is quickly reduced by 80% to 90%, ischemia develops. Ischemia can lead to injury and necrosis of myocardial tissue if blood flow is not restored. Most MIs are the result of atherosclerosis of a coronary artery, rupture of the plaque, subsequent thrombosis, and occlusion (blockage) of blood flow. Other factors may be involved, however, such as coronary artery spasm, platelet aggregation, and emboli from mural thrombi (thrombi lining the walls of the cardiac chambers).
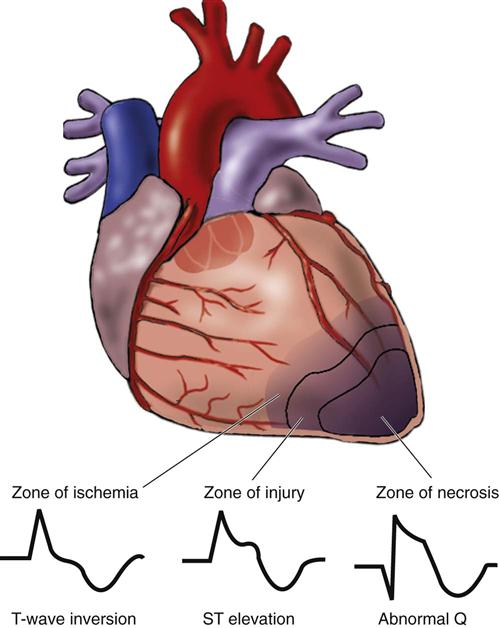
Often MIs begin with infarction of the subendocardial layer of cardiac muscle. This layer has the longest myofibrils in the heart, the greatest oxygen demand, and the poorest oxygen supply. Around the initial area of infarction (zone of necrosis) in the subendocardium are two other zones: (1) the zone of injury—tissue that is injured but not necrotic; and (2) the zone of ischemia—tissue that is oxygen deprived. This pattern is illustrated in Fig. 40-2.
Infarction is a dynamic process that does not occur instantly. Rather, it evolves over a period of several hours. Hypoxia (decreased oxygen) from ischemia may lead to local vasodilation of blood vessels and acidosis. Potassium, calcium, and magnesium imbalances, as well as acidosis at the cellular level, may lead to changes in normal conduction and contractile functions. Catecholamines (epinephrine and norepinephrine) released in response to hypoxia and pain may increase the heart’s rate, contractility, and afterload. These factors increase oxygen requirements in tissue that is already oxygen deprived. This may lead to life-threatening ventricular dysrhythmias. The area of infarction may extend into the zones of injury and ischemia. The actual extent of the zone of infarction depends on three factors: collateral circulation, anaerobic metabolism, and workload demands on the myocardium.
The infarction may involve only the subendocardium (called a subendocardial MI) or may spread to the epicardium or to all three layers of cardiac muscle. When all three layers are involved, the MI is termed transmural. Subendocardial MIs have less effect on wall motion and cardiac output than do transmural infarctions. When fewer grams of myocardium are affected, the characteristic “Q” wave on the ECG, which may also indicate an old infarction, may not appear.
Obvious physical changes do not occur in the heart until 6 hours after the infarction, when the infarcted region appears blue and swollen. These changes explain the need for intervention within the first 4 to 6 hours of symptom onset! After 48 hours, the infarcted area turns gray with yellow streaks as neutrophils invade the tissue and begin to remove the necrotic cells. By 8 to 10 days after infarction, granulation tissue forms at the edges of the necrotic tissue. Over a 2- to 3-month period, the necrotic area eventually develops into a shrunken, thin, firm scar. Scar tissue permanently changes the size and shape of the entire left ventricle, called ventricular remodeling. Remodeling may decrease left ventricular function, cause heart failure, and increase morbidity and mortality. The scarred tissue does not contract nor does it conduct electrically. Thus this area is often the cause of chronic ventricular dysrhythmias surrounding the infarcted zone.
The patient’s response to an MI also depends on which coronary artery or arteries were obstructed and which part of the left ventricle wall was damaged: anterior, septal, lateral, inferior, or posterior. Fig. 35-3 in Chapter 35 shows the location of the major coronary arteries.
Obstruction of the left anterior descending (LAD) artery causes anterior or septal MIs because it perfuses the anterior wall and most of the septum of the left ventricle. Patients with anterior wall MIs (AWMIs) have the highest mortality rate because they are most likely to have left ventricular failure and dysrhythmias from damage to the left ventricle.
The circumflex artery supplies the lateral wall of the left ventricle and possibly portions of the posterior wall or the sinoatrial (SA) and atrioventricular (AV) nodes. Patients with obstruction of the circumflex artery may experience a posterior wall MI (PWMI) or a lateral wall MI (LWMI) and sinus dysrhythmias.
In most people, the right coronary artery (RCA) supplies most of the SA and AV nodes, as well as the right ventricle and inferior or diaphragmatic portion of the left ventricle. Patients with obstruction of the RCA often have inferior wall MIs. About half of all inferior wall MIs are associated with an occlusion of the RCA causing significant damage to the right ventricle. Thus it is important to obtain a “right-sided” ECG to assess for right ventricular involvement.
Etiology and Genetic Risk
Atherosclerosis is the primary factor in the development of CAD. Numerous risk factors contribute to atherosclerosis and subsequently to CAD (also see Chapter 38).
Nonmodifiable risk factors are personal characteristics that cannot be altered or controlled. These risk factors, which interact with each other, include age, gender, family history, and ethnic background. People with a family history of CAD are at high risk for developing the disease. These factors are discussed in more detail in Chapter 35.
Modifiable risk factors are lifestyle choices that can be controlled by the patient, such as smoking and obesity. These factors are described later in the Health Promotion and Maintenance section of this chapter.
Incidence/Prevalence
According to the American Heart Association (AHA) (2010), 64% of women and 50% of men who had a myocardial infarction (MI) (“heart attack”) were not aware that they had CAD. The average age of a person having a first MI is 64.5 years for men and 70.3 years for women (AHA, 2010). Almost 30% of patients who have an MI die within 5 years after the event (AHA, 2010).
Every 25 seconds, a person in the United States has a major coronary event and 452,000 people die each year from an MI. Many people die from coronary heart disease without being hospitalized. Most of these are sudden deaths caused by cardiac arrest (AHA, 2010).
Many patients who survive MIs are not able to return to work. CAD is the leading cause of premature, permanent disability in the United States, accounting for about 20% of disability allowances by the Social Security Administration.
Health Promotion and Maintenance
Ninety-five percent of sudden cardiac arrest victims die before reaching the hospital, largely because of ventricular fibrillation (“v fib”). To help combat this problem, automatic external defibrillators (AEDs) are found in many public places, such as in shopping centers and on airplanes. Employees are taught how to use these devices if a sudden cardiac arrest occurs. Some patients with diagnosed CAD have AEDs in their homes or at work. How to use this device is described on p. 738 in Chapter 36.
Health promotion efforts are directed toward controlling or altering modifiable risk factors for CAD. Some of these factors have a genetic basis, which is described elsewhere in this text. Common risk factors include:
 Nursing Safety Priority
Nursing Safety Priority
Action Alert
For patients at risk for coronary artery disease (CAD), especially MI, assess specific risk factors and implement an individualized health teaching plan. Teach people who have one or more of these risk factors the importance of modifying or eliminating them to decrease their chances of CAD (Chart 40-1).
 Cultural Awareness
Cultural Awareness
Several groups have a higher genetic risk for CAD than others. African-American and Hispanic women have higher CAD risk factors than white women of the same socioeconomic status. Of American Indians and Alaskan Natives 18 years of age and older, about 64% of men and 81% of women have one or more CAD risk factors (hypertension [HTN], smoking, high cholesterol, excess weight, or diabetes mellitus). The leading cause of death for both men and women in the Euro-American population is cardiac disease, even though they may not have genetic predispositions to developing cardiovascular risk factors (AHA, 2010).
Reducing Elevated Serum Lipid Levels
The risk for CAD rises as serum cholesterol and triglyceride levels increase. In addition to measuring the total serum cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), and triglyceride (TG) levels are important in assessing risk for CAD. LDL cholesterol is the “bad” type, and HDL cholesterol is referred to as “good” because it has protective properties. Elevated levels of LDL combined with low levels of HDL increase the risk for MI. Total serum cholesterol levels also put the patient at a higher risk for developing an MI. According to the AHA (2010), a 10% reduction in serum cholesterol may result in a 30% reduction in the incidence of CAD and MI. The fasting total cholesterol should be below 130 mg/dL. The AHA (2010) defines levels of fasting total cholesterol as:
The desired LDL level in patients who are at high risk or have existing CAD is less than 70 mg/dL. For patients at low or moderate risk, LDL should also be substantially less than 100 mg/dL (AHA, 2010). HDL cholesterol levels should be above 40 mg/dL, although this recommendation may soon be changed to a higher level. The recommended triglyceride level is less than 135 mg/dL in women and 150 mg/dL in men (Pagana & Pagana, 2010).
Approaches to decrease lipids are focused on diet, exercise, and drug therapy that lowers cholesterol and triglyceride levels. Teach patients with elevated lipid levels to:
Using Complementary and Alternative Therapies
Teach patients that adding omega-3 fatty acids from fish and plant sources has been effective for some patients in reducing lipid levels, stabilizing atherosclerotic plaques, and reducing sudden death from an MI. The preferred source of omega-3 acids is from fish three times a week or a daily fish oil nutritional supplement (1-2 g/day) containing eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) (AHA, 2010). Plant sources (flaxseed, flaxseed oil, walnuts, and canola oil) contain α-linolenic acid, and the conversion of α-linolenic acid to EPA and DHA is not as efficient in patients who consume a typical Western diet (Surette, 2008). Lovaza (omega-3 fatty acids) is a new medication approved by the Federal Drug Administration (FDA) and is used to reduce very high triglycerides (>500 mg/dL) levels. Lovaza has not been proven to prevent heart attacks or stroke.
Garlic supplements may also have a small effect on reducing lipid levels, but they have not been shown to prevent MI. Patients often take a number of other supplements, such as vitamin E, coenzyme Q10, Pantesin, and vitamin B complex to decrease the risk for heart disease. None of these substances has been found to be helpful in reducing coronary artery disease.
Eliminating Tobacco Use
In the United States, an estimated 23% of men and 18% of women smoke cigarettes, putting them at increased risk for MI (AHA, 2010). About five million U.S. men and women chew tobacco, with the highest rates in the South and rural areas. Tobacco use and passive smoking from “second-hand smoke” (also called environmental smoke) substantially reduce blood flow in the coronary arteries.
Tobacco use, especially cigarette smoking, accounts for over one third of deaths from CAD. It enhances the process of atherosclerosis through mechanisms that are still poorly understood. Nicotine begins the release of catecholamines, resulting in an increased heart rate and peripheral vasoconstriction. This action causes increases in blood pressure (BP), cardiac afterload, and oxygen consumption. Cigarette smoking has also been found to cause endothelial dysfunction and increased vessel wall thickness. This process increases the risk for clot formation and vessel occlusion. The resulting hypertension may exacerbate the atherosclerotic process by increasing vessel wall permeability. Another problem with cigarette smoking is the production of carbon monoxide, which has been found to decrease the oxygen content in arterial blood. The good news is that when cigarette smoking is stopped, the risk for CAD decreases. A person who stops smoking may decrease the risk for CAD by as much as 80% in 1 year. Reducing the tar and nicotine content of the cigarettes smoked does not reduce the risk for CAD (AHA, 2010).
Ask about tobacco use, and advise the tobacco user and family members who smoke to quit using this harmful substance. Teach all patients to avoid environmental tobacco smoke at work and at home if at all possible. Additional information about tobacco use and smoking cessation is found in Chapters 32 and 35.
Increasing Physical Activity
Physical inactivity may be the most important risk factor for the general population. Less-active, less-fit people have a 30% to 50% greater risk for developing high blood pressure (BP), which predisposes to CAD. Physical inactivity is more common among women than men, among African Americans and Hispanics than Euro-Americans, among older adults than younger adults, and among the less affluent than the more affluent (AHA, 2010). The causes for these differences are not known. Teach patients that regular physical activity helps maintain body weight and muscle mass while improving BP and lipid values.
Moderate-intensity activities like walking are associated with a major reduction in CAD risk. However, intense exercising may contribute to plaque rupture and increase the number of cardiac episodes. Teach people that participating in exercise for 30 minutes a day can reduce hypertension and increase secretions of endorphins. It also leads to decreased smoking and eating, improved metabolism, and a stronger feeling of well-being. Other benefits include decreased blood clotting and higher plasma HDL levels, increased heart volume, increased cardiac capillary blood flow, and decreased heart rate. Physical activity does not increase collateral circulation or reduce the size of existing plaques.
Managing Other Factors
One in three Americans has hypertension (HTN). This disease increases the workload of the heart, which increases the risk for MI. The cause of primary HTN is not known. However, it is easily detected and usually controllable. About half of patients having a first MI have a BP greater than 160/95 mm Hg. Ways to manage hypertension and therefore reduce the risk for CAD are described in Chapter 38.
Diabetes mellitus (DM) is a major risk factor for heart disease. A woman with diabetes mellitus is twice as likely to develop CAD than a woman without DM. Heart disease is the leading cause of diabetic-related death in both men and women. Most adults with diabetes also have hypertension. Chapter 67 discusses vascular complications of diabetes in detail.
Obesity is strongly associated with the development of hypertension, diabetes, and increased serum lipid levels. Women with fat deposited around their waists are at the highest risk for CAD. Teach the importance of weight management to help prevent these chronic and potentially life-threatening diseases.
Alcohol may help prevent or contribute to the development of CAD, depending on the amount consumed. Excessive consumption, described as having more than 3 ounces (90 mL) per day, can lead to increased heart disease, hypertension, and metabolic syndrome, described in the next section. A lower amount may help prevent CAD (Suzuki et al., 2009).
 Cultural Awareness
Cultural Awareness
Modifiable risk factors vary for people of different racial and ethnic backgrounds. Some of the differences may be explained by lack of access to health care for some groups or by genetic factors. American Indians, for example, have the highest percentage of smokers among women and men. However, many of these people have poor access to care or have language barriers in a predominantly English-speaking, Euro-American health care system. Nutritional preferences may also explain some of the differences. For instance, according to the AHA (2010), high cholesterol is more common in African-American and Hispanic populations. Diets higher in fat and cholesterol are often less expensive and may be a factor in explaining differences, and obesity is more common in these groups. Genetic factors may also contribute to the differences among ethnic groups.
A person’s response to emotional stress may also be associated with heart disease. Work stress, in particular, may be associated with left ventricular hypertrophy. During times of stress, increased heart rate increases the work of the heart, thus causing changes in the left ventricle.
Metabolic syndrome, also called syndrome X, has been recognized as a risk factor for cardiovascular (CV) disease and is being aggressively researched. Patients who have three of the factors in Table 40-1 are diagnosed with metabolic syndrome. This health problem increases the risk for developing diabetes and CAD. About 47 million people in the United States have metabolic syndrome (AHA, 2010). This increase is likely due to physical inactivity and the current obesity epidemic. Management is aimed at reducing risks, managing hypertension, and preventing complications.
TABLE 40-1
INDICATORS OF RISK FACTORS FOR METABOLIC SYNDROME
| RISK FACTOR | INDICATOR |
| Hypertension | Either blood pressure of 130/85 mm Hg or higher or taking antihypertensive drug(s) |
| Decreased HDL-C (usually with high LDL-C) level | Either HDL-C <40 mg/dL for men or <50 mg/dL for women or taking an anticholesterol drug |
| Increased level of triglycerides | Either 150 mg/dL or higher or taking an anticholesterol drug |
| Increased fasting blood glucose (due to diabetes, glucose intolerance, or insulin resistance) | Either 100 mg/dL or higher or taking antidiabetic drug(s) |
| Large waist size (excessive abdominal fat causing central obesity) | 40 inches (102 cm) or greater for men or 35 inches (89 cm) or greater for women |
HDL-C, High-density lipoprotein–cholesterol; LDL-C, low-density lipoprotein–cholesterol.
Elevated levels of serum homocysteine, an amino acid, have been associated with an increased incidence of CAD. However, research findings are not consistent regarding its risk. Vitamin B supplements have been thought to decrease homocysteine. Recent studies suggest that vitamin B is not effective as secondary prevention, but few studies have been conducted on vitamin B as a primary preventive measure (Ebbing et al., 2008).
Patients with multiple modifiable risk factors have several times the risk for CAD as those without these characteristics. Although many factors place a person at risk for heart disease, there are well-documented, effective ways of promoting cardiovascular health. The most important interdisciplinary intervention is health teaching.
 NCLEX Examination Challenge
NCLEX Examination ChallengePatient-Centered Collaborative Care
Assessment
History
If symptoms of CAD are present at the time of the interview, delay collecting data until interventions for symptom relief, vital sign instability, and dysrhythmias are started and discomfort resolves. If the patient had pain, ask about how he or she has managed the discomfort and other symptoms and which drugs he or she may be taking. When the patient is pain-free, obtain information about family history and modifiable risk factors, including eating habits, lifestyle, and physical activity levels. Ask about a history of smoking and how much alcohol is consumed each day. Collaborate with the dietitian to assess current body mass index (BMI) and weight.
Physical Assessment/Clinical Manifestations
Rapid assessment of the patient with chest pain or other presenting symptoms is crucial. It is important to differentiate among the types of chest pain and to identify the source. Question the patient to determine the characteristics of the discomfort. Patients may deny pain, however, and report that they feel “pressure.” Appropriate questions to ask concerning the discomfort include onset, location, radiation, intensity, duration, and precipitating and relieving factors.
 Cultural Awareness
Cultural Awareness
African Americans and women tend to delay seeking treatment for MI and therefore have higher mortality rates than Euro-Americans. One contributing factor to this delay is a greater incidence of dyspnea as an acute symptom among these groups rather than the classic pain more typical of other groups (AHA, 2010).
If pain is present, ask the patient if the pain is in the chest, epigastric area, jaw, back, shoulder, or arm. Ask him or her to rate the pain on a scale of 0 to 10, with 10 being the highest level of discomfort. Some patients describe the discomfort as tightness, a burning sensation, pressure, or indigestion.
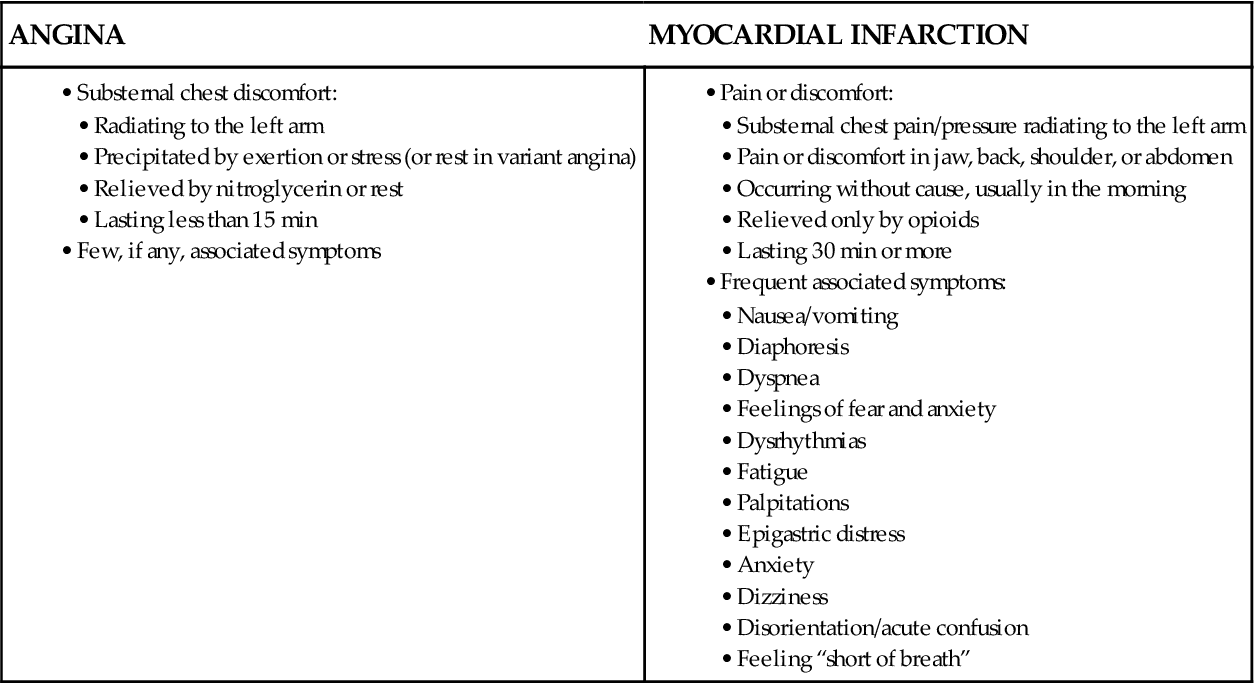
Chart 40-2 compares and contrasts angina and infarction pain. Because angina pain is ischemic pain, it usually improves when the imbalance between oxygen supply and demand is resolved. For example, rest reduces tissue demands and nitroglycerin improves oxygen supply. Discomfort from a myocardial infarction (MI) does not usually resolve with these measures. Also ask about any associated symptoms, including nausea, vomiting, diaphoresis, dizziness, weakness, palpitations, and shortness of breath.
Chart 40-2
Key Features
Angina and Myocardial Infarction
| ANGINA | MYOCARDIAL INFARCTION |
Assess blood pressure and heart rate. Interpret the patient’s cardiac rhythm and presence of dysrhythmias. Sinus tachycardia with premature ventricular contractions (PVCs) frequently occurs in the first few hours after an MI.
Next assess distal peripheral pulses and skin temperature. The skin should be warm with all pulses palpable. In the patient with unstable angina or MI, poor cardiac output may be manifested by cool, diaphoretic (“sweaty”) skin and diminished or absent pulses. Auscultate for an S3 gallop, which often indicates heart failure—a serious and common complication of MI. Assess the respiratory rate and breath sounds for signs of heart failure. An increased respiratory rate is common because of anxiety and pain, but crackles or wheezes may indicate left-sided heart failure. An S4 heart sound is a common finding in the patient who has had a previous MI or hypertension. Assess for the presence of jugular venous distention and peripheral edema.
The patient with MI may experience a temperature elevation for several days after infarction. Temperatures as high as 102° F (38.9° C) may occur in response to myocardial necrosis, indicating the inflammatory response.
Psychosocial Assessment
Denial is a common early reaction to chest discomfort associated with angina or MI. On average, the patient with an acute MI waits more than 2 hours before seeking medical attention. Often he or she rationalizes that symptoms are due to indigestion or overexertion. In some situations, denial is a normal part of adapting to a stressful event. However, denial that interferes with identifying a symptom such as chest discomfort can be harmful. Explain the importance of reporting any discomfort to the health care provider.
Fear, depression, anxiety, and anger are other common reactions of many patients and their families. Assist in identifying these feelings. Encourage them to explain their understanding of the event, and clarify any misconceptions.
Laboratory Assessment
Although there is no single ideal test to diagnose MI, the most common laboratory tests include troponins T and I, creatine kinase-MB (CK-MB), and myoglobin. These cardiac markers are specific for MI and cardiac necrosis. Troponins T and I and myoglobin rise quickly. CK-MB is the most specific marker for MI but does not peak until about 24 hours after the onset of pain. These tests are described in more detail in Chapter 35.
Imaging Assessment
Unless there is associated cardiac dysfunction (e.g., valve disease) or heart failure, a chest x-ray is not diagnostic for angina or MI.
Thallium scans use radioisotope imaging to assess for ischemia or necrotic muscle tissue related to angina or myocardial infarction (MI). Areas of decreased or absent perfusion, referred to as cold spots, identify ischemia or infarction. Thallium may be used with the exercise tolerance test. Dipyridamole (Persantine) thallium scanning (DTS) may also be used.
Contrast-enhanced cardiovascular magnetic resonance (CMR) may also be done as a noninvasive approach to detect MI. Echocardiography may be used to visualize the structures of the heart.
Use of the 64-slice computed tomography coronary angiography (CTCA) has been found to be helpful in diagnosing coronary artery disease in symptomatic patients identified as having a “low- or intermediate-pretest probability” risk for CAD. This new generation of high-speed computed tomography (CT) scanners is becoming a highly reliable, noninvasive way to evaluate CAD (Weustink et al., 2010).
Other Diagnostic Assessment
Twelve-lead electrocardiograms (ECGs) allow the health care provider to examine the heart from varying perspectives. By identifying the lead(s) in which ECG changes are occurring, the health care provider can identify both the occurrence and the location of ischemia (angina) or necrosis (infarction). In addition to the traditional 12-lead ECG, the health care provider may request a “right-sided” or 18-lead ECG to determine whether ischemia or infarction has occurred in the right ventricle.
An ischemic myocardium does not repolarize normally. Thus 12-lead ECGs obtained during an angina episode reveal ST depression, T-wave inversion, or both. Variant angina, caused by coronary vasospasm (vessel spasm), usually causes elevation of the ST segment during angina attacks. These ST and T-wave changes usually subside when the ischemia is resolved and pain is relieved. However, the T wave may remain flat or inverted for a period of time. If the patient is not experiencing angina at the moment of the test, the ECG is usually normal unless he or she has evidence of an old MI.
When infarction occurs, one of three ECG changes is usually observed: ST-elevation MI (STEMI), T-wave inversion, or non–ST-elevation MI (NSTEMI). An abnormal Q wave (wider than 0.04 seconds or more than one-third the height of the QRS complex) may develop, depending on the amount of myocardium that has necrosed. Women having an MI often present with an NSTEMI or T-wave inversion.
The Q wave may develop because necrotic cells do not conduct electrical stimuli. Hours to days after the MI, the ST-segment and T-wave changes return to normal. However, when the Q wave exists, it may become permanent. The Q waves may disappear after a number of years, but their absence does not necessarily mean that the patient has not had an MI.
After the acute stages of an angina episode or MI, the health care provider often requests an exercise tolerance test (stress test) on a treadmill to assess for ECG changes consistent with ischemia, evaluate medical therapy, and identify those who might benefit from invasive therapy. Pharmacologic stress-testing agents such as dobutamine (Dobutrex) may be used instead of the treadmill. Treadmill exercise testing is only moderately accurate for women when compared with men (Bellasi et al., 2007). In women with suspected CAD, stress echocardiography or single photon emission computed tomography (SPECT) should be performed.
Cardiac catheterization may be performed to determine the extent and exact location of coronary artery obstructions. It allows the cardiologist and cardiac surgeon to identify patients who might benefit from percutaneous transluminal coronary angioplasty (PTCA) and stent placement or from coronary artery bypass grafting (CABG). Each of the diagnostic tests in this section is described in detail in Chapter 35.
Analysis
The patient with coronary artery disease (CAD) may have either angina or MI. If MI is suspected or cannot be completely ruled out, the patient is admitted to a telemetry unit for continuous monitoring or to a critical care unit if hemodynamically unstable.
The priority problems for most patients with CAD are:
1 Acute Pain related to imbalance between myocardial oxygen supply and demand
2 Inadequate tissue perfusion (cardiopulmonary) related to interruption of arterial blood flow
3 Activity Intolerance related to fatigue caused by imbalance between oxygen supply and demand
4 Ineffective Coping related to effects of acute illness and major changes in lifestyle
For the patient experiencing an MI, additional problems include:
Planning and Implementation
Astute assessment skills, timely analysis of troponin, and analysis of the 12-lead ECG (or 18-lead ECG for a suspected right ventricular infarction) are essential to ensure appropriate patient care management. This is particularly important since the average time a patient waits before seeking treatment is 2 hours and 20 minutes. This delay lessens the 4- to 6-hour window of opportunity for the most advantageous treatment with percutaneous intervention.
Managing Acute Pain
Patients with diabetes mellitus and coronary artery disease (CAD) may not experience chest pain or pressure because of diabetic neuropathy. In this patient population, the onset of acute myocardial infarction (AMI) may be signaled by new onset of atrial fibrillation. With new-onset atrial fibrillation, a cardiac workup should be done to rule out myocardial infarction.
Planning: Expected Outcomes.
The expected outcome is that the patient will verbalize a report of decreased pain and discomfort as a result of prompt collaborative interventions.
Interventions.
The purpose of patient-centered collaborative care is to eliminate discomfort by providing pain relief measures, decreasing myocardial oxygen demand, and increasing myocardial oxygen supply.
Emergency Care.
Evaluate any report of pain, obtain vital signs, ensure an IV access, and notify the health care provider of the patient’s condition. Chart 40-3 summarizes the emergency interventions for the patient with symptoms of CAD.
Pain relief helps increase the oxygen supply and decrease myocardial oxygen demand. The American Heart Association (AHA) recommends several pain management strategies, including morphine sulfate and oxygen. Give morphine as the priority in managing pain in patients having an MI!
Drug Therapy.
At home or in the hospital, the patient may take nitroglycerin to relieve episodic anginal pain. Aspirin 325 mg, an antiplatelet drug, may also be taken daily to prevent clots that further block coronary arteries.
Nitroglycerin (NTG), a nitrate often referred to as “nitro,” increases collateral blood flow, redistributes blood flow toward the subendocardium, and dilates the coronary arteries. In addition, it decreases myocardial oxygen demand by peripheral vasodilation, which decreases both preload and afterload. Teach the patient to hold the tablet under the tongue and drink 5 mL of water, if necessary, to allow the tablet to dissolve. NTG spray is also available and is more quickly absorbed. Pain relief should begin within 1 to 2 minutes and should be clearly evident in 3 to 5 minutes. After 5 minutes, recheck the patient’s pain intensity and vital signs. If the BP is less than 100 mm Hg systolic or 25 mm Hg lower than the previous reading, lower the head of the bed and notify the health care provider. If the patient is experiencing some but not complete relief and vital signs remain stable, another NTG tablet or spray may be used. In 5-minute increments, a total of three doses may be administered in an attempt to relieve angina pain. If the patient uses NTG spray instead of the tablet, teach him or her to sit upright and spray the dose under the tongue. NTG topical patches should be placed below the nipple line to decrease discomfort.
Angina usually responds to NTG. The patient typically states that the pain is relieved or markedly diminished. When simple measures, such as taking three sublingual nitroglycerin tablets one after the other, do not relieve chest discomfort, the patient may be experiencing an MI.
 Nursing Safety Priority
Nursing Safety Priority
Critical Rescue
If the patient is experiencing an MI, prepare the patient for transfer to a specialized unit where close monitoring and appropriate management can be provided. If the patient is at home or in the community, call 911 for transfer to the closest emergency department.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


