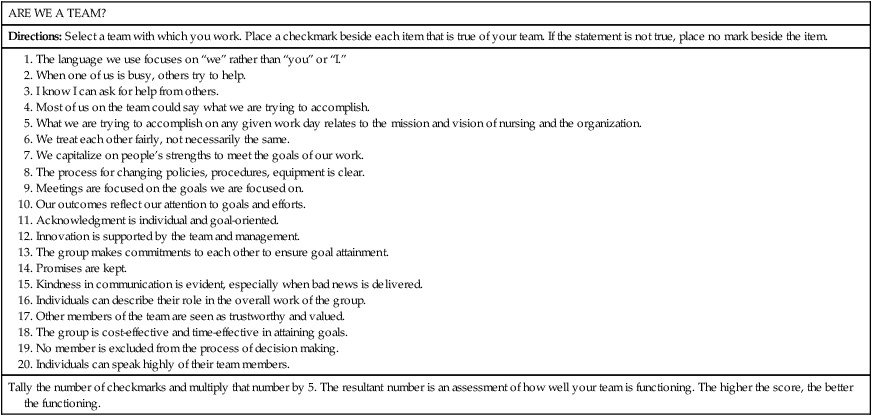
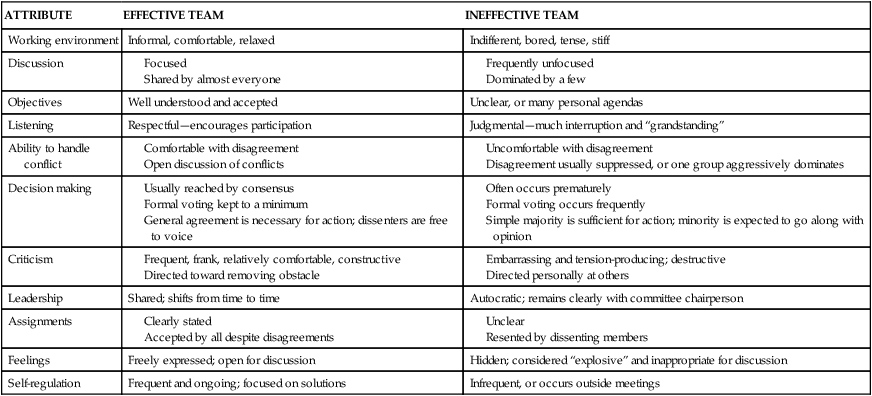
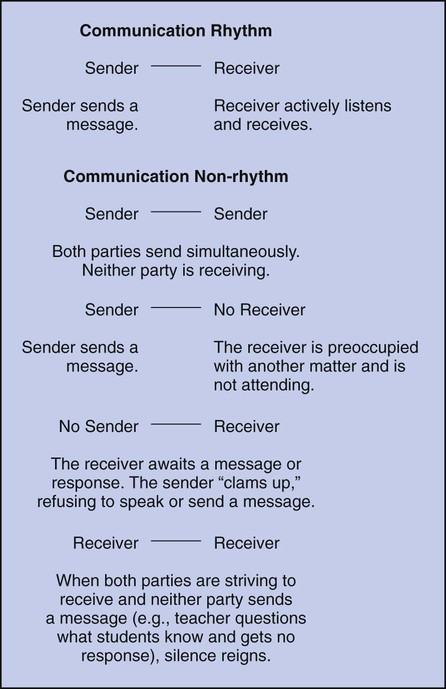
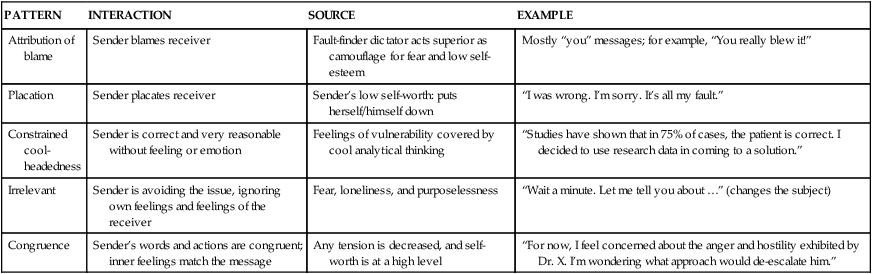
• Evaluate the differences between a group and a team. • Value four key concepts of teams. • Demonstrate an effective communication interaction. • Identify at least five communication pitfalls. • Apply the guidelines for acknowledgment to a situation in your clinical setting. • Compare a setting that uses the “rules of the game” with your current clinical setting. • Develop an example of a team that functions synergistically, including the results such a team would produce. • Discuss the importance of team to patient safety and quality. In our society, in which so much emphasis is placed on the individual and individual achievement, teamwork is the quintessential contradiction. In other words, with all the focus on individuals, we still need individuals to work together in groups to accomplish goals and keep patients safe. Everybody knows and understands this, particularly individuals who spend their Sundays watching football or basketball. These team sports are premier models of cooperation and competition. They are the model for teamwork for business today, and they represent a group following their respective leader or “coach” (Parcells, 2000). A group of people does not constitute a team. From Davis and Sharon’s perspective (2002), a team is a group of people with a high degree of interdependence geared toward the achievement of a goal or a task. Often, we can recognize intuitively when the so-called team is not functioning effectively. We say things such as, “We need to be more like a team” or “I’d like to see more team players around here.” Consequently, in the process of defining team, effective versus ineffective teams should be considered. Teams are groups that have defined objectives, ongoing positive relationships, and a supportive environment and that are focused on accomplishing a specific task. Teams are essential in providing cost-effective, high-quality health care. As resources are expended more prudently, patient care teams must develop clearly defined goals, use creative problem solving, and demonstrate mutual respect and support. Facilities with ineffective teams will find themselves out of business. Exercise 18-1 Think of the last team or group of which you were a part. Think about what went on in that team or group. Specifically think about what worked for you and what did not work. Use the “Team Assessment Exercise” in Table 18-1 to assess aspects of your team more specifically. Address each of the identified areas and discover how well your team or group functioned. Think about roles, activities, relationships, and general environment. Consider examples of shared decision making, shared leadership, shared accountability, and shared problem solving. These are the concepts that can be used to evaluate the functioning of almost any team of which you are a member. TABLE 18-1 ©The Wise Group, 2007, Lubbock, Texas. When a team functions effectively, a significant difference is evident in the entire work atmosphere, the way in which discussions progress, the level of understanding of the team-specific goals and tasks, the willingness of members to listen, the manner in which disagreements are handled, the use of consensus, and the way in which feedback is given and received. The original work done by McGregor (1960) sheds light on some of these significant differences, which are summarized in Table 18-2. TABLE 18-2 ATTRIBUTES OF EFFECTIVE AND INEFFECTIVE TEAMS Adapted from McGregor, D. (1960). The human side of enterprise. New York: McGraw-Hill. The challenges encountered in today’s healthcare systems are prodigious. Patient safety issues are at the forefront. Ongoing rounds of downsizing, budget cuts, declining patient days, reduced payments, and staff layoffs abound. Effective teams participate in effective problem solving, increased creativity, and improved health care. The effects of smoothly functioning teams on patient safety and the creation of a just culture are critically important, and one tool set to address these issues, including communication, can be found in the Literature Perspective on p. 349. • Model the Way—Credibility is the foundation of leadership. It is established by consistently Doing What You Say You Will Do or by Setting the Example for the other team members. • Inspire a Shared Vision—Imagine exciting and ennobling possibilities, and enlist others in these dreams through positive attitude, excitement, and hard work. • Challenge the Process—Seek innovative ways to change, grow, and improve—experiment and take risks. • Enable Others to Act—Foster collaboration by promoting cooperation and building trust. Create a sense of reciprocity or give and take. Establish a sense of “We’re all in this together.” • Encourage the Heart—Novice leaders encourage their constituents to carry on. They keep hope and determination alive, recognize contributions, and celebrate victories. It is not unusual today to have team members from four different generations of workers: Veterans, Baby Boomers, Generation X, and Generation Y. Because the workforce is aging, there may be a preponderance of Baby Boomers and Generation Xers in a work setting. Each generation, traditionally interpreted as a span of 20 years, grew up in a different era and was influenced by different historical events and cultural developments (Weingarten, 2009). For example, Veterans live by the rules and do not question authority. Boomers lived through the Cold War and were influenced by the assassinations of President Kennedy, Senator Robert Kennedy, and Martin Luther King, Jr.; the Civil Rights movement; and the Women’s Rights movement. Generation X nurses were often the “latch-key kids” because both parents worked outside the home. Divorce was common, and job stability was no longer guaranteed. Generation Y nurses are the future of the profession and have grown up with massive amounts of information and technology. They have experienced terrorism and natural disasters. They are culturally diverse and view education as the key to success. Efforts to understand and bridge these differences can be the difference between a dysfunctional and an effective team. Chapter 3 provides more detail about these differences. Communication in the work environment is not only important to good working conditions that retain nurses but also critical to reduction of medical errors (American Association of Critical-Care Nurses [AACN] & VitalSmarts, 2005; Arford, 2005). Because of such issues, new graduates go through a facility orientation, which emphasizes communication skills. Many nurses view this as a waste of time that could be used to further technical skills; however, at evaluation time, communication skills are often seen as a significant area for improvement (Buckman, Korsch, Baile, & Jason, 2000; Weiner, Barnet, Cheng, & Daaleman, 2005). The only thing human beings do more often than communicate is breathe. Communication is the most important component of daily activities. It is essential to clinical practice, to building teams, and to leadership. A person cannot not communicate. Because communication consists of both verbal and nonverbal signals, humans are continuously communicating not just thoughts, ideas, and opinions but also feelings and emotions (Morreale, Spitzberg, & Barge, 2001). Once the message is sent, it cannot be retracted; it can be amended, but the first impression of the communication usually is lasting. However, as important as this initial impression is, it is often an unconscious response or reaction. How we communicate is also a reflection of self-worth: Once a human being has arrived on this earth, communication is the largest single factor determining what kinds of relationships she or he makes with others and what happens to each in the world (Satir, 1988). Self-worth is a major influence in all communication. Stress results whenever self-worth is threatened. A basic model of communication patterns between the sender and the receiver is found in Figure 18-1. Effective communication develops a rhythm in which messages are sent and received in a productive, respectful, and supportive manner (Nemeth, 2008). Communication begins to break down as the rhythm is disrupted. The sender-receiver pattern disintegrates into a non-rhythmic event, as described in Figure 18-1. When non-rhythmic patterns develop, the participants may feel disrespected, upset, and even fearful. In her classic work, Satir (1988) identified the connection between stress and self-worth that can evolve as a result of a breakdown in communication. She defined stress as a threat to positive self-worth. Human beings tend to feel stress or anxiety whenever there is an unconscious linking of feelings, behaviors, or comments from others to a lowering of self-esteem or an attack on self-worth. A conscious effort ought to be made to relieve stress through activities such as ensuring specific/scheduled quiet time, requesting peer support, keeping a journal, treating yourself to something special, or going for a walk (Weiss, 2001). When this threat is identified, the receiver often reacts using one of the five communication patterns: attribution of blame, placation, constrained cool-headedness, immaterial irrelevance, or congruence (Bradley & Edinberg, 1990; Satir, 1988). Each pattern interaction and the source of the interaction are described with examples of each pattern in Table 18-3. The pattern that produces effective communication, the one to strive for, is congruence. Congruent communication occurs when both the verbal and nonverbal actions fit the inner feelings of the sender and are appropriate to the context of the message. This communication pattern creates the kind of connection between the sender and the receiver that fosters respect, support, and the creation of relationship. TABLE 18-3 Adapted from Satir, V. (1988). The new peoplemaking. Mountain View, CA: Science & Behavior Books; and Bradley, J., & Edinberg, M. (1990). Communication in the nursing context (3rd ed.). Norwalk, CT: Appleton & Lange. In today’s busy world, many interruptions and interferences to clear, focused, effective communication create breakdowns. According to Olen (1993), to be aware of these potential problems allows both sender and receiver to be prepared to minimize such barriers. • Distractions: Distractions most commonly come through sensory perceptions, such as poor lighting or background noise, including music, talking, ringing phones, and interruptions by others. Papers, reports, and heavy workloads can also be distracting. • Inadequate knowledge: The sender and receiver may be at different levels of knowledge, particularly in this time of highly specialized and technical knowledge bases. For multiple reasons, one person may not seek clarity from the other. • Poor planning: The process of organizing, planning, and clearly thinking through what needs to be communicated is very helpful. If the interaction is more spontaneous, it can more easily fall into a non-rhythmic pattern. • Differences in perception: Both the sender and the receiver have their individual mental filters—the way in which they see the world. Because of this individuality, no two filters are the same. Thus the same message is interpreted differently. Add to this, for example, sociocultural, ethnic, and educational differences, and it is easy to see how these differences can occur. • Emotions and personality: Someone who is experiencing distress may not be able to receive another message or may have difficulty keeping his or her emotions out of an unrelated message. Most humans, at some point, bring distress or problems from home to the workplace. If these remain unconscious, they can influence the work setting in a negative or nonproductive way. Effective communication suggests that the interaction is a rhythmic pattern that is respectful and clear, promotes trust, and encourages the expression of feelings and viewpoints. On the other hand, pitfalls in communication comprise actions, behaviors, and words that create distrust, are dishonoring, and decrease the feelings of self-worth in the receiver. Box 18-1 lists the major pitfalls of communication. These pitfalls lead to communication breakdowns that affect not only the team but also the quality of care to patients (Jason, 2000). Effective guidelines can be used when communicating. Such tools as SBAR are often used when conveying clinical information from one caregiver to another (Box 18-2). Most of these tools are used to facilitate a positive outcome and to create an environment in which the communicator can achieve the desired outcome. Unconscious use of any of the pitfalls will most likely result in thwarting the desired outcome. Box 18-3 lists effective guidelines for communication. When thinking about conflict, it is helpful to realize that conflict is fundamental to the human experience and is an integral part of all human interaction (Porter-O’Grady & Malloch, 2007)). Therefore the challenge is to recognize the breakdown in the communication process and to deal appropriately with it (Porter-O’Grady & Malloch, 2007). Conflicts are usually based on attempts to protect a person’s self-esteem or to alter perceived inequities in power, because most human beings believe that other people have greater power, and thus these human beings are unlikely to achieve their objectives (Sportsman, 2005). For example, when a nurse recognizes upset and reaction between two nursing assistants with whom he or she is working, the following steps can be helpful (Sportsman, 2005): • Identify the triggering event. • Discover the historical context for each person. • Assess how interdependent they are on each other. • Identify the issues, goals, and resources involved in the situation.
Building Teams Through Communication and Partnerships
Introduction
Groups and Teams
ATTRIBUTE
EFFECTIVE TEAM
INEFFECTIVE TEAM
Working environment
Informal, comfortable, relaxed
Indifferent, bored, tense, stiff
Discussion
Objectives
Well understood and accepted
Unclear, or many personal agendas
Listening
Respectful—encourages participation
Judgmental—much interruption and “grandstanding”
Ability to handle conflict
Decision making
Criticism
Leadership
Shared; shifts from time to time
Autocratic; remains clearly with committee chairperson
Assignments
Feelings
Freely expressed; open for discussion
Hidden; considered “explosive” and inappropriate for discussion
Self-regulation
Frequent and ongoing; focused on solutions
Infrequent, or occurs outside meetings
 Literature Perspective
Literature Perspective
Generational Differences
Communicating Effectively
Stress
Stress Response Model
PATTERN
INTERACTION
SOURCE
EXAMPLE
Attribution of blame
Sender blames receiver
Fault-finder dictator acts superior as camouflage for fear and low self-esteem
Mostly “you” messages; for example, “You really blew it!”
Placation
Sender placates receiver
Sender’s low self-worth: puts herself/himself down
“I was wrong. I’m sorry. It’s all my fault.”
Constrained cool-headedness
Sender is correct and very reasonable without feeling or emotion
Feelings of vulnerability covered by cool analytical thinking
“Studies have shown that in 75% of cases, the patient is correct. I decided to use research data in coming to a solution.”
Irrelevant
Sender is avoiding the issue, ignoring own feelings and feelings of the receiver
Fear, loneliness, and purposelessness
“Wait a minute. Let me tell you about …” (changes the subject)
Congruence
Sender’s words and actions are congruent; inner feelings match the message
Any tension is decreased, and self-worth is at a high level
“For now, I feel concerned about the anger and hostility exhibited by Dr. X. I’m wondering what approach would de-escalate him.”
Communication Barriers
Communication Pitfalls
Communication Guidelines
Key Concepts of Teams
Conflict Resolution
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Nurse Key
Fastest Nurse Insight Engine

Get Clinical Tree app for offline access
