Judith Laver Bierschbach
Assessment of the Ear and Hearing
Learning Outcomes
Safe and Effective Care Environment
Health Promotion and Maintenance
Psychosocial Integrity
Physiological Integrity
7 Perform a clinical ear and hearing assessment, including health history and psychosocial assessment.
9 Identify 10 common drugs that affect hearing.

http://evolve.elsevier.com/Iggy/
Animation: Ears: Weber Test
Answer Key for NCLEX Examination Challenges and Decision-Making Challenges
Audio Glossary
Key Points
Review Questions for the NCLEX® Examination
Video Clip: Ear Canal
Video Clip: External Ear
The ear and the brain together allow hearing. Hearing is one of the five senses important for communicating with the world. Functional hearing assists in the concepts of sensation and cognition. It is used to assess surroundings, allow independence, warn of danger, appreciate music, work, play, and interact with other people.
Ear and hearing problems are common among adults of all ages. Assessment of the ear and hearing is an important skill for nurses in any care environment. Therefore an understanding of the anatomy and physiology of the ear is essential. Many ear and hearing problems develop over long periods and may be affected by drugs or systemic health problems.
Anatomy and Physiology Review
Structure
The ear has three divisions: the external ear, the middle ear, and the inner ear. Each part is important to hearing.
External Ear
The external ear develops in the embryo at the same time as the kidneys and urinary tract. Thus any person with a defect of the external ear should be examined for possible problems of the kidney and urinary systems.
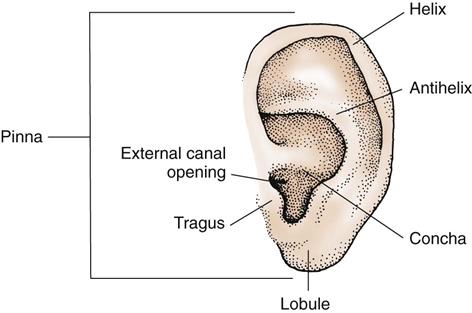
The pinna is the part of the external ear that is composed of cartilage covered by skin and attached to the head at about a 10-degree angle. It is embedded in the temporal bone on both sides of the head at the level of the eyes. The external ear also includes the mastoid process, which is the bony ridge located over the temporal bone behind the pinna. The external ear extends from the pinna through the external ear canal to the tympanic membrane (eardrum) (Fig. 50-1). The ear canal is slightly S-shaped and lined with cerumen (wax)-producing glands, sebaceous glands, and hair follicles. Cerumen helps protect and lubricate the ear canal. The hair follicles and cerumen protect the eardrum and the middle ear. The distance from the opening of the ear canal to the eardrum in an adult is 1 to  inches (2.5 to 3.75 cm).
inches (2.5 to 3.75 cm).
Middle Ear
The middle ear begins at the medial or inner side of the eardrum. The eardrum separates the external ear and the middle ear.
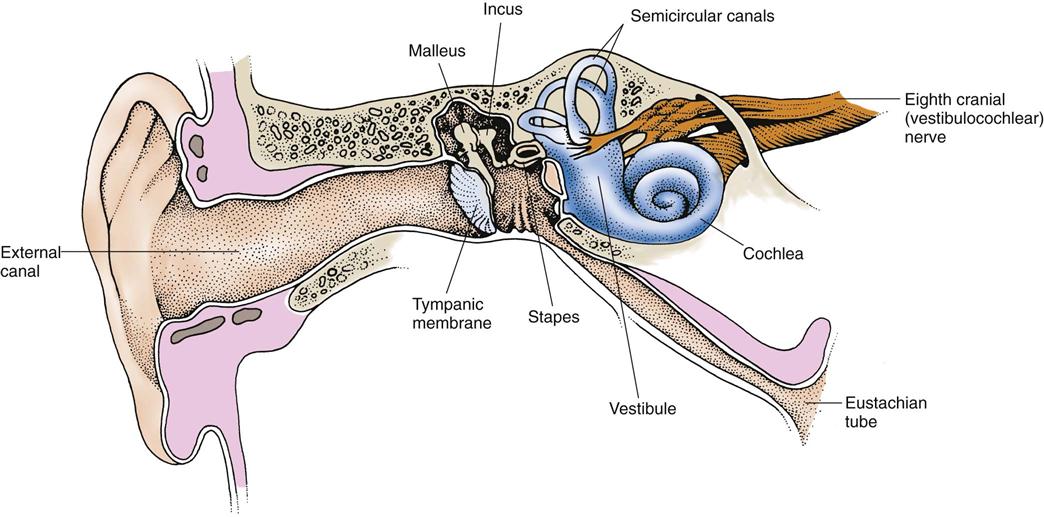
The middle ear consists of a compartment called the epitympanum. Located in the epitympanum are the top opening of the eustachian tube and three small bones known as the bony ossicles, which are the malleus (hammer), the incus (anvil), and the stapes (stirrup) (Fig. 50-2). The bony ossicles are joined loosely, thereby moving with vibrations created when sound waves hit the eardrum.
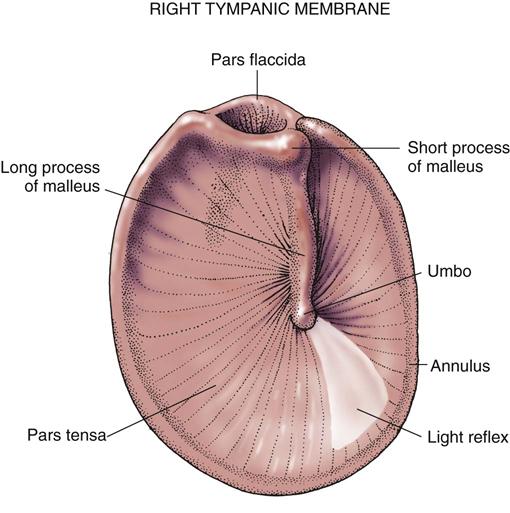
The eardrum, a thick sheet of tissue, is transparent, opaque, or pearly gray and moves when air is injected into the external canal. The landmarks on the eardrum include the annulus, the pars flaccida, and the pars tensa. These correspond to the parts of the malleus that can be seen through the transparent eardrum. The eardrum is attached to the first bony ossicle, the malleus, at the umbo (Fig. 50-3). The umbo is seen through the eardrum membrane as a white dot and is one end of the long process of the malleus. The pars flaccida is that portion of the eardrum above the short process of the malleus. The pars tensa is that portion surrounding the long process of the malleus.
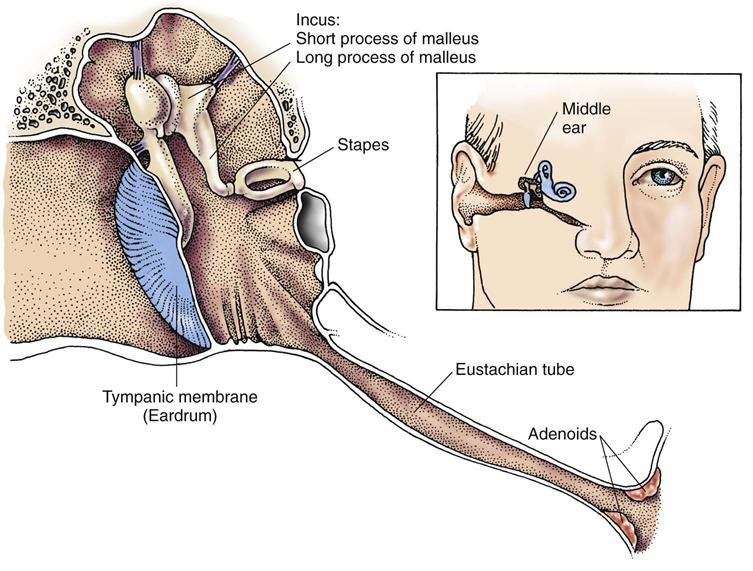
The middle ear is separated from the inner ear by the round window and the oval window. The eustachian tube begins at the floor of the middle ear and extends to the throat. The tube opening in the throat is surrounded by adenoid lymphatic tissue (Fig. 50-4). The eustachian tube allows the pressure on both sides of the eardrum to equalize. Secretions from the middle ear drain through the tube into the throat.
Inner Ear
The inner ear is on the other side of the oval window and contains the semicircular canals, the cochlea, the vestibule, and the distal end of the eighth cranial nerve (see Fig. 50-2). The semicircular canals are tubes made of cartilage and contain fluid and hair cells. These canals are connected to the sensory nerve fibers of the vestibular portion of the eighth cranial nerve. The fluid and hair cells within the canals help maintain the sense of balance.
The cochlea, the spiral organ of hearing, is divided into the scala tympani and the scala vestibuli. The scala media is filled with endolymph, and the scala tympani and scala vestibuli are filled with perilymph. These fluids protect the cochlea and the semicircular canals by allowing these structures to “float” in the fluids and be cushioned against abrupt head movements.
The organ of Corti is the receptor of hearing located on the basilar membrane of the cochlea. The cochlea contains hair cells that detect vibration from sound and stimulate the eighth cranial nerve.
The vestibule is a small, oval-shaped, bony chamber between the semicircular canals and the cochlea. It contains the utricle and the saccule, organs that are important for balance.
Function
Hearing is the main function of the ear and occurs when sound is delivered through the air to the external ear canal and the temporal bone covering the mastoid air cells. The sound waves strike the mastoid and the movable eardrum, creating vibrations. The eardrum is connected to the first bony ossicle, which allows the sound wave vibrations to be transferred from the eardrum to the malleus, the incus, and the stapes. From the stapes, the vibrations are transmitted to the cochlea. Receptors at the cochlea transduce (change) the vibrations into action potentials. The action potentials are conducted to the brain as nerve impulses by the cochlear portion of the eighth cranial (auditory) nerve. The nerve impulses are processed and interpreted as sound by the brain in the auditory cortex of the temporal lobe.
Ear and Hearing Changes Associated with Aging
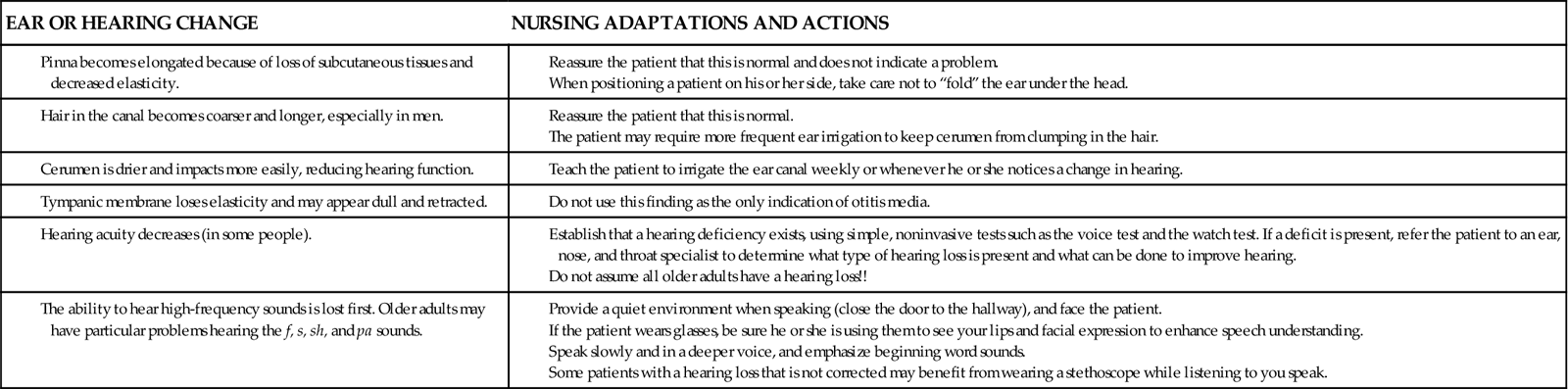
Ear and hearing changes related to aging are listed in Chart 50-1, along with implications for care of older patients who have these changes. Some of the ear changes, such as an increase in ear size, are harmless. Other changes to ear structures may pose threats to the hearing ability of older adults.
Chart 50-1
Nursing Focus on the Older Adult
Age-Related Changes in the Ear and Hearing
All older adults should be screened for hearing acuity. Many scales or tools are available to assess hearing loss. However, asking “Do you have a hearing problem now?” may be just as helpful as these scales. Family members may have noticed behaviors that suggest changes in a patient’s hearing.
Assessment Methods
Patient History
Obtain a thorough history from the patient before performing the physical examination. Hearing assessment begins while observing the patient listening to and answering questions. The patient’s posture and appropriateness of responses provide information about hearing acuity. For example, posture changes, such as tilting the head to one side or leaning forward when listening to another person speak, may indicate the presence of a hearing problem. Other indicators of hearing difficulty include frequently asking the speaker to repeat statements or frequently saying “What?” or “Huh?” Notice whether the patient responds to whispered questions and conversations and startles when an unexpected sound occurs in the environment. Also assess whether the patient’s responses match the question asked. For example, when you ask the patient “How old are you?” does the patient respond with an age or does he or she say “No, I don’t have a cold.”
During the interview, sit in adequate light and face the patient to allow him or her to see you speak. Use short, simple language the patient is comfortable with rather than long medical terms. Obtain data on demographics, personal and family history, socioeconomic status, current health problems, and the use of remedies for ear problems. Chart 50-2 lists important questions to ask about functional hearing.
The patient’s gender is important. Some hearing disorders, such as otosclerosis, are more common in women. Other disorders, such as Ménière’s disease, are more common in men. Age is also an important factor in hearing loss.
Personal history includes past or current manifestations of ear pain, ear discharge, vertigo (spinning sensation), tinnitus (ringing), decreased hearing, and difficulty understanding people when they talk or difficulty hearing environmental noise. Ask the patient about:
• Ear itch
• Any invasive instruments routinely used to clean the ear (e.g., Q-Tip, match, bobby pin, key)
• Type and pattern of ear hygiene
• Exposure to loud noise or music
• Air travel (especially in unpressurized aircraft)
• Swimming and whether ear protection is used
• History of hereditary factors that can cause progressive hearing loss
• History of smoking (reduces oxygenation of the cochlea)
• History of vitamin B12 and folate deficiency (associated with age-related hearing loss)
If the patient uses foreign objects to clean the ear canal (e.g., bobby-pins, Q-tips, toothpicks, keys), explain the danger in using these objects. They can scrape the skin of the canal, push cerumen up against the eardrum, and even puncture the eardrum. If the patient says that cerumen buildup is a problem, teach him or her to use an ear irrigation syringe and proper solutions to remove it. Chart 50-3 describes techniques to teach patients how to remove cerumen safely.
 Nursing Safety Priority
Nursing Safety Priority
Action Alert
Teach patients the safe way to clean their ears, stressing that nothing smaller than his or her own fingertip should be inserted into the canal.
Chart 50-3
Patient and Family Education: Preparing for Self-Management
Self–Ear Irrigation for Cerumen Removal
• The safest type of ear syringe to use is one that has a right-angle or “elbow” in the tip.
• Irrigating your ears in the shower is an easy method.
• Fill the syringe with the lukewarm tap water.
 – to
– to  -inch into your ear canal, aiming toward the roof of the canal.
-inch into your ear canal, aiming toward the roof of the canal.• Hold your head at a 30-degree angle to the side you are irrigating.
• Use one hand to hold the syringe and the other to push the plunger or squeeze the bulb.
• Apply gentle but firm continuous pressure, allowing the water to flow against the top of the canal.
• Do not use blasts or bursts of sudden pressure.
• The ear canal should fill, and water will begin to flow out, bringing ear wax and debris with it.
• If a dental water-pressure irrigator is used, put it on the lowest possible setting.
• Repeat the procedure on the other ear.
• If you feel that water is still in the canal, hold a hair dyer on a low setting near the ear.
• Irrigate your ears anytime from weekly to monthly, depending on how fast your ear wax collects.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


