Tami Kathleen Little
Assessment of the Cardiovascular System
Learning Outcomes
Safe and Effective Care Environment
Health Promotion and Maintenance
Psychosocial Integrity
Physiological Integrity
7 Review the anatomy and physiology of the CV system.
8 Describe the unique characteristics of heart disease in women.
9 Perform focused physical assessment for patients with CV problems.
10 Interpret laboratory test findings for patients with suspected or actual CV disease.
11 Differentiate invasive hemodynamic pressures and their significance.

http://evolve.elsevier.com/Iggy/
Animation: Auscultation of Heart Valves
Animation: Blood Flow: Circulatory System
Animation: Cardiac Cycle During Systole and Diastole
Animation: Heart Valves and Sounds
Animation: Pulse Variations
Answer Key for NCLEX Examination Challenges and Decision-Making Challenges
Audio Clip: Single S1
Audio Clip: S1 at Various Locations
Audio Clip: Single S2
Audio Clip: S2 at Various Locations
Audio Clip: S4
Audio Clip: S3
Audio Clip: Murmurs: High, Medium, and Low
Audio Clip: Murmurs: Blowing, Harsh or Rough, and Rumble
Audio Clip: Systolic Murmur
Audio Clip: Diastolic Murmur
Audio Clip: Pericardial Friction Rub
Audio Glossary
Concept Map Creator
Key Points
Review Questions for the NCLEX® Examination
Video Clip: Anterior Chest
Video Clip: Auscultation with Diaphragm and Bell
Video Clip: Auscultatory Landmarks
Video Clip: Carotid Artery
Video Clip: Pulses, Lower Extremities
As the name implies, the cardiovascular (CV) system is made up of the heart and blood vessels (both arteries and veins). It is responsible for supplying oxygen to body organs and other tissues (perfusion). The heart muscle, called the myocardium, must receive sufficient oxygen to pump blood to other parts of the body. The arteries must be patent so that the pumped blood can reach the rest of the body. Oxygen in the blood is needed for cells to live and function properly. When diseases or other problems of the CV systems occur, oxygenation and perfusion decrease, often resulting in life-threatening events or a risk for these events.
The CV system works with the respiratory and hematologic systems to meet the human need for oxygenation and tissue perfusion (see Fig. 1 of the Concept Overview). Any problem in these systems requires the CV system to work harder to meet oxygenation and tissue perfusion needs.
In almost every year since 1900, cardiovascular disease (CVD) has been the number-one cause of death in the United States. Nearly 2300 Americans die of CVD each day, an average of one death every 38 seconds (American Heart Association [AHA], 2010b). The disease kills more people than the next four causes of death combined, including cancer, chronic lower respiratory diseases, accidents, and diabetes. Of particular concern is that CVD is the leading cause of death for women. In addition, the American Heart Association (AHA) estimates that more than one in three adults is living with some form of the disease. About 20% of people who experience a myocardial infarction will die within 1 year from the initial cardiac event (AHA, 2010b).
Anatomy and Physiology Review
Heart
Structure
The human heart is a fist-sized, muscular organ located in the mediastinum between the lungs (Fig. 35-1). Each beat of the heart pumps about 60 mL of blood, or 5 L/min. During strenuous physical activity, it can double the amount of blood pumped to meet the body’s increased oxygenation needs. The heart is protected by a covering called the pericardium. A muscular wall (septum) separates the heart into two halves: right and left. Each half has an atrium and a ventricle (Fig. 35-2).


The right atrium (RA) receives deoxygenated venous blood, which is returned from the body through the superior and inferior venae cavae. It also receives blood from the heart muscle through the coronary sinus. Most of this venous return flows passively from the RA, through the opened tricuspid valve, and to the right ventricle during ventricular diastole, or filling. The remaining venous return is actively propelled by the RA into the right ventricle during atrial systole, or contraction.
The right ventricle (RV) is a muscular pump located behind the sternum. It generates enough pressure to close the tricuspid valve, open the pulmonic valve, and propel blood into the pulmonary artery and the lungs.
After blood is reoxygenated in the lungs, it flows freely from the four pulmonary veins into the left atrium. Blood then flows through an opened mitral valve into the left ventricle during ventricular diastole. When the left ventricle is almost full, the left atrium (LA) contracts, pumping the remaining blood volume into the left ventricle. With systolic contraction, the left ventricle (LV) generates enough pressure to close the mitral valve and open the aortic valve. Blood is propelled into the aorta and into the systemic arterial circulation. Blood flow through the heart is shown in Fig. 35-2.
Blood moves from the aorta throughout the systemic circulation to the various tissues of the body. The pressure of blood in the aorta of a young adult averages about 100 to 120 mm Hg, whereas the pressure of blood in the RA averages about 0 to 5 mm Hg. These differences in pressure produce a pressure gradient, with blood flowing from an area of higher pressure to an area of lower pressure. The heart and vascular structures are responsible for maintaining these pressures.
The four cardiac valves are responsible for maintaining the forward flow of blood through the chambers of the heart (see Fig. 35-2). These valves open and close when pressure and volume change within the heart’s chambers. The cardiac valves are classified into two types: atrioventricular (AV) valves and semilunar valves.
The AV valves separate the atria from the ventricles. The tricuspid valve separates the RA from the RV. The mitral (bicuspid) valve separates the LA from the LV. During ventricular diastole, these valves act as funnels and help move the flow of blood from the atria to the ventricles. During systole, the valves close to prevent the backflow (regurgitation) of blood into the atria.
The semilunar valves are the pulmonic valve and the aortic valve that prevent blood from flowing back into the ventricles during diastole. The pulmonic valve separates the right ventricle from the pulmonary artery. The aortic valve separates the left ventricle from the aorta.
The heart muscle receives blood to meet its metabolic needs through the coronary arterial system (Fig. 35-3). The coronary arteries originate from an area on the aorta just beyond the aortic valve. All of the coronary arteries feeding the left heart originate from the left main coronary artery (LMCA). The right coronary artery (RCA) branches from the aorta to perfuse the right heart and inferior wall of the left heart.
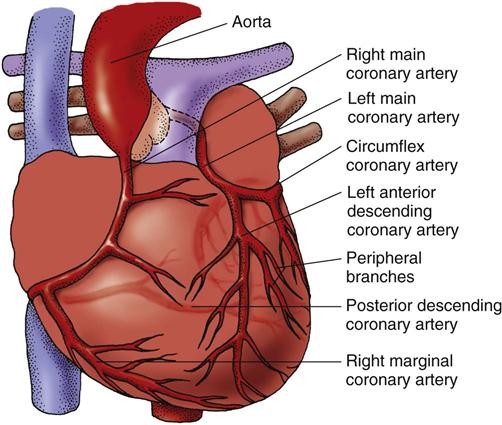
Coronary artery blood flow to the myocardium occurs primarily during diastole, when coronary vascular resistance is minimized. To maintain adequate blood flow through the coronary arteries, mean arterial pressure (MAP) must be at least 60 mm Hg. A MAP of between 60 and 70 mm Hg is necessary to maintain perfusion of major body organs, such as the kidneys and brain.
The left main artery divides into two branches: the left anterior descending (LAD) branch and the left circumflex (LCX) branch. The LAD branch descends toward the anterior wall and the apex of the left ventricle. It supplies blood to portions of the left ventricle, ventricular septum, chordae tendineae, papillary muscle, and, to a lesser extent, the right ventricle.
The LCX branch descends toward the lateral wall of the left ventricle and apex. It supplies blood to the left atrium, the lateral and posterior surfaces of the left ventricle, and sometimes portions of the interventricular septum. In about half of people, the LCX branch supplies the sinoatrial (SA) node. In a very small number of people, it supplies the AV node. Peripheral branches arise from the LAD and LCX branches and form an abundant network of vessels throughout the entire myocardium.
The right coronary artery (RCA) originates from the right sinus of Valsalva, encircles the heart, and descends toward the apex of the right ventricle. The RCA supplies the RA, RV, and inferior portion of the LV. In about half of people, the RCA supplies the SA node, and in almost everyone, it supplies the AV node.
Function
The electrophysiologic properties of heart muscle are responsible for regulating heart rate (HR) and rhythm. Cardiac muscle cells possess the characteristics of automaticity, excitability, conductivity, contractility, and refractoriness. Chapter 36 describes these properties and cardiac conduction in detail.
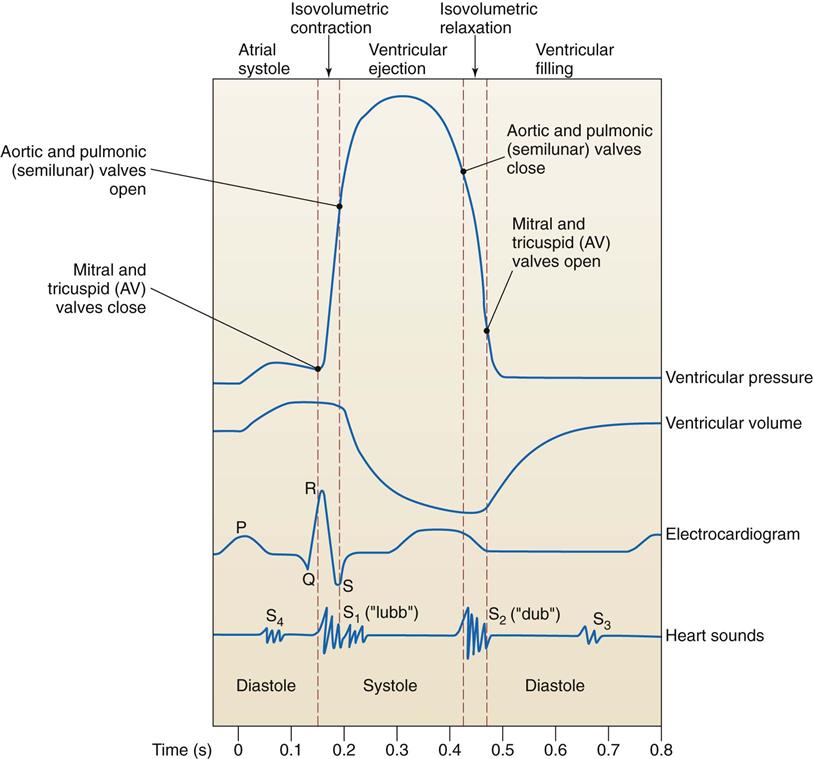
Sequence of Events During the Cardiac Cycle.
The phases of the cardiac cycle are generally described in relation to changes in pressure and volume in the left ventricle during filling (diastole) and ventricular contraction (systole) (Fig. 35-4). Diastole, normally about two thirds of the cardiac cycle, consists of relaxation and filling of the atria and ventricles. Systole consists of the contraction and emptying of the atria and ventricles.
Myocardial contraction results from the release of large numbers of calcium ions from the sarcoplasmic reticulum and from the blood. These ions diffuse into the myofibril sarcomere (the basic contractile unit of the myocardial cell). Calcium ions promote the interaction of actin and myosin protein filaments, causing these filaments to link and overlap. Cross-bridges, or linkages, are formed as the protein filaments slide over or overlap each other. These cross-bridges act as force-generating sites. The sliding of these protein filaments shortens the sarcomeres, producing myocardial contraction.
Cardiac muscle relaxes when calcium ions are pumped back into the sarcoplasmic reticulum, causing a decrease in the number of calcium ions around the myofibrils. This reduced number of ions causes the protein filaments to disengage, the sarcomere to lengthen, and the muscle to relax.
Mechanical Properties of the Heart.
The electrical and mechanical properties of cardiac muscle determine the function of the cardiovascular system. The healthy heart can adapt to various pathophysiologic conditions (e.g., stress, infections, hemorrhage) to maintain adequate blood flow to the various body tissues. Blood flow from the heart into the systemic arterial circulation is measured clinically as cardiac output (CO), the amount of blood pumped from the left ventricle each minute. CO depends on the relationship between heart rate (HR) and stroke volume (SV); it is the product of these two variables:

In adults, the CO ranges from 4 to 7 L/min. Because CO requirements vary according to body size, the cardiac index is calculated to adjust for differences in body size. The cardiac index can be determined by dividing the CO by the body surface area. The normal range is 2.7 to 3.2 L/min/m2 of body surface area.
Heart rate (HR) refers to the number of times the ventricles contract each minute. The normal resting HR for an adult is between 60 and 100 beats/min. Increases in rate increase myocardial oxygen demand. The HR is extrinsically controlled by the autonomic nervous system (ANS), which adjusts rapidly when necessary to regulate cardiac output. The parasympathetic (vagus nerve) system slows the HR, whereas sympathetic stimulation increases the heart rate. An increase in circulating catecholamines (e.g., epinephrine and norepinephrine) usually causes an increase in HR and contractility. Many cardiovascular drugs, particularly beta blockers, block this sympathetic (fight or flight) pattern by decreasing the HR.
Stroke volume (SV) is the amount of blood ejected by the left ventricle during each contraction. Several variables influence SV and, ultimately, CO. These variables include HR, preload, afterload, and contractility.
Preload refers to the degree of myocardial fiber stretch at the end of diastole and just before contraction. The stretch imposed on the muscle fibers results from the volume contained within the ventricle at the end of diastole. Preload is determined by the amount of blood returning to the heart from both the venous system (right heart) and the pulmonary system (left heart) (left ventricular end-diastolic [LVED] volume).
An increase in ventricular volume increases muscle-fiber length and tension, thereby enhancing contraction and improving stroke volume. This statement is derived from Starling’s law of the heart: The more the heart is filled during diastole (within limits), the more forcefully it contracts. Excessive filling of the ventricles results in excessive LVED volume and pressure, however, and may result in decreased cardiac output.
Another factor affecting stroke volume, afterload, is the pressure or resistance that the ventricles must overcome to eject blood through the semilunar valves and into the peripheral blood vessels. The amount of resistance is directly related to arterial blood pressure and the diameter of the blood vessels.
Impedance, the peripheral component of afterload, is the pressure that the heart must overcome to open the aortic valve. The amount of impedance depends on aortic compliance and total systemic vascular resistance, a combination of blood viscosity (thickness) and arteriolar constriction. A decrease in stroke volume can result from an increase in afterload without the benefit of compensatory mechanisms, thus leading to a decrease in cardiac output.
Myocardial contractility affects stroke volume and CO and is the force of cardiac contraction independent of preload. Contractility is increased by factors such as sympathetic stimulation, calcium release, and positive inotropic drugs. It is decreased by factors such as hypoxia and acidemia.
Vascular System
The vascular system serves several purposes:
• Provides a route for blood to travel from the heart to nourish the various tissues of the body
• Carries cellular wastes to the excretory organs
• Allows lymphatic flow to drain tissue fluid back into the circulation
The vascular system is divided into the arterial system and the venous system. In the arterial system, blood moves from the larger arteries to a network of smaller blood vessels, called arterioles, which meet the capillary bed. In the venous system, blood travels from the capillaries to the venules and to the larger system of veins, eventually returning in the vena cava to the heart for recirculation.
Arterial System
The primary function of the arterial system is to deliver oxygen and nutrients to various tissues in the body. Nutrients are carried through arteries to arterioles, then branch into smaller terminal arterioles and finally join with capillaries and venules to form a capillary network. Within this network, nutrients are exchanged across capillary membranes by three primary processes: osmosis, filtration, and diffusion. (See Chapter 13 for detailed discussions of these processes.)
The arterial system delivers blood to various tissues for oxygen and nourishment. At the tissue level, nutrients, chemicals, and body defense substances are distributed and exchanged for cellular waste products, depending on the needs of the particular tissue. The arteries transport the cellular wastes to the excretory organs (e.g., kidneys and lungs) to be reprocessed or removed. These vessels also contribute to temperature regulation in the tissues. Blood can be either directed toward the skin to promote heat loss or diverted away from the skin to conserve heat.
Blood pressure (BP) is the force of blood exerted against the vessel walls. Pressure in the larger arterial blood vessels is greater (about 80 to 100 mm Hg) and decreases as blood flow reaches the capillaries (about 25 mm Hg). By the time blood enters the right atrium, the BP is about 0 to 5 mm Hg. Volume, ventricular contraction, and vascular tone are necessary to maintain blood pressure.
BP is determined primarily by the quantity of blood flow or cardiac output (CO), as well as by the resistance in the arterioles:

Any factor that increases CO or total peripheral vascular resistance increases the BP. In general, BP is maintained at a relatively constant level. Therefore an increase or decrease in total peripheral vascular resistance is associated with a decrease or an increase in CO, respectively. Three mechanisms mediate and regulate BP:
Systolic BP is the amount of pressure/force generated by the left ventricle to distribute blood into the aorta with each contraction of the heart. It is a measure of how effectively the heart pumps and is an indicator of vascular tone. Diastolic BP is the amount of pressure/force against the arterial walls during the relaxation phase of the heart.
BP is regulated by balancing the sympathetic and parasympathetic nervous systems of the autonomic nervous system. Changes in autonomic activity are responses to messages sent by the sensory receptors in the various tissues of the body. These receptors, including the baroreceptors, chemoreceptors, and stretch receptors, respond differently to the biochemical and physiologic changes of the body.
Baroreceptors in the arch of the aorta and at the origin of the internal carotid arteries are stimulated when the arterial walls are stretched by an increased BP. Impulses from these baroreceptors inhibit the vasomotor center, which is located in the pons and the medulla. Inhibition of this center results in a drop in BP.
Several 1- to 2-mm collections of tissue have been identified in the carotid arteries and along the aortic arch known as peripheral chemoreceptors. These receptors are sensitive primarily to hypoxemia (a decrease in the partial pressure of arterial oxygen [PaO2]). When stimulated, these chemoreceptors send impulses along the vagus nerves to activate a vasoconstrictor response and raise BP.
The central chemoreceptors in the respiratory center of the brain are also stimulated by hypercapnia (an increase in partial pressure of arterial carbon dioxide [PaCO2]) and acidosis. The direct effect of carbon dioxide on the central nervous system (CNS), however, is 10 times stronger than the effect of hypoxia on the peripheral chemoreceptors.
Stretch receptors in the vena cava and the right atrium are sensitive to pressure or volume changes. When a patient is hypovolemic, stretch receptors in the blood vessels sense a reduced volume or pressure and send fewer impulses to the CNS. This reaction stimulates the sympathetic nervous system to increase the heart rate (HR) and constrict the peripheral blood vessels.
The kidneys also help regulate cardiovascular activity. When renal blood flow or pressure decreases, the kidneys retain sodium and water. BP tends to rise because of fluid retention and activation of the renin-angiotensin-aldosterone mechanism (see Fig. 13-6 in Chapter 13). This mechanism results in vasoconstriction and sodium retention (and thus fluid retention). Vascular volume is also regulated by the release of antidiuretic hormone (vasopressin) from the posterior pituitary gland (see Chapter 13).
Other factors can also influence the activity of the cardiovascular system. Emotional behaviors (e.g., excitement, pain, anger) stimulate the sympathetic nervous system to increase blood pressure (BP) and heart rate (HR). Increased physical activity such as exercise also increases BP and HR during the activity. Body temperature can affect the metabolic needs of the tissues, thereby influencing the delivery of blood. In hypothermia, tissues require fewer nutrients and blood pressure falls. In hyperthermia, the metabolic requirement of the tissues is greater and BP and pulse rate rise.
Venous System
The primary function of the venous system is to complete the circulation of blood by returning blood from the capillaries to the right side of the heart. It is composed of a series of veins that are located next to the arterial system. A second superficial venous circulation runs parallel to the subcutaneous tissue of the extremity. These two venous systems are connected by communicating veins that provide a means for blood to travel from the superficial veins to the deep veins. Blood flow is directed toward the deep venous circulation.
Veins have the ability to accommodate large shifts in volume with minimal changes in venous pressure. This flexibility allows the venous system to accommodate the administration of IV fluids and blood transfusions, as well as to maintain pressure during blood loss and dehydration. Veins in the superficial and deep venous systems (except the smallest and the largest veins) have valves that direct blood flow back to the heart and prevent backflow. Skeletal muscles in the extremities provide a force that helps push the venous blood forward. The superior vena cava and inferior vena cava are valveless and large enough to allow blood flow to return easily to the heart.
Gravity exerts an increase in hydrostatic pressure in the capillaries when the patient is in an upright position, delaying venous return. Hydrostatic pressure is decreased in dependent areas such as the legs when the patient is lying down, and thus there is less hindrance of venous return to the heart.
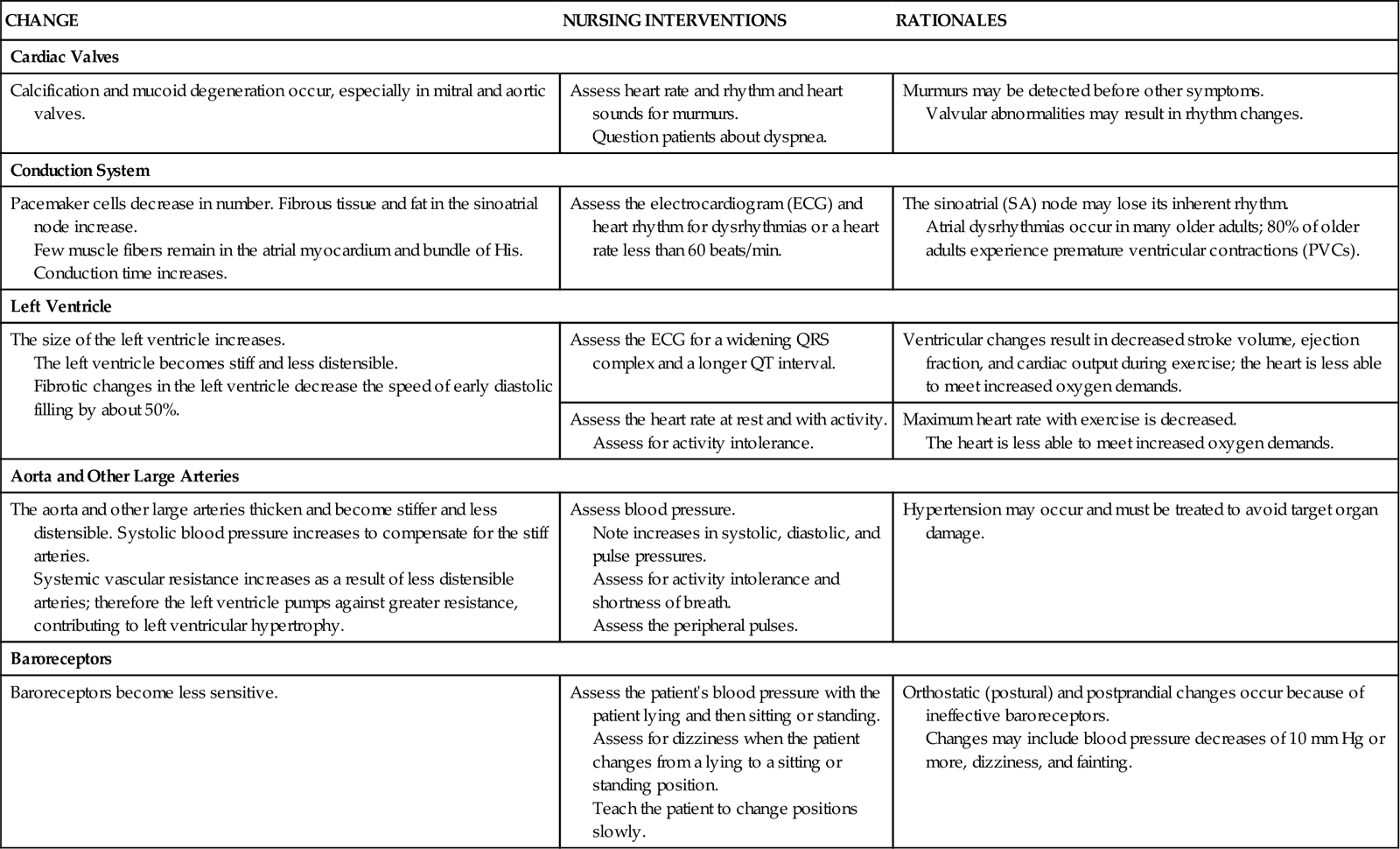
Cardiovascular Changes Associated with Aging
A number of physiologic changes in the cardiovascular system occur with advancing age (Chart 35-1). Many of these changes result in a loss of cardiac reserve. Thus these changes are usually not evident when the older adult is resting. They become apparent only when the person is physically or emotionally stressed and the heart cannot meet the increased metabolic demands of the body.
Assessment Methods
Patient History
The focus of the patient history is on obtaining information about risk factors and symptoms of cardiovascular disease (Chart 35-2). Assess nonmodifiable (uncontrollable) risk factors including the patient’s age, gender, ethnic origin, and family history of cardiovascular disease. Ask about any chronic disease or illness that the patient may have. The incidence of conditions such as coronary artery disease (CAD) and valvular disease increases with age. The incidence of CAD also varies with the patient’s gender. Men have a higher risk for CAD than women of all ages except in the oldest age-group of 80 years and older (AHA, 2010b).
Heart disease is the leading cause of diabetes-related death for both men and women. Adults with diabetes have heart disease death rates 2 to 4 times higher than those without diabetes. The risk for stroke is also 2 to 4 times higher among people with diabetes. The number of premature deaths (younger than 65 years) from heart disease is greatest among American Indians and Alaska Natives and lowest among Asians (AHA, 2010b).
Modifiable (controllable) risk factors should also be assessed. Modifiable risk factors are personal lifestyle habits, including cigarette use, physical inactivity, obesity, and psychological variables. Ask the patient about each of these common risk factors.
Cigarette smoking is a major risk factor for CVD, specifically coronary artery disease (CAD) and peripheral vascular disease (PVD). Three compounds in cigarette smoke have been implicated in the development of CAD: tar, nicotine, and carbon monoxide. The smoking history should include the number of cigarettes smoked daily, the duration of the smoking habit, and the age of the patient when smoking started. Record the smoking history in pack-years, which is the number of packs per day multiplied by the number of years the patient has smoked.
Ask about the patient’s desire to quit, past attempts to quit, and the methods used. Determine nicotine dependence by asking questions such as:
• How soon after you wake up in the morning do you smoke?
• Do you wake up in the middle of your sleep time to smoke?
• Do you find it difficult not to smoke in places where smoking is prohibited?
Three to four years after a patient has stopped smoking, his or her CVD risk appears to be similar to that of a person who has never smoked. Be sure to ask those who do not currently smoke whether they have ever smoked and when they quit. Passive smoke significantly reduces blood flow in healthy young adults’ coronary arteries, and the risk for dying increases among those who are exposed to secondhand smoke (AHA, 2010a).
A sedentary lifestyle is also a major risk factor for heart disease. Regular physical activity promotes cardiovascular fitness and produces beneficial changes in blood pressure and levels of blood lipids and clotting factors. Unfortunately, few people in the United States follow the recommended exercise guidelines: 30 minutes daily of light to moderate exercise, which is equivalent to a 30-minute brisk walk. According to the American Heart Association (AHA) (2010a), fewer than two thirds of people in the United States engage in this much exercise five times a week and fewer engage in more vigorous physical activity to promote cardiopulmonary fitness. Encourage increased physical exercise as part of a lifestyle change to reduce the risk for CAD. Ask patients about the type of exercise they perform, how long a period they have participated in the exercise, and the frequency and intensity of the exercise.
About two thirds of American adults are overweight when defined as a body mass index (BMI) of 25 to 30. Obesity, defined as a BMI greater than 30, is particularly a problem for African-American women, Mexican Americans, and native Hawaiians, but the exact cause of this cultural difference is unknown (AHA, 2010a). Obesity is also associated with hypertension, hyperlipidemia, and diabetes; all are known contributors to CVD.
The American Heart Association provides guidelines to combat obesity and improve cardiac health, including ingesting more nutrient-rich foods that have vitamins, minerals, fiber, and other nutrients but are low in calories. To get the necessary nutrients, teach patients to choose foods like vegetables, fruits, whole-grain products, and fat-free dairy products most often. Also teach patients to not eat more calories than they can burn every day (AHA, 2010a).
A variety of psychological factors make people more vulnerable to the development of heart disease. Those who are highly competitive, overly concerned about meeting deadlines, and often hostile or angry are at higher risk for heart disease. Psychological stress, anger, depression, and hostility are all closely associated with risk for developing heart disease.
You might ask the patient, “How do you respond when you have to wait for an appointment?” Chronic anger and hostility appear to be closely associated with CVD. The constant arousal of the sympathetic nervous system as a result of anger may influence blood pressure, serum fatty acids and lipids, and clotting mechanisms. Observe the patient, and assess his or her response to stressful situations.
Review the patient’s medical history, noting any major illnesses such as diabetes mellitus, renal disease, anemia, high BP, stroke, bleeding disorders, connective tissue diseases, chronic pulmonary diseases, heart disease, and thrombophlebitis. These conditions can influence the patient’s cardiovascular status.
Ask about previous treatment for CVD, identify previous diagnostic procedures (e.g., electrocardiography [ECG], cardiac catheterization), and request information about any medical or invasive treatment of CVD. Ask specifically about recurrent tonsillitis, streptococcal infections, and rheumatic fever because these conditions may lead to valvular abnormalities of the heart. In addition, inquire about any known congenital heart defects. Many patients with congenital heart problems live into adulthood because of improved treatment and surgeries.
Ask patients about their drug history, beginning with any current or recent use of prescription or over-the-counter (OTC) medications or herbal/natural products. Inquire about known sensitivities to any drug and the nature of the reaction (e.g., nausea, rash). Patients should be asked whether they have recently used cocaine or any IV “street” drugs, because these substances are often associated with heart disease.
Ask women whether they are taking oral contraceptives or an estrogen replacement. The incidence of myocardial infarction (MI) and stroke in women older than 35 years who take oral contraceptives is increased if they smoke, have diabetes, or have hypertension.
The social history includes information about the patient’s living situation, including having a domestic partner, other household members, environment, and occupation. Identification of support systems is especially important in exploring the possibility that the patient might have difficulty paying for medications or treatment. People who report an annual household income less than $30,000 have a greater risk for CVD than people who have an income over $50,000 (Metcalf et al., 2008; Wright et al., 2009).
Ask about occupation, including the type of work performed and the requirements of the specific job. For instance, does the job involve physical exertion such as lifting heavy objects? Is the job emotionally stressful? What does a day’s work entail? Does the patient’s job require him or her to be outside in extreme weather conditions?
Nutrition History
A nutrition history includes the patient’s recall of food and fluid intake during a 24-hour period, self-imposed or medically prescribed dietary restrictions or supplementations, and the amount and type of alcohol consumption. If needed, the dietitian reviews the type of foods selected by the patient for the amount of sodium, sugar, cholesterol, fiber, and fat. Cultural beliefs and economic status can influence the choice of food items and therefore are seriously considered. Family members or significant others who are responsible for shopping and cooking should be included in this screening.
 NCLEX Examination Challenge
NCLEX Examination Challenge
Health Promotion and Maintenance
The nurse is providing education to help reduce cardiovascular risks for adults at a community health fair. Which statement made by a participant indicates understanding of the health education?
A “I can’t do anything about my disease risk because it is in my genes.”
B “I will take my blood pressure medication only when I have symptoms.”
C “I will start walking on the treadmill each day when I watch my favorite TV show.”
D “I don’t need to stop smoking because damage to my blood vessels is irreversible.”
Family History and Genetic Risk
Review the family history, and obtain information about the age, health status, and cause of death of immediate family members. A positive family history for CAD in a first-degree relative (parent, sibling, or child) is a major risk factor. It is more important than other factors such as hypertension, obesity, diabetes, or sudden cardiac death (AHA, 2010b).
Current Health Problems
Ask the patient to describe his or her health concerns. Expand on the description of these concerns by obtaining information about their onset, duration, sequence, frequency, location, quality, intensity, associated symptoms, and precipitating, aggravating, and relieving factors. Major symptoms usually identified by patients with CVD include chest pain or discomfort, dyspnea, fatigue, palpitations, weight gain, syncope, and extremity pain.
Pain or discomfort, considered a traditional symptom of heart disease, can result from ischemic heart disease, pericarditis, and aortic dissection. Chest pain can also be due to noncardiac conditions such as pleurisy, pulmonary embolus, hiatal hernia, gastroesophageal reflux disease, neuromuscular abnormalities, and anxiety.
 Nursing Safety Priority
Nursing Safety Priority
Action Alert
Thoroughly evaluate the nature and characteristics of the chest pain. Because pain resulting from myocardial ischemia is life threatening and can lead to serious complications, its cause should be considered ischemic (reduced or obstructed blood flow to the myocardium) until proven otherwise. When assessing for symptoms, ask the patient if he or she has “discomfort,” “heaviness,” “pressure,” and “indigestion.”
Ask the patient to identify when the symptoms were first noticed (onset):
If he or she has repeated painful episodes, assess how often the symptoms occur (frequency). If pain is present, ask whether it is different from any other episodes of pain. Ask the patient to describe what activities he or she was doing when it first occurred, such as sleeping, arguing, or running (precipitating factors). If possible, the patient should point to the area where the chest pain occurred (location) and describe if and how the pain radiated (spread).
In addition, ask how the pain feels and whether it is sharp, dull, or crushing (quality of pain). To understand the severity of the pain, ask the patient to grade it from 1 to 10, with 10 indicating severe pain (intensity). He or she may also report other signs and symptoms that occur at the same time (associated symptoms), such as dyspnea, diaphoresis (excessive sweating), nausea, and vomiting. Other factors that need to be addressed are those that may have made the chest pain worse (aggravating factors) or less intense (relieving factors). Chest pain can arise from a variety of sources (Table 35-1). By obtaining the appropriate information, you can help identify the source of the chest discomfort.
TABLE 35-1
Assessment of Chest Discomfort: How Various Types of Chest Pain Differ
| ONSET | QUALITY AND SEVERITY | LOCATION AND RADIATION | DURATION AND RELIEVING Factors |
| Angina | |||
| Sudden, usually in response to exertion, emotion, or extremes in temperature | Squeezing, viselike pain | Substernal; may spread across the chest and the back and/or down the arms | Usually the left side of chest without radiation Usually lasts less than 15 min; relieved with rest, nitrate administration, or oxygen therapy |
| Myocardial Infarction | |||
| Sudden, without precipitating factors, often in early morning | Intense stabbing, viselike pain or pressure, severe | Substernal; may spread throughout the anterior chest and to the arms, jaw, back, or neck | Continuous or no chest discomfort; relieved with morphine, cardiac drugs, and oxygen therapy |
| Pericarditis | |||
| Sudden | Sharp, stabbing, moderate to severe | Substernal; usually spreads to the left side or the back | Intermittent; relieved with sitting upright, analgesia, or administration of anti-inflammatory agents |
| Pleuropulmonary | |||
| Variable | Moderate ache, worse on inspiration | Lung fields | Continuous until the underlying condition is treated or the patient has rested |
| Esophageal-Gastric | |||
| Variable | Squeezing, heartburn, variable severity | Substernal; may spread to the shoulders or the abdomen | Variable; may be relieved with antacid administration, food intake, or taking a sitting position |
| Anxiety | |||
| Variable, may be in response to stress or fatigue | Dull ache to sharp stabbing; may be associated with numbness in fingers | Not well located and usually does not radiate to other parts of the body as pain | Usually lasts a few minutes |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


