Maternal role attainment becoming a mother
Molly Meighan
“The process of becoming a mother requires extensive psychological, social, and physical work. A woman experiences heightened vulnerability and faces tremendous challenges as she makes this transition. Nurses have an extraordinary opportunity to help women learn, gain confidence, and experience growth as they assume the mother identity”
(Mercer, 2006, p. 649).
Ramona T. Mercer
1929 to present
Photo credit: Marie Cox, M&M Studios, San Francisco, CA.
Previous authors: Mary M. (Molly) Meighan, Alberta M. Bee, Denise Legge, and Stephanie Oetting.
Credentials and background of the theorist
Ramona T. Mercer began her nursing career in 1950, when she received her diploma from St. Margaret’s School of Nursing in Montgomery, Alabama. She graduated with the L.L. Hill Award for Highest Scholastic Standing. She returned to school in 1960 after working as a staff nurse, head nurse, and instructor in the areas of pediatrics, obstetrics, and contagious diseases. She completed a bachelor’s degree in nursing in 1962, graduating with distinction from the University of New Mexico, Albuquerque. She went on to earn a master’s degree in maternal-child nursing from Emory University in 1964 and completed a Ph.D. in maternity nursing at the University of Pittsburgh in 1973.
After receiving her Ph.D., Mercer moved to California and accepted the position of Assistant Professor in the Department of Family Health Care Nursing at the University of California, San Francisco. She was promoted to associate professor in 1977 and to full professor in 1983. She remained in that role until her retirement in 1987. Currently, Dr. Mercer is Professor Emeritus in Family Health Nursing at the University of California, San Francisco (Mercer, curriculum vitae, 2002).
Mercer received awards throughout her career. In 1963, while working and pursuing studies in nursing, she received the Department of Health, Education, and Welfare Public Health Service Nurse Trainee Award at Emory University and was inducted into Sigma Theta Tau. She received this award again during her years at the University of Pittsburgh. She also received the Bixler Scholarship for Nursing Education and Research, Southern Regional Board, for doctoral study. In 1982, she received the Maternal Child Health Nurse of the Year Award from the National Foundation of the March of Dimes and American Nurses Association, Division of Maternal Child Health Practice. She was presented with the Fourth Annual Helen Nahm Lecturer Award at the University of California, San Francisco School of Nursing, in 1984. Mercer’s research awards include the American Society for Psychoprophylaxis in Obstetrics (ASPO)/Lamaze National Research Award in 1987; the Distinguished Research Lectureship Award, Western Institute of Nursing, Western Society for Research in Nursing in 1988; and the American Nurses Foundation’s Distinguished Contribution to Nursing Science Award in 1990 (Mercer, curriculum vitae, 2002). Mercer has authored numerous articles, editorials, and commentaries. In addition, she has published six books and six book chapters.
In early research efforts, Mercer focused on the behaviors and needs of breastfeeding mothers, mothers with postpartum illness, mothers bearing infants with defects, and teenage mothers. Her first book, Nursing Care for Parents at Risk (1977), received an American Journal of Nursing Book of the Year Award in 1978. Her study of teenage mothers over the first year of motherhood resulted in the 1979 book, Perspectives on Adolescent Health Care, which also received an American Journal of Nursing Book of the Year Award in 1980. Preceding research led Mercer to study family relationships, antepartal stress as related to familial relationships and the maternal role, and mothers of various ages. In 1986, Mercer’s research on three age groups of mothers was drawn together in her third book, First-Time Motherhood: Experiences from Teens to Forties (1986a). Mercer’s fifth book, Parents at Risk, published in 1990, also received an American Journal of Nursing Book of the Year Award. Parents at Risk (1990) focused on strategies for facilitating early parent-infant interactions and promoting parental competence in relation to specific risk situations. Mercer’s sixth book, Becoming a Mother: Research on Maternal Identity from Rubin to the Present, was published by Springer Publishing Company of New York in 1995. This book contains a more complete description of Mercer’s Theory of Maternal Role Attainment and her framework for studying variables that impact the maternal role.
Since her first publication in 1968, Mercer has written numerous articles for both nursing and non-nursing journals. She published several online courses for Nurseweek during the 1990s and through early 2000, including “Adolescent Sexuality and Child-bearing,” “Transitions to Parenthood,” and “Helping Parents When the Unexpected Occurs.”
Mercer maintained membership in several professional organizations, including the American Nurses Association and the American Academy of Nursing, and was an active member on many national committees. From 1983 to 1990, she was Associate Editor of Health Care for Women International. Mercer served on the review panel for Nursing Research and Western Journal of Nursing Research and on the editorial board of the Journal of Adolescent Health Care, and she was on the executive advisory board of Nurseweek. She also served as a reviewer for numerous grant proposals. Additionally, she was actively involved with regional, national, and international scientific and professional meetings and workshops (Mercer, curriculum vitae, 2002). She was honored as a Living Legend by the American Academy of Nursing during the Annual Meeting and Conference in Carlsbad, California, in November 2003. Mercer was honored by the University of New Mexico in 2004, receiving the first College of Nursing Distinguished Alumni Award. In 2005, she was recognized as among the most outstanding alumni and faculty, and her name appears on the Wall of Fame at the University of California, San Francisco.
Theoretical sources
Mercer’s Theory of Maternal Role Attainment was based on her extensive research on the topic beginning in the late 1960s. Mercer’s professor and mentor, Reva Rubin at the University of Pittsburgh, was a major stimulus for both research and theory development. Rubin (1977, 1984) was well known for her work in defining and describing maternal role attainment as a process of binding-in, or being attached to, the child and achieving a maternal role identity or seeing oneself in the role and having a sense of comfort about it. Mercer’s framework and study variables reflect many of Rubin’s concepts.
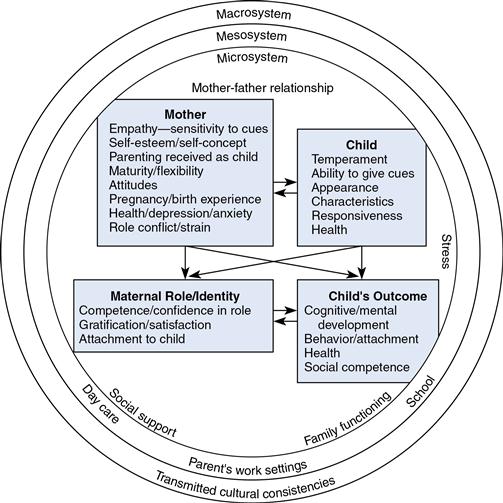
In addition to Rubin’s work, Mercer based her research on both role and developmental theories. She relied heavily on an interactionist approach to role theory, using Mead’s (1934) theory on role enactment and Turner’s (1978) theory on the core self. In addition, Thornton and Nardi’s (1975) role acquisition process helped shape Mercer’s theory, as did the work of Burr, Leigh, Day, and Constantine (1979). Werner’s (1957) developmental process theories also contributed. In addition, Mercer’s work was influenced by von Bertalanffy’s (1968) general system theory. Her model of maternal role attainment depicted in Figure 27–1 uses Bronfenbrenner’s (1979) concepts of nested circles as a means of portraying interactional environmental influences on the maternal role. The complexity of her research interest led Mercer to rely on several theoretical sources to identify and study variables that affect maternal role attainment. Although much of her work involved testing and extending Rubin’s theories, she has consistently looked to the research of others in the development and expansion of her theory.
Use of empirical evidence
Mercer selected both maternal and infant variables for her studies on the basis of her review of the literature and findings of researchers in several disciplines. She found that many factors may have a direct or indirect influence on the maternal role, adding to the complexity of her studies. Maternal factors in Mercer’s research included age at first birth, birth experience, early separation from the infant, social stress, social support, personality traits, self-concept, child-rearing attitudes, and health. She included the infant variables of temperament, appearance, responsiveness, health status, and ability to give cues. Mercer (1995) and Ferketich and Mercer (1995a, 1995b, 1995c) also noted the importance of the father’s role and applied many of Mercer’s previous findings in studying the paternal response to parenthood. Her research required numerous instruments to measure the variables of interest.
Mercer has studied the influence of these variables on parental attachment and competence over several intervals, including the immediate postpartum period and 1 month, 4 months, 8 months, and 1 year following birth (Mercer & Ferketich, 1990a, 1990b). In addition, she has included adolescents, older mothers, ill mothers, mothers dealing with congenital defects, families experiencing antepartal stress, parents at high risk, mothers who had cesarean deliveries, and fathers in her research (Mercer, 1989; Mercer & Ferketich, 1994, 1995; Mercer, Ferketich, & DeJoseph, 1993). As a recent step, she compared her findings and the basis for her original theory with current research. As a result, Mercer (2004) has proposed that the term maternal role attainment be replaced with becoming a mother, because this more accurately describes the continued evolvement of the role across the woman’s life span. In addition, she proposed using more recent nursing research findings to describe the stages and process of becoming a mother.
Major assumptions
For maternal role attainment, Mercer (1981, 1986a, 1995) stated the following assumptions:
• A relatively stable core self, acquired through lifelong socialization, determines how a mother defines and perceives events; her perceptions of her infant’s and others’ responses to her mothering, with her life situation, are the real world to which she responds (Mercer, 1986a).
• In addition to the mother’s socialization, her developmental level and innate personality characteristics also influence her behavioral responses (Mercer, 1986a).
• The mother’s role partner, her infant, will reflect the mother’s competence in the mothering role through growth and development (Mercer, 1986a).
• The infant is considered an active partner in the maternal role-taking process, affecting and being affected by the role enactment (Mercer, 1981).
• The father’s or mother’s intimate partner contributes to role attainment in a way that cannot be duplicated by any other supportive person (Mercer, 1995).
• Maternal identity develops concurrently with maternal attachment, and each depends on the other (Mercer, 1995; Rubin, 1977).
Nursing
Mercer (1995) stated that “Nurses are the health professionals having the most sustained and intense interaction with women in the maternity cycle” (p. xii). Nurses are responsible for promoting the health of families and children; nurses are pioneers in developing and sharing assessment strategies for these patients, she explained. Her definition of nursing provided in a personal communication is as follows:
Nursing is a dynamic profession with three major foci: health promotion and prevention of illness, providing care for those who need professional assistance to achieve their optimal level of health and functioning, and research to enhance the knowledge base for providing excellent nursing care. Nurses provide health care for individuals, families, and communities. Following assessment of the client’s situation and environment, the nurse identifies goals with the client, provides assistance to the client through teaching, supporting, providing care the client is unable to provide for self, and interfacing with the environment and the client
(R. Mercer, personal communication, March 21, 2004).
In her writing, Mercer (1995) refers to the importance of nursing care. In Becoming a Mother: Research on Maternal Identity from Rubin to the Present, Mercer does not specifically mention nursing care, however she emphasizes that the kind of help or care a woman receives during pregnancy and the first year following birth can have long-term effects for her and her child. Nurses in maternal-child settings play a sizable role in providing both care and information during this period.
Person
Mercer (1985a) does not specifically define person, but refers to the self or core self. She views the self as separate from the roles that are played. Through maternal individuation, a woman may regain her own personhood as she extrapolates herself from the mother-infant dyad (Mercer, 1985b). The core self evolves from a cultural context and determines how situations are defined and shaped (Mercer, 1985a). The concepts of self-esteem and self-confidence are important in attainment of the maternal role. The mother as a separate person interacts with her infant and with the father or her significant other. She is both influential and is influenced by both of them (Mercer, 1995).
Health
In her theory, Mercer defines health status as the mother’s and father’s perception of their prior health, current health, health outlook, resistance-susceptibility to illness, health worry or concern, sickness orientation, and rejection of the sick role. Health status of the newborn is the extent of disease present and infant health status by parental rating of overall health (Mercer, 1986b). The health status of a family is affected negatively by antepartum stress (Mercer, Ferketich, DeJoseph, May, & Sollid, 1988; Mercer, May, Ferketich, & DeJoseph, 1986). Health status is an important indirect influence on satisfaction with relationships in childbearing families. Health is also viewed as a desired outcome for the child. It is influenced by both maternal and infant variables. Mercer (1995) stresses the importance of health care during the childbearing and childrearing processes.
Environment
Mercer conceptualized the environment from Bronfenbrenner’s definition of the ecological environment and based her earliest model in Figure 27–1 on it (Mercer, 1995; R. Mercer, personal communication, June 24, 2000). This model illustrates the ecological interacting environments in which maternal role attainment develops. During personal communication on January 4, 2003, Mercer explained, “Development of a role/person cannot be considered apart from the environment; there is a mutual accommodation between the developing person and the changing properties of the immediate settings, relationships between the settings, and the larger contexts in which the settings are embedded.” Stresses and social support within the environment influence both maternal and paternal role attainment and the developing child.
Theoretical assertions
Mercer’s original Theory and Model of Maternal Role Attainment were introduced in 1991 during a symposium at the International Research Conference sponsored by the Council of Nursing Research and American Nurses Association in Los Angeles, California (Mercer, 1995). It was refined and presented more clearly in her 1995 book, Becoming a Mother: Research on Maternal Identity from Rubin to the Present (see Figure 27–1).
Mercer’s (2004) more recent revision of her theory has focused on the woman’s transition in becoming a mother. Motherhood involves an extensive change in a woman’s life that requires her ongoing development. According to Mercer, becoming a mother is more extensive than just assuming a role. It is unending and continuously evolving. Therefore, she proposed that the term maternal role attainment be retired. She based that recommendation on the published research of Walker, Crain, and Thompson (1986a, 1986b), Koniak-Griffin (1993), and McBride and Shore (2001), who had examined the process of mothering and raised questions about the appropriateness of maternal role attainment as an end point in the process.
Maternal role attainment: Mercer’s original model
Mercer’s Model of Maternal Role Attainment was placed within Bronfenbrenner’s (1979) nested circles of the microsystem, mesosystem, and macrosystem (see Figure 27–1). The original model proposed by Mercer was altered in 2000, changing the term exosystem, originally found in the second circle, and replacing it with the term mesosystem. Mercer (personal communication, January 4, 2003) explained that this change made the model more consistent with Bronfenbrenner’s terminology, as follows:
1. The microsystem is the immediate environment in which maternal role attainment occurs. It includes factors such as family functioning, mother-father relationships, social support, economic status, family values, and stressors. The variables contained within this immediate environment interact with one or more of the other variables in affecting the transition to motherhood. The infant as an individual is embedded within the family system. The family is viewed as a semi-closed system maintaining boundaries and control over interchange between the family system and other social systems (Mercer, 1990).
The microsystem is the most influential on maternal role attainment (Mercer, 1995; R. Mercer, personal communication, January 4, 2003). In 1995, Mercer expanded her earlier concepts and model to emphasize the importance of the father in role attainment, stating that he helps “diffuse tension developing within the mother-infant dyad” (p. 15). Maternal role attainment is achieved through the interactions of father, mother, and infant. Figure 27–2, first introduced in Mercer’s (1995) sixth book, Becoming a Mother: Research on Maternal Identity from Rubin to the Present, depicts this interaction. The layers a through d represent the stages of maternal role attainment from anticipatory to personal (role identity) and the infant’s growth and developmental stages (Mercer, 1995).
3. The macrosystem refers to the general prototypes existing in a particular culture or transmitted cultural consistencies. The macrosystem includes the social, political, and cultural influences on the other two systems. The health care environment and the current health care system policies that affect maternal role attainment originate in this system (Mercer, 1995). National laws regarding women and children and health priorities that influence maternal role attainment are within the macrosystem.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


