Modeling and role-modeling
Margaret E. Erickson
“Unconditional acceptance of the person as a human in the process of Being and Becoming is basic to the Modeling and Role-Modeling paradigm. It is a prerequisite to facilitating holistic growth …. Unconditional acceptance of the person as a human being who has an inherent need for dignity and respect from others, and for connectedness—that kind of Unconditional Acceptance is based on Unconditional Love”
(Erickson, 2006, p. 343).
Helen C. Erickson
1937 to present
Evelyn M. Tomlin
1929 to present
Mary Ann P. Swain
1941 to present
Credentials and background of the theorists
Helen C. Erickson
Helen C. Erickson received a diploma in 1957 from Saginaw General Hospital in Saginaw, Michigan. Her degrees include a baccalaureate in nursing in 1974, dual master’s degrees in psychiatric nursing and medical-surgical nursing in 1976, and a doctor of educational psychology in 1984, all from the University of Michigan. Erickson’s professional experience began in the emergency room of the Midland Community Hospital in Midland, Texas, where she was Head Nurse; she then worked as Night Supervisor at the Michigan State Home for the Mentally Impaired and Handicapped in Mount Pleasant. In 1960, she moved to Puerto Rico with her husband and was Director of Health Services at Inter-American University in San German, Puerto Rico, until 1964. On return to the United States, she was a staff nurse at St. Joseph’s and University Hospitals in Ann Arbor, Michigan. Erickson later was a mental health nurse consultant to the Pediatric Nurse Practitioner Program at University of Michigan and University of Michigan Hospitals—Adult Care.
Previous authors: Margaret E. Erickson, Jane A. Caldwell-Gwin, Lisa A. Carr, Brenda Kay Harmon, Karen Hartman, Connie Rae Jarlsberg, Judy McCormick, and Kathryn W. Noone.
The authors express appreciation to Helen C. Erickson, Evelyn M. Tomlin, and Mary Ann P. Swain for critiquing earlier editions of this chapter.
Erickson’s academic career began as Assistant Instructor in the RN Studies Program at the University of Michigan School of Nursing, and later as Chairperson of the Undergraduate Program and Dean for Undergraduate Studies. She was Assistant Professor at the University of Michigan from 1978 to 1986. In 1986, she moved to the University of South Carolina College of Nursing, where she served as Associate Professor, Assistant Dean for Academic Programs, and Associate Dean for Academic Affairs. In 1988, she became Professor of Nursing, Chair of Adult Health, and Special Assistant to the Dean, Graduate Programs, at the University of Texas School of Nursing in Austin. In 1997, she became Emeritus Professor at the University of Texas at Austin. She has maintained an independent nursing practice since 1976.
Erickson is a member of the American Nurses Association, American Nurses Foundation, the Charter Club, American Holistic Nurses Association, Texas Nurses Association, Sigma Theta Tau, and the Institute for the Advancement of Health. She served as President of the Society for the Advancement of Modeling and Role-Modeling from 1986 to 1990; as chairperson of the First National Symposium on Modeling and Role-Modeling in 1986; and on the planning boards for many national biannual conferences.
Erickson was in Who’s Who Among University Students and is a member of Phi Kappa Phi. She received the Sigma Theta Tau Rho Chapter Award of Excellence in Nursing in 1980 and the Amoco Foundation Good Teaching Award in 1982. She was accepted into ADARA (a University of Michigan honor society for women in leadership) in 1982. In 1990, she received the Faculty Teaching Award from the University of Texas School of Nursing, a Founders award from the Sigma Theta Tau International Honor Society in Nursing. She also received the Excellence in Education Award from the Epsilon Theta Chapter in 1993 and the Graduate Faculty Teaching Award from the University of Texas School of Nursing in 1995. Erickson was inducted as a Fellow into the American Academy of Nursing in 1996. She received the Distinguished Faculty citation from Humboldt State University in California in 2001. The Helen Erickson Endowed Lectureship in Holistic Health Nursing was established in her honor in 1997 at the University of Texas at Austin. The biennial lectureship highlights international holistic nursing leaders.
Erickson consults on research with the Modeling and Role-Modeling Theory and presents seminars, conferences, and papers on the theory nationally and internationally. She consults on implementation of the theory in practice at the University of Michigan Medical Center, Brigham and Women’s Hospital in Boston, Oregon Health Science University Hospital in Portland, and the University of Pittsburgh hospitals. She consults with faculty members on use of the theory into their curricula and practice in schools of nursing and service agencies. Humboldt University School of Nursing in Arcata, California, was first to use the Modeling and Role-Modeling Theory as a conceptual curriculum base. Metropolitan State University at St. Paul adopted the Modeling and Role-Modeling Theory for RN, baccalaureate, and master’s programs. St. Catherine’s College in St. Paul, Minnesota, and the Joanne Gay Dishman Department of Nursing at Lamar University have adopted it for their associate degree program.
Erickson has been invited to speak at many national and international conferences. She has been involved in activities of the American Holistic Nurses’ Association, served as a content expert for certification curricula, and was included in a book featuring nurse healers (H. Erickson, personal communication, July 1992). Although retired from the University of Texas at Austin, Erickson continues to be actively involved in the promotion of holistic nursing, serving as Chair for the Board of Directors of the American Holistic Nurses’ Certification Corporation (AHNCC) from 2002 to 2012, and she remains involved and committed to the work of the AHNCC. She provides consultation, educational programs nationally and internationally, and is actively involved in the Society for the Advancement of Modeling and Role-Modeling (H. Erickson, personal communication, June 10, 2000).
Evelyn M. Tomlin
Evelyn M. Tomlin’s nursing education began in Southern California. She attended Pasadena City College, Los Angeles County General Hospital School of Nursing, and the University of Southern California, where she received her bachelor of science degree in nursing. She received a master of science degree in psychiatric nursing from the University of Michigan in 1976.
Tomlin’s professional experiences are varied. She began as a clinical instructor at Los Angeles County General Hospital School of Nursing and later lived in Kabul, Afghanistan, where she taught English at the Afghan Institute of Technology. She served as a school nurse and practiced family nursing in the overseas American and European communities where she lived and participated in more than 46 home deliveries with a certified nurse-midwife. After she established medical services at the United States Embassy Hospital, she practiced as a staff nurse. Upon returning to the United States, she was employed by the Visiting Nurse Association (VNA) in Ann Arbor, Michigan. At the VNA, she was coordinator and clinical instructor for student practical nurses. In addition, she was a staff nurse in a coronary care unit, worked in the respiratory intensive care unit, and was Head Nurse in the emergency department at St. Joseph’s Mercy Hospital in Ann Arbor. She later taught fundamentals of nursing as Assistant Professor in the RN Studies Program at the University of Michigan. During this time, she served as mental health consultant to the pediatric nurse practitioner program at the University of Michigan.
Tomlin was among the first 16 nurses in the United States to be certified by the American Association of Critical Care Nurses. With several colleagues, she opened one of the first offices for independent nursing practice in Michigan and continued independent practice until 1993. She is a member of Sigma Theta Tau Rho Chapter, California Scholarship Federation, and the Philomathian Society. Tomlin presented programs based on the Modeling and Role-Modeling Theory, with emphasis on clinical applications. She was the first editor for the newsletter of the Society for the Advancement of Modeling and Role-Modeling (E. Tomlin, curriculum vitae, 1992).
In 1985, Tomlin moved to Big Rock, Illinois, where she enjoyed teaching small community and nursing groups and working in a community shelter serving the women and children of Fox Valley. She later moved to Geneva, Illinois, where she resides with her husband. Tomlin identifies herself as a Christian in retirement from nursing for pay, but not from nursing practice. She is pursuing interests in the practice of healing prayer, stating that she has always been interested in the interface of the Modeling and Role-Modeling Theory and Judeo-Christian principles. She is now retired after many years on the board of directors and as a volunteer at Wayside Cross Ministries in Aurora, Illinois, where she taught and counseled homeless women, many of whom were single mothers.
Mary Ann P. Swain
Mary Ann P. Swain’s educational background is in psychology. She received her bachelor’s degree in psychology from DePauw University and her master’s and doctoral degrees in psychology from the University of Michigan. Swain taught psychology, research methods, and statistics as a teaching assistant at DePauw University and later as a lecturer and professor of psychology and nursing research at the University of Michigan. At the University of Michigan, she was Director of the Doctoral Program in Nursing in 1975 for 1 year, Chairperson of Nursing Research from 1977 to 1982, and became Associate Vice President for Academic Affairs in 1983.
Swain is a member of the American Psychological Association and an associate member of the Michigan Nurses Association. She developed and taught classes in psychology, research, and nursing research methods and collaborated with nurse researchers on projects, including health promotion among diabetic patients and ways to influence compliance among patients with hypertension. She helped Erickson publish a model that assessed an individual’s potential to mobilize resources and adapt to stress, which is significant to the Modeling and Role-Modeling Theory.
Swain received the Alpha Lambda Delta, Psi Chi, Mortar Board, and Phi Beta Kappa awards while at DePauw University. In 1981, she was recognized by the Rho Chapter of Sigma Theta Tau for Contributions to Nursing, and in 1983 she became an honorary member of Sigma Theta Tau. In 1994, she moved to Appalachia, New York, with her husband, where she served as Provost and Vice President for Academic Affairs for Binghamton University for nearly 20 years. She is director of the doctoral (PhD in Nursing) program at Decker School of Nursing and Chair of the Department of Student Affairs. Her research interests are health development across the life span and interrelationships among life stressors, healthy development, and illness.
Theoretical sources
The theory and paradigm Modeling and Role-Modeling was developed with a retroductive process. The original model was derived inductively from Erickson’s clinical and personal life experiences. The works of Maslow, Erikson, Piaget, Engel, Selye, and M. Erickson MD were then integrated and synthesized into the original model to label, further articulate, and refine a holistic theory and paradigm for nursing. H. Erickson (1976) argued that people have mind-body relations and an identifiable resource potential that predicts their ability to contend with stress. She articulated a relationship between needs status and developmental processes, satisfaction with needs and attachment objects, loss and illness, and health and need satisfaction. Tomlin and Swain validated and affirmed Erickson’s practice model and helped her expand and articulate labeled phenomena, concepts, and theoretical relationships.
Maslow’s theory of human needs was used to label and articulate their personal observations that “all people want to be the best that they can possibly be; unmet basic needs interfere with holistic growth whereas satisfied needs promote growth” (Erickson, Tomlin, & Swain, 2002, p. 56; Erickson, M., 1996a, 1996b, 2006; Jensen, 1995). Erickson further developed the model to state that unmet basic needs create need deficits that can lead to initiation or aggravation of physical or mental distress or illness, while need satisfaction creates assets that provide resources needed to contend with stress and promote health, growth, and development.
Piaget’s theory of cognitive development provides a framework for understanding the development of thinking, while integration of Erik Erikson’s work on the stages of psychosocial development through the life span provides a theoretical basis for understanding the psychosocial evolution of the individual. Each of his eight stages represents developmental tasks. As an individual resolves each task, he or she gains strengths that contribute to character development and health. As an outcome of each stage, people develop a sense of their own worth and projection of themselves into the future. “The utility of Erikson’s theory is the freedom we may take to view aspects of people’s problems as uncompleted tasks. This perspective provides a hopeful expectation for the individual’s future since it connotes something still in progress” (Erickson, Tomlin, & Swain, 2002, pp. 62–63).
The works of Winnicott, Klein, Mahler, and Bowlby on object attachment were integrated with the original model to develop and articulate the concept of affiliated individuation (AI). Object relations theory proposes that an infant initially forms an attachment to his or her caregiver after having repeated positive contacts. As the child grows and begins to move toward a more separate and individuated state, a sense of autonomy develops and he or she usually transfers some attachment to an inanimate object such as a cuddly blanket or a teddy bear. Later, the child may attach to a favorite baseball glove, doll, or pet, and finally onto more abstract things in adulthood, such as an educational degree, professional role, or relationship. Erickson drew on the work of these individuals and proposed a theoretical relationship between object attachment and need satisfaction, theorizing that when an object repeatedly meets an individual’s basic needs, attachment or connectedness to that object occurs. From synthesis of these theoretical linkages and research findings, a new concept of AI was identified and defined as the inherent need to be connected with significant others at the same time that there is a sense of separateness from them (Erickson, H., 2006, 2010; Erickson, Erickson, & Jensen, 2006; Erickson, Tomlin, & Swain, 1983; Erickson, M., 1996b). From the time of birth until a person takes their last breath, AI and object attachment are essential to need satisfaction, adaptive coping, and healthy growth and development. Furthermore, “object loss results in basic need deficits” (Erickson, Tomlin, & Swain, 2002, p. 88). Loss is real, threatened, or perceived; it may be a normal part of the developmental process, or it may be situational. Loss always results in grief; normal grief is resolved in approximately 1 year. When loss occurs and only inadequate or inappropriate objects are available to meet needs, morbid grief results. Morbid grief interferes with the individual’s ability to grow and develop to their maximal potential (Erickson, Tomlin, & Swain, 2002; Erickson, M., 2006). The work of Selye and Engel, as cited by Erickson, Tomlin, and Swain (1983), provided additional conceptual support for the propositions regarding loss and an individual’s stress responses to loss or losses. Selye’s theory pertains to an individual’s biophysical responses to stress, and Engel explores the psychosocial responses to stressors.
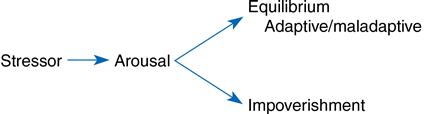
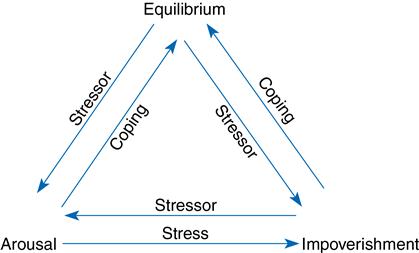
The integration and synthesis of these theories, with the integration of Erickson’s clinical observations and lived experiences, resulted in the conception of the Adaptive Potential Assessment Model (APAM). The APAM focuses on an individual’s ability to mobilize resources when confronted with stressors rather than adapt to them. This model was first developed by Erickson (1976) and later described in publication by Erickson and Swain (1982).
Erickson credits Milton H. Erickson with influencing her clinical practice and providing inspiration and direction in the development of this theory. Initially, he articulated the formulation of the Modeling and Role-Modeling Theory when he urged Erickson to “model the client’s world, understand it as they do, then role-model the picture the client has drawn, building a healthy world for them” (H. Erickson, personal communication, November 1984).
Use of empirical evidence
Several studies provided initial evidence for philosophical premises and theoretical linkages implied in the original book by Erickson, Tomlin, and Swain (1983) and later specified by Erickson (1990b). The APAM (Figures 25–1 and 25–2) has been tested as a classification model (Barnfather, 1987; Erickson, 1976; Kleinbeck, 1977) as a predictor for health status (Barnfather, 1990b) for length of hospital stay (Erickson & Swain, 1982), and as it relates to basic needs status (Barnfather, 1993). Findings from these studies provide beginning evidence for the proposed three-state model across populations, a relationship between health and ability to mobilize resources, and an ability to mobilize resources and needs status. Two other studies have shown relationships among stressors (measured as life events) and propensity for accidents (Babcock & Mueller, 1980) and resource state and ability to take in and use new information (Clementino & Lapinske, 1980). Benson (2003, 2006, 2011) studied the APAM as applied to small groups.
Relationships among self-care knowledge, resources, and activities have been demonstrated in several studies (Acton, 1993; Baas, 1992; Irvin, 1993; Jensen, 1995; Miller, 1994). The self-care knowledge construct, first studied by Erickson (1985), was replicated and found to be significantly associated with perceived control (Cain & Perzynski, 1986); perceived autonomy (Hertz & Anschutz, 2002; Matsui & Capezuti, 2008); and quality of life (Baas, Fontana, & Bhat, 1997). Self-directedness, need for harmony (affiliation), and need for autonomy (individuation) were found when multidimensional scaling was used to explore relationships among self-care knowledge, resources, and actions. The author concluded that a positive attitude was a major factor when health-directed self-care actions were assessed (Rosenow, 1991). Physical activity in patients after myocardial infarction was shown to be affected by life satisfaction (not physical condition); life satisfaction was predicted by availability of self-care resources and resources needed; and resources needed served as a suppressor for resources available (Baas, 1992). In a sample of caregivers, social support predicted for stress level and self-worth had an indirect effect on hope through self-worth (Irvin, 1993; Irvin & Acton, 1997), whereas persons with diabetes with spiritual well-being were better able to cope (Landis, 1991).
When the Modeling and Role-Modeling Theory was used as a guideline, interviews were used to determine the client’s model of the world. The following seven themes emerged (Erickson, 1990a):
1. Cause of the problem, which was unique to the individual
2. Related factors, also unique to the individual
3. Expectations for the future
5. Affiliation
Each was unique and warranted individualized interventions. Other qualitative research studies on self-care knowledge showed that acutely ill patients perceived monitoring, caring, presence, touch, and voice tones as comforting (Kennedy, 1991); healthy adults sought need satisfaction from the nurse practitioner in primary care (Boodley, 1990, 1986); and hospice patients benefited from nurse empathy (Raudonis, 1991). Additional studies addressed the experience of persons 85 years of age and older as they manage their health (Beltz, 1999), the perceptions of hope in elementary school children (Baldwin, 1996), the experiences and perceptions of mothers utilizing child health services in South Africa (Jonker, 2012), the experiential meaning of well-being and the lived experience of employed mothers (Weber, 1995, 1999), the meaning and impact of suffering in people with rheumatoid arthritis (Dildy, 1992), the relationship between experiences of prolonged family suffering and evolving spiritual identity (Clayton, 2001), the quality of life of older adults with urinary incontinence (Liang, 2008), and the human-environment relationship when healing from an episodic illness (Bowman, 1998).
Case study methods have shown relationships among needs, attachment, and developmental residual needs (Kinney, 1990, 1992; Kinney & Erickson, 1990) and coping (Jensen, 1995), and challenges in the treatment of Factitious Disorder (Hagglund, 2009).
Studies revealed relationships among mistrust and length of stay in hospitalized subjects (Finch, 1990); perceived enactment of autonomy, self-care, and holistic health in older adults (Anschutz, 2000; Hertz & Anschutz, 2002); perceived enactment of autonomy and self-care resources among senior center users (Matsui & Capezuti, 2008) ; perceived enactment of autonomy, self-care, perceived support, control, and well being in older adults (Chen, 1996); perceived enactment of autonomy and related sociodemographic factors among older adults (Hwang & Lin, 2004); loss, morbid grief, and onset of symptoms of Alzheimer’s disease (Erickson, Kinney, Becker, et al., 1994; Irvin & Acton, 1996); and basic needs satisfaction and health-promoting self-care behaviors in adults (Acton & Malathum, 2000).
Other studies addressed linkages between role-modeled interventions and outcomes (Erickson, Kinney, Becker, et al., 1994; Hertz, 1991; Irvin, 1993; Jensen, 1995; Kennedy, 1991, Lamb, 2005; Sung &Yu, 2006). University students who perceived satisfaction of needs were more successful in school (Smith, 1980), older adults who felt supported reported higher need satisfaction and were better able to cope (Keck, 1989), adolescent mothers who felt supported and perceived need satisfaction had a more positive maternal-infant attachment (Erickson, M., 2006; Erickson, 1996a, 1996b), those with a strong social network reported better health (Doornbos, 1983), and persons convicted of sexual offenses who were provided with support to remodel their worlds were able to develop new behaviors and move on with their lives (Scheela, 1991). Families and post–myocardial infarction patients who were able to participate in planning their own care through contracting had less anxiety and better perceived control and perceived support (Holl, 1992). Caregivers of adults with dementia who experienced theory-based nursing using the Modeling and Role-Modeling Theory perceived that their needs were met and were healthier (Hopkins, 1995), and they were encouraged, which helped them accept the situation and transcend the experience of caregiving (Hopkins, 1995). Self-care resources, measured as needs, are related to perceived support and coping in women with breast cancer (Keck, 1989), physical well-being in persons with chronic obstructive pulmonary disease (Leidy, 1990; Kline,1988), and anxiety in hospitalized patients who have had cardiac surgery and their families (Holl, 1992). Finally, when AI was tested as a buffer between stress and well-being, a mediation effect was found (Acton, 1997; Acton, 1993; Acton, Irvin, Jensen, et al., 1997).
Additional studies that operationalize self-care resources by measuring developmental residuals have shown that identity resolution in adolescents with facial disfiguration can be predicted by previous developmental residual (Miller, 1986). Chen (1996) found that feelings of control over one’s health (health control orientation) status in older adults with hypertension correlated highly with self-efficacy and self-care. In addition, her work supported that health control orientation, self-efficacy, and self-care were associated with well-being. Through interviews of older adults living independently, Hertz, Rossetti, and Nelson (2006) were able to identify categories of self-care actions that encompassed important self-care activities.
Other researchers found that trust predicts for adolescent clients’ involvement in the prescribed medical regimen (Finch, 1987); perceived support and adaptation are related to developmental residual in families with newborn infants (Darling-Fisher, 1987; Darling-Fisher & Leidy 1988); and mistrust predicts length of hospital stay, and positive residual serves as a buffer (Finch, 1987). Positive residual in the intimacy stage of healthy adults predicts for health behaviors (MacLean, 1987, 1990, 1992). Developmental residual predicts for hope, trust-mistrust residual predicts for generalized hope, autonomy-shame and doubt residual predicts for particularized hope in the elderly (Curl, 1992); and negative residual is related to speed and impatience behaviors in a healthy sample of military personnel (Kinney, 1992).
Studies have also been used to explore perceived enactment of autonomy and life satisfaction in older adults (Anschutz, 2000), self-care knowledge in informants in the hospital (Erickson, 1985), developmental growth in adults with heart failure (Baas, Beery, Fontana, & Wagoner, 1999), the ability to mobilize coping resources and basic needs (Barnfather, 1990a), the relationship between basic needs satisfaction and emotionally motivated eating (Timmerman & Acton, 2001; Cleary, & Crafti, 2007), and relations among hostility, self-esteem, self-concept, and psychosocial residual in persons with coronary heart disease (Sofhauser, 1996, 2003). Research has also been conducted that explores the relationship between spiritual well-being and heart failure (Beery, Baas, Fowler, & Allen, 2002); spirituality in caregivers of family members with dementia (Acton & Miller, 1996); the implementation of a mind, body, spirit self-empowerment program for adolescents (Nash, 2007a); and spirituality in women with breast cancer (Kinney, Rodgers, Nash, & Bray, 2003). Baas (2004) studied self-care resources and quality of life in patients following myocardial infarction and self-care resources and well-being in clients with cardiac disorders (2011). She and colleagues also examined the psychosocial aspects of heart failure management (Baas & Conway, 2004), explored body awareness in heart failure or transplant patients (Baas, Beery, Allen, et al., 2004), and reported patient adjustments to the cardiac devices (Beery, Baas, & Henthorn, 2007).
Tools that have been developed to test the Modeling and Role-Modeling Theory include the Basic Needs Satisfaction Inventory (Kline, 1988), the Erikson Psychosocial Stage Inventory (Darling-Fisher & Leidy, 1988), the Perceived Enactment of Autonomy tool designed to measure a prerequisite to self-care actions in the elderly (Hertz, 1991, 1999; Hertz & Anschutz, 2002), the Self-Care Resource Inventory (Baas, 1992, 2011), an adjustment scale designed to measure self-report with implanted devices in cardiac patients (Beery, Baas, Mathews, et al., 2005), the Robinson Self-Appraisal Inventory designed to measure denial (the first stage in the grief process) in patients after myocardial infarction (Robinson, 1992), the Erickson Maternal Bonding-Attachment Tool designed to measure self-care knowledge as motivational style (deficit or being motivated) and self-care resource (maternal need satisfaction) (Erickson, 1996b), a theory-based nursing assessment (Finch, 1990), and the Hopkins Clinical Assessment of the APAM (Hopkins, 1995).
Major assumptions
Nursing
“The nurse is a facilitator, not an effector. Our nurse-client relationship is an interactive, interpersonal process that aids the individual to identify, mobilize, and develop his or her own strengths to achieve a perceived optimal state of health and well-being” (H. Erickson, personal communication, 2004). Rogers (1996) has defined this relationship as facilitative-affiliation. The five aims of nursing interventions are to build trust, affirm and promote client strengths, promote positive orientation, facilitate perceived control, and set health-directed mutual goals (Erickson, Tomlin, & Swain, 2002).
Person
Differentiation is made between patients and clients in this theory. A patient is given treatment and instruction; a client participates in his or her own care. “Our goal is for nurses to work with clients” (Erickson, Tomlin, & Swain, 2002, p. 21). “A client is one who is considered to be a legitimate member of the decision-making team, who always has some control over the planned regimen, and who is incorporated into the planning and implementation of his or her own care as much as possible” (Erickson, Kinney, Stone, et al., 1990, p. 20; Erickson, Tomlin, & Swain, 2002, p. 253).
Health
“Health is a state of physical, mental, and social wellbeing, not merely the absence of disease or infirmity. It connotates a state of dynamic equilibrium among the various subsystems [of a holistic person]” (Erickson, Tomlin, & Swain, 2002, p. 46).
Environment
“Environment is not identified in the theory as an entity of its own. The theorists see environment in the social subsystems as the interaction between self and others both cultural and individual. Biophysical stressors are seen as part of the environment” (H. Erickson, personal communication, March 30, 1988).
Theoretical assertions
The theoretical assertions of the Modeling and Role-Modeling Theory are based on the linkages between completion of developmental tasks and basic needs satisfaction; among basic needs satisfaction, object attachment and loss, and developmental tasks; and between the ability to mobilize coping resources and need satisfaction. Three generic theoretical assertions constitute theoretical linkages implied in the theory as follows:
1. “The degree to which developmental tasks are resolved is dependent on the degree to which human needs are satisfied” (Erickson, Tomlin, & Swain, 2002, p. 87).
2. “The degree to which needs are satisfied by object attachment depends on the availability of those objects and the degree to which they provide comfort and security as opposed to threat and anxiety” (Erickson, Tomlin, & Swain, 1983, p. 90).
3. “An individual’s potential for mobilizing resources, the person’s state of coping according to the APAM, is directly associated with the person’s need satisfaction level” (Erickson, Tomlin, & Swain, 2002, p. 91).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


