On completion of this chapter, the reader will be able to: • Define the terms mortality and morbidity. • Identify two ways that knowledge of mortality and morbidity can improve child health. • List three major causes of death during infancy, early childhood, later childhood, and adolescence. • List two major causes of illness during childhood. • Describe five broad functions of the pediatric nurse in promoting the health of children. • Define the term critical thinking. • Identify the five steps of the nursing process. • Define the term nursing diagnosis. The major goal for pediatric nursing is to improve the quality of health care for children and their families. In 2011, almost 74 million children 0 to 17 years of age lived in the United States, comprising 23.7% of the population (Forum on Child and Family Statistics, 2012). The health status of children in the United States has improved in a number of areas, including increased immunization rates for all children, decreased adolescent birth rate, and improved child health outcomes. Unfortunately, millions of children and their families have no health insurance, which results in a lack of access to care and health-promotion services. In addition, disparities in pediatric health care are related to race, ethnicity, socioeconomic status, and geographic factors. Patterns of child health are shaped by medical progress and societal trends (Starmer, Duby, Slaw, et al., 2010). Shifts in population demographics, family structure, income, education levels, and cultural norms directly affect the health of children (Leslie, Slaw, Edwards, et al., 2010). The Healthy People 2020 leading health indicators (Box 26-1) provide a framework for identifying essential components for child health–promotion programs designed to prevent future health problems in our nation’s children. Many leading causes of disease, disability, and death in children (i.e., prematurity, nutritional deficiencies, injuries, chronic lung disease, obesity, cardiovascular disease, depression, violence, substance abuse, and human immunodeficiency virus/acquired immunodeficiency syndrome [HIV/AIDS]) can be significantly reduced or prevented in children and adolescents by addressing six categories of behavior (World Health Organization, 2011): 2. Behavior that results in injury and violence 4. Dietary and hygienic practices that cause disease 6. Sexual behavior that causes unintended pregnancy and disease Child health promotion provides opportunities to reduce differences in current health status among members of different groups and ensure equal opportunities and resources to enable all children to achieve their fullest health potential. Dental caries is the single most common chronic disease of childhood (Cheng, Han, and Gansky, 2008; Heuer, 2007). Nearly one in five children between the ages of 2 and 4 years has visible cavities (Kagihara, Niederhauser, and Stark, 2009). The most common form of early dental disease is early childhood caries, which may begin before the first birthday and progress to pain and infection within the first 2 years of life (Kagihara, Niederhauser, and Stark, 2009). Preschoolers of low-income families are twice as likely to develop tooth decay and only half as likely to visit the dentist as other children. Early childhood caries is a preventable disease, and nurses play an essential role in educating children and parents about practicing dental hygiene beginning with the first tooth eruption; drinking fluoridated water, including bottled water; and instituting early dental preventive care. Changes in modern society, including advancing medical knowledge and technology, the proliferation of information systems, economically troubled times, and various changes and disruptive influences on the family, are leading to significant medical problems that affect the health of children (Leslie, Slaw, Edwards, et al., 2010). Recent concern has focused on groups of children who are at highest risk, such as children born prematurely or with very low birth weight (VLBW) or low birth weight (LBW), children attending child care centers, children who live in poverty or are homeless, children of immigrant families, and children with chronic medical and psychiatric illness and disabilities. In addition, these children and their families face multiple barriers to adequate health, dental, and psychiatric care. The new morbidity, also known as pediatric social illness, refers to the behavior, social, and educational problems that children face. Problems that can negatively impact a child’s development include poverty, violence, aggression, noncompliance, school failure, and adjustment to parental separation and divorce. In addition, mental health issues cause challenges in childhood and adolescence. Childhood obesity is the most common nutritional problem among American children, is increasing in epidemic proportions, and is associated with type 2 diabetes (Cali and Caprio, 2008; de Onis, Blössner, and Borghi, 2010; Matyka, 2008; Raj and Kumar, 2010). Obesity in children and adolescents is defined as a body mass index (BMI) at or greater than the 95th percentile for youth of the same age and gender (Schwartz and Chadha, 2008). The National Health and Nutrition Examination Survey reported that the prevalence of overweight children doubled and the prevalence of overweight adolescents tripled between 1980 and 2000 (American Dietetic Association, 2008). Advancements in entertainment and technology such as television, computers, and video games have contributed to the growing childhood obesity problem in the United States. In the National Longitudinal Study of Adolescent Health, screen time (TV, video, computer use) interacts with genetic factors to influence BMI changes (Graff, North, Monda, et al., 2011). Lack of physical activity related to limited resources, unsafe environments, and inconvenient play and exercise facilities, combined with easy access to television and video games, increases the incidence of obesity among low-income, minority children. Overweight youth have increased risk for developing hypercholesterolemia, insulin resistance, diabetes, hypertension, and heart disease (Matyka, 2008; Schwartz and Chadha, 2008) (Fig. 26-1). The U.S. Department of Health and Human Services suggests that nurses focus on prevention strategies to reduce the incidence of overweight children from the current 20% in all ethnic groups to less than 6%. Injuries are the most common cause of death and disability to children in the United States (Schnitzer, 2006) (Table 26-1). Motor vehicle accidents (MVAs) continue to be the most common cause of death in children older than 1 year. Other unintentional injuries (choking, drowning, fires, and firearm accidents) take the lives of children every day. Many childhood injuries and fatalities could be prevented by implementing programs of accident prevention and health promotion. TABLE 26-1 MORTALITY FROM LEADING TYPES OF UNINTENTIONAL INJURIES, UNITED STATES, 2008 (RATE PER 100,000 POPULATION IN EACH AGE-GROUP) Adapted from National Safety Council: Injury facts, 2012 Edition, Itaska, IL, 2012, Author. Data from National Center for Health Statistics and US Census Bureau. The type of injury and the circumstances surrounding it are closely related to normal growth and development (Box 26-2). As children develop, their innate curiosity compels them to investigate the environment and to mimic the behavior of others. This is essential to acquire competency as an adult but can also predispose children to numerous hazards. The pattern of deaths caused by unintentional injuries, especially from MVAs, drowning, and fires, is remarkably consistent in most Western societies. The leading causes of death from injuries for each age-group according to gender are presented in Table 26-1. The majority of deaths from injuries occur in boys. It is important to note that accidents continue to account for more than 3 times as many teen deaths as any other cause (Annie E. Casey Foundation, 2009). Fortunately, prevention strategies such as the use of car restraints, bicycle helmets, and smoke detectors have significantly decreased fatalities for children. Nevertheless, the overwhelming causes of death in children are MVAs, including occupant, pedestrian, bicycle, and motorcycle deaths; these account for more than half of all injury deaths (Centers for Disease Control and Prevention [CDC], 2006). Children older than 1 year of age have the highest rate of death from MVAs, primarily from a failure to properly use car restraints (Fig. 26-2). Bicycle-associated injuries also cause a number childhood deaths. Children ages 5 to 9 years are at greatest risk for bicycling fatalities. The majority of bicycling deaths are from head injuries. Helmets greatly reduce the risk for head injury, but few children wear helmets (Castle, Burke, Arbogast, et al., 2010). Community-wide bicycle helmet campaigns and mandatory-use laws have resulted in significant increases in helmet use. Still, issues such as stylishness, comfort, and social acceptability remain important factors in noncompliance. Nurses can educate children and families about pedestrian and bicycle safety. In particular, school nurses can promote helmet wearing and encourage peer leaders to act as role models. Drowning and burns are among the top three leading causes of deaths for males and females throughout childhood (Fig. 26-3). In addition, improper use of firearms is a major cause of death among males (Fig. 26-4). During infancy, more boys die from aspiration or suffocation than do girls (Fig. 26-5). Approximately 70% of all unintentional poisonings are reported in children younger than 2 years (Bronstein, Spyker, Cantilena, et al., 2008; Franklin and Rodgers, 2008) (Fig. 26-6). By ages 4 to 5 years, unintentional poisonings are uncommon. Intentional poisoning, associated with drug and alcohol abuse and suicide attempt, is the second leading cause of death in adolescent females and third leading cause in adolescent males. Youth violence is a high-visibility, high-priority concern in every sector of U.S. society. (U.S. Department of Health and Human Services, 2011). Strikingly higher homicide rates are found among minority populations, especially African-American children. The causes of violence against children and self-inflicted violence are not fully understood. Violence seems to permeate American households through television programs, commercials, video games, and movies, all of which tend to desensitize the child toward violence. Violence also permeates the schools with the availability of guns, illicit drugs, and gangs. The problem of child homicide is extremely complex and involves numerous social, economic, and other influences. Prevention lies in better understanding of the social and psychologic factors that lead to the high rates of homicide and suicide. Nurses need to be especially aware of young people who harm animals or start fires, are depressed, are repeatedly in trouble with the criminal justice system, or are associated with groups known to be violent. Prevention requires early identification and rapid therapeutic intervention by qualified professionals. Pediatric nurses can assess children and adolescents for risk factors related to violence. Families who own firearms must be educated about their safe use and storage. The presence of a gun in a household increases the risk for suicide by about fivefold and the risk for homicide by about threefold. Technologic changes such as childproof safety devices and loading indicators could improve the safety of firearms (see Community Focus box). Violence in Children Violent crimes continue to be a significant health issue for children, with homicide being the second leading cause of death in 15- to 19-year-olds (Annie E. Casey Foundation, 2009). The multifaceted origins of violence include developmental factors, gang involvement, access to firearms, drugs, the media, poverty, and family conflict. Often the silent and underrecognized victims are the children who witness acts of community violence. Studies suggest that chronic exposure to violence has a negative effect on a child’s cognitive, social, psychologic, and moral development. Also, multiple exposures to episodes of violence do not inoculate children against the negative effects; continued exposure can result in lasting symptoms of stress. Children living with chronic violence may exhibit behaviors such as difficulty concentrating in school, memory impairment, aggressive play, uncaring behaviors, and constricted activities and thinking for fear of reliving the traumatic event. Risk-taking behaviors, particularly in males, tend to begin in the first decade of life and continue into adolescence with drinking alcohol while driving, speeding, carrying a weapon, or using illicit drugs. Adolescent trends in cigarette smoking, alcohol use, and illicit drug abuse have declined since 2002. Approximately 9.8% of youth reported cigarette smoking, 15.9% reported alcohol use, and 9.5% reported illicit drug abuse within the past month (National Survey on Drug Use and Health, 2008). The slight decline in American youth’s illicit drug use is attributed to education regarding the adverse effects of illicit drugs, parental disapproval, decreased availability of drugs, and consistent participation in church and organized activities such as scouts and sports. One out of 5 adolescents has a mental health problem, and 1 out of 10 has a serious emotional problem that affects daily functioning (Coury, 2006). Psychosocial problems in children seen in primary care settings in rural areas are common (Polaha, Dalton, and Allen, 2011). Children and adolescents with mental health problems are more likely to drop out of school than those with other disabilities (Polaha, Dalton, and Allen, 2011). Suicide is defined as a self-chosen death and is the third leading cause of death in children ages 10 to 19 years (Doucette, 2005). The American Association of Suicidology (2009) estimates that there are 11.5 youth suicides (15-24 years) every day. Suicide is preventable. Nurses should be alert to the symptoms of mental illness and potential suicidal ideation and be aware of potential resources for high-quality integrated mental health services. The infant mortality rate is the number of deaths during the first year of life per 1000 live births. It may be further divided into neonatal mortality (<28 days of life) and postneonatal mortality (28 days to 11 months). In the United States, infant mortality has decreased dramatically. At the beginning of the twentieth century, the rate was approximately 200 infant deaths per 1000 live births. Based on preliminary data the infant mortality rate was 6.05 deaths per 1000 live births in 2011 (Hamilton, Hoyert, Martin, et al., 2013; Hoyert and Xu, 2012). From a worldwide perspective, however, the United States lags behind other nations in reducing infant mortality. In 2010 the United States ranked number 30 among nations with 40,000 births or more. Hong Kong, Japan, and Finland have the three lowest rates, with the United States ranked thirtieth behind Hungary and the Slovack Republic (Hamilton, Hoyert, Martin, et al., 2013). Birth weight is considered the major determinant of neonatal death in technologically developed countries. The lower the birth weight, the higher the mortality. The relatively high incidence of LBW (<2500 g [5.5 pounds]) in the United States is considered a key factor in its higher neonatal mortality rate when compared with other countries. Access to and the use of high-quality prenatal care is a promising preventive strategy to decrease early birth and infant mortality. Other factors that increase the risk for infant mortality include African-American race, male gender, short or long gestation, maternal age, and lower level of maternal education (Martin, Kochanek, Strobino, et al., 2005). As Table 26-2 demonstrates, many of the leading causes of death during infancy continue to occur during the perinatal period. The first four causes—congenital anomalies, disorders relating to short gestation and unspecified LBW, sudden infant death syndrome, and newborn affected by maternal complications of pregnancy—accounted for about half (52%) of all deaths of infants younger than 1 year (Hamilton, Hoyert, Martin, et al., 2013). LBW is a major indicator of infant health and a significant predictor of infant mortality (Hamilton, Hoyert, Martin, et al., 2013). Many birth defects are associated with LBW, and reducing the incidence of LBW will help prevent congenital anomalies. Infant mortality resulting from HIV infection decreased significantly during the 1990s. TABLE 26-2 INFANT MORTALITY RATE AND PERCENTAGE OF TOTAL DEATHS FOR 10 LEADING CAUSES OF INFANT DEATH IN 2011 (RATE PER 1000 LIVE BIRTHS)*
21st Century Pediatric Nursing
Health Care for Children
Health Promotion
Dental Care
Childhood Health Problems
Obesity and Type 2 Diabetes
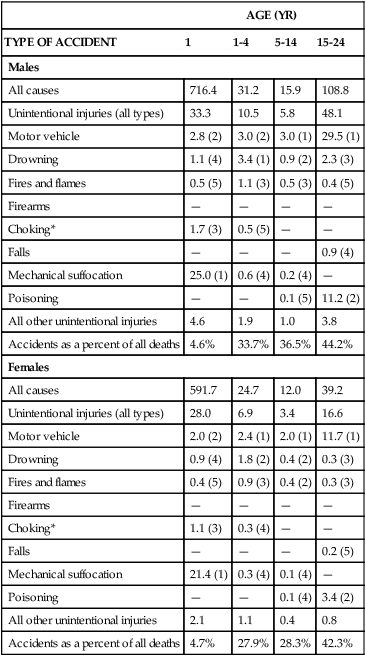
Childhood Injuries
AGE (YR)
TYPE OF ACCIDENT
1
1-4
5-14
15-24
Males
All causes
716.4
31.2
15.9
108.8
Unintentional injuries (all types)
33.3
10.5
5.8
48.1
Motor vehicle
2.8 (2)
3.0 (2)
3.0 (1)
29.5 (1)
Drowning
1.1 (4)
3.4 (1)
0.9 (2)
2.3 (3)
Fires and flames
0.5 (5)
1.1 (3)
0.5 (3)
0.4 (5)
Firearms
—
—
—
—
Choking*
1.7 (3)
0.5 (5)
—
—
Falls
—
—
—
0.9 (4)
Mechanical suffocation
25.0 (1)
0.6 (4)
0.2 (4)
—
Poisoning
—
—
0.1 (5)
11.2 (2)
All other unintentional injuries
4.6
1.9
1.0
3.8
Accidents as a percent of all deaths
4.6%
33.7%
36.5%
44.2%
Females
All causes
591.7
24.7
12.0
39.2
Unintentional injuries (all types)
28.0
6.9
3.4
16.6
Motor vehicle
2.0 (2)
2.4 (1)
2.0 (1)
11.7 (1)
Drowning
0.9 (4)
1.8 (2)
0.4 (2)
0.3 (3)
Fires and flames
0.4 (5)
0.9 (3)
0.4 (2)
0.3 (3)
Firearms
—
—
—
—
Choking*
1.1 (3)
0.3 (4)
—
—
Falls
—
—
—
0.2 (5)
Mechanical suffocation
21.4 (1)
0.3 (4)
0.1 (4)
—
Poisoning
—
—
0.1 (4)
3.4 (2)
All other unintentional injuries
2.1
1.1
0.4
0.8
Accidents as a percent of all deaths
4.7%
27.9%
28.3%
42.3%


Violence
 Community Focus
Community Focus
Substance Abuse
Mental Health Problems
Mortality and Morbidity
Infant Mortality
RANK
CAUSE OF DEATH (BASED ON 10TH REVISION, INTERNATIONAL CLASSIFICATION OF DISEASES)
PERCENT
RATE
All races, all causes
100.00%
604.7
1
Congenital anomalies
20.8
126.1
2
Disorders relating to short gestation and unspecified low birth weight
17.2
104.1
3
Sudden infant death syndrome
7.2
43.3
4
Newborn affected by maternal complications of pregnancy
6.6
39.9
5
Accidents (unintentional injuries)
4.6
27.5
6
Newborn affected by complications of placenta, cord, and membranes
4.1
25.1
7
Bacterial sepsis of newborn
2.2
13.3
8
Respiratory distress of newborn
2.1
13.0
9
Diseases of circulatory system
2.1
12.5
10
Neonatal hemorrhage, asphyxia
1.9
11.2 ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


21st Century Pediatric Nursing



Get Clinical Tree app for offline access
