The Infant
Objectives
1. Define each key term listed.
3. Discuss the major aspects of cognitive development in the first year of life.
5. Discuss the nutritional needs of growing infants.
6. Compare breastfeeding, bottle feeding, and the various infant formulas available.
7. Describe how to select and prepare solid foods for the infant.
8. List four common concerns of parents about the feeding of infants.
9. Discuss the development of feeding skills in the infant.
10. Compare and contrast natural, organic, and processed foods.
11. Examine nutritional counseling for the infant.
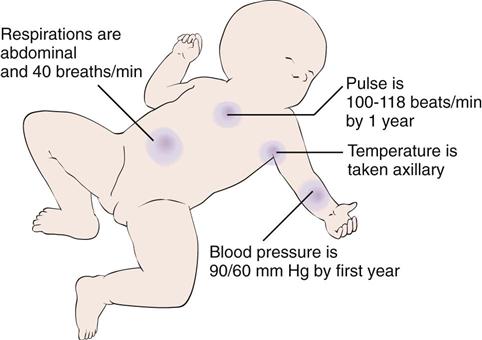
13. Describe normal vital signs for a 1-year-old infant.
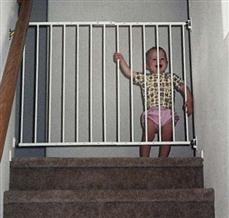
14. Discuss safety issues in the care of infants.
15. Discuss the approach to and the specifics of care of an infant with colic.
16. Identify age-appropriate toys and their developmental or therapeutic value.
17. Discuss principles of safety during infancy.
Key Terms
colic (p. 395)
extrusion reflex (ĕks-TRŪ-zhŭn RĒ-flĕks, p. 397)
grasp reflex (p. 387)
milestones (p. 386)
norms (p. 386)
object permanence (p. 404)
oral stage (p. 387)
parachute reflex (p. 387)
pincer grasp (p. 387)
prehension (p. 387)
satiety (să-TĪ-ĕ-tē, p. 398)
weaning (p. 403)
 http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Physical, emotional, and cognitive growth and the development of motor abilities occur rapidly during the first year of life. Milestones of growth and development describe general patterns of achievements at various stages of infancy. These milestones, or patterns, are referred to as norms. Norms can vary greatly for the individual child, but the nurse must understand the normal range for milestone achievement to assess the progress of growth and development of the infant and initiate early referral for follow-up care.
During the neonatal phase of development, the chief tasks mastered were the establishment of effective feeding patterns and a predictable sleep-wake cycle. Infants who have unmet hunger needs can become irritable, may not perceive feeding as pleasurable, and may fail to develop trust in the caregiver. Parental bonding and social interaction begin in the neonatal phase but heighten when the infant begins to respond with a social smile, making the caregiver feel “loved.”
By the time the infant is age 4 to 6 months, the positive parental interaction with the infant should be obvious during clinic visits. If the parent does not appear to enjoy the developmental changes in the infant at this age or does not appear relaxed during interactions with the infant, further follow-up of possible family dysfunction or social or mental stresses should be initiated.
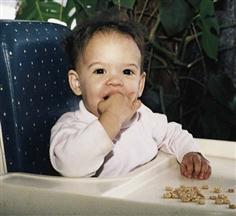
By age 9 months, control of feeding may become an issue of conflict between parent and infant. The parent needs to “let go” and introduce the infant to finger foods and initiate drinking from a cup. Offering limited choices can reduce conflict as the infant reaches toward autonomy. If the nurse notices an overly neat and orderly approach during feeding, parental guidance may be necessary. Separation anxiety (see Chapter 21) can be expected by the ninth-month clinic visit, and the nurse should expect to spend some time playing with the infant and getting to know the infant to establish the rapport necessary for a successful physical assessment. Repetition is the key to successful parent teaching and counseling by the nurse.
Children, unlike adults, are in the process of growing while they are hospitalized. To provide total patient care, the nurse must be able to recognize a patient’s needs at various stages of growth and development. The pulse rate, respiration, and blood pressure measurements that are normal for an infant are not normal for the adult patient (Figure 16-1). The nurse must try to meet individual needs effectively and to administer the specialized nursing care required for the particular patient. The most common cause for concern about a child is a sudden slowing, not typical for age, of any aspect of development.
General Characteristics
Oral Stage
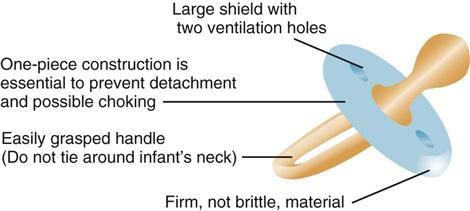
Sucking brings the infant comfort and relief from tension. This oral stage of personality development is important for the infant’s physical and psychological development. The nurse, knowing the importance of sucking to the infant, holds the infant during feedings and allows sufficient time to suck. Infants who are warm and comfortable associate food with love. The infant who is fed intravenous fluids is given added attention and a pacifier to ensure the necessary satisfaction of sucking (Figure 16-2). When the teeth appear, the infant learns to bite and enjoys objects that can be chewed. Gradually, the infant begins to put fingers into the mouth. When infants can use their hands more skillfully, they will not suck their fingers as often and will be able to derive pleasure from other sources.
Motor Development
The grasp reflex is seen when one touches the palms of the infant’s hands and flexion occurs. This reflex disappears at about 3 months. Prehension, the ability to grasp objects between the fingers and the opposing thumb, occurs slightly later (age 5 to 6 months) and follows an orderly sequence of development (Figure 16-3).
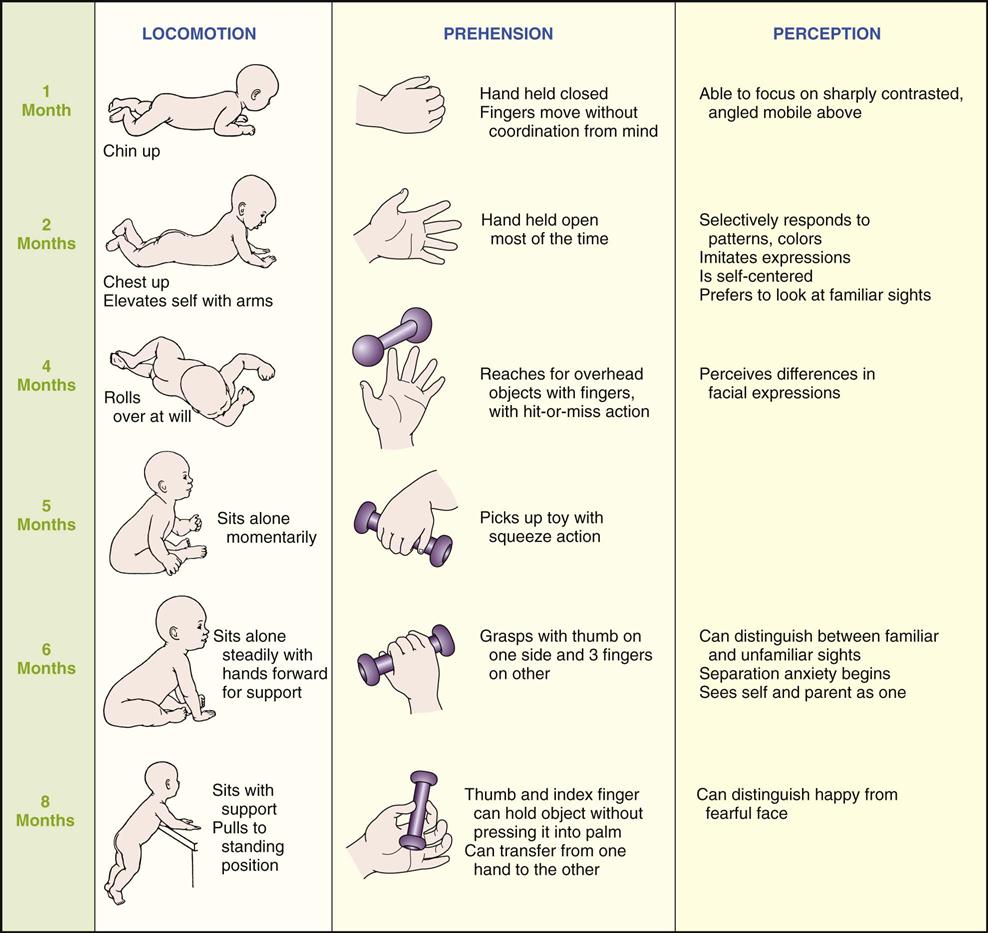
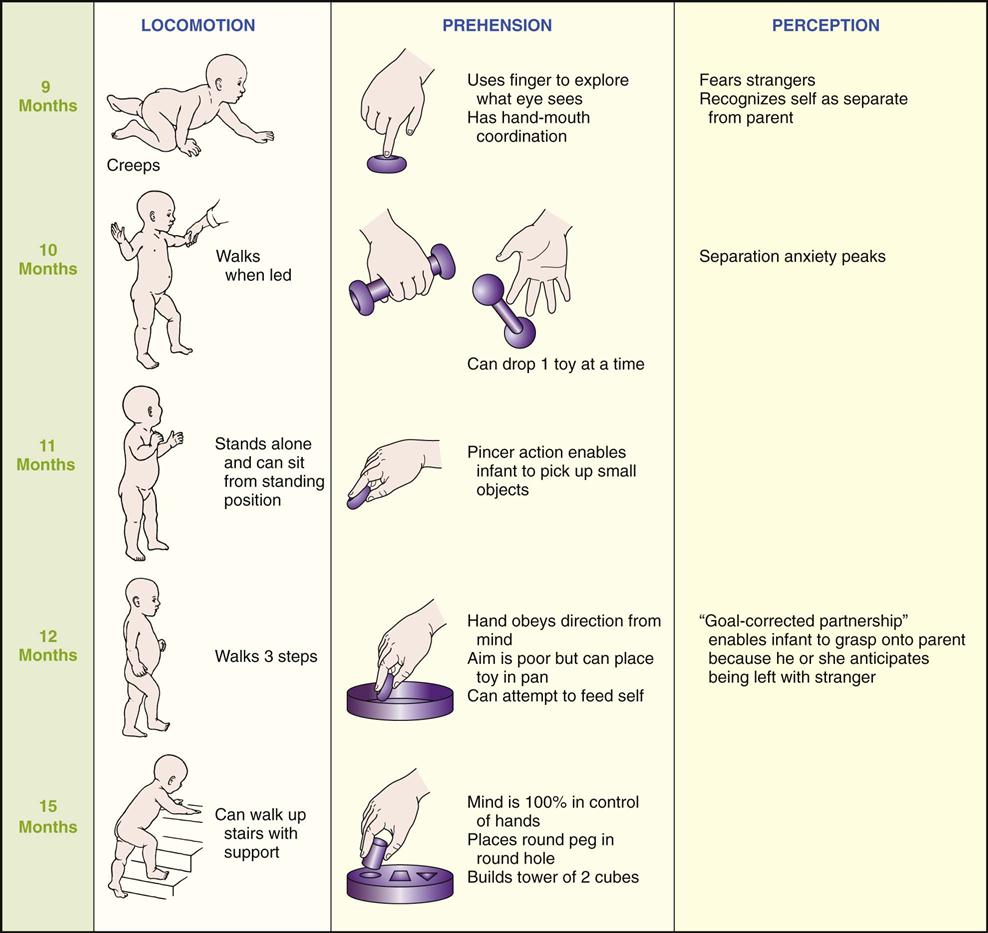
The parachute reflex appears by age 7 to 9 months. This is a protective arm extension that occurs when an infant is suddenly thrust downward when prone. By age 1 year the pincer grasp coordination of index finger and thumb is well-established.
Emotional Development
Love and security are vital needs of infants. They require the continuous affection of their parents. If trust is to develop, consistency must be established. Parents are assured that they need not be afraid of spoiling their infants by attending promptly to their needs. Infants who are consistently picked up in response to crying show fewer crying episodes when they are toddlers and less aggressive behavior at age 2 years. Loving adults affirm that the world is a good place in which to live. Each day the infant becomes impressed by parental actions and learns to imitate and trust caregivers. A sense of trust is vital to the development of a healthy personality. Many consider it to be the foundation of emotional growth. The child who does not develop a sense of trust learns to mistrust people, which could have a permanently negative effect on personality development.
Parents are taught to talk, sing, and touch their infants while providing care. They should not expect too much or too little from them. Infants will easily accomplish various activities if they are not forced before they reach readiness. When an infant shows readiness to learn a task, parents should provide encouragement.
 Nursing Tip
Nursing Tip
Parental approval is important to the infant, and setting limits early is important (Anderson, 2008). Principles of discipline at this age include the following:
Need for Constant Care and Guidance
The full-time caregiver needs and deserves the understanding of and kind support from relatives at home and from the nurse in the hospital. Pediatrics involves family-centered care. A short break from pressures provides renewed energy with which to enjoy the infant. A trip to the store or a stroll with the infant in the carriage affords stimulation and a change of environment for the infant and the caregiver. The infant who is constantly left in a crib or playpen and is not introduced to a variety of learning experiences may become shy and withdrawn. Sensory stimulation is essential for the development of the infant’s thought processes and perceptual abilities.
If a mother is unable to room-in with her hospitalized infant, personnel should try to imitate her care by promptly fulfilling the infant’s physical and emotional needs. In the nursery the nurse first feeds the infant who appears hungry, rather than delaying feeding to adhere to a specific routine. Wet diapers are changed as soon as possible. The crying child is soothed. The exactness of time or method of bathing or feeding the infant is less important than the care with which it is done. The infant easily recognizes warmth and affection or the lack thereof.
Development and Care
Box 16-1 is a guide to infant care from the first month to the first birthday. Some of the aspects of care (e.g., safety measures) are important throughout the entire year. The nurse explains to parents that physical patterns cannot be separated from social patterns and that abrupt changes do not take place with each new month. Human development cannot be separated into specific areas any more than the body’s structure can be separated from its function.
Box 16-1
Physical Development, Social Behavior, and Care and Guidance of Infants
1 Month
Physical Development

Social Behavior
Care and Guidance
2 Months
Physical Development
Care and Guidance
Sleep: Develops own pattern; may sleep from feeding to feeding.
Pacifier: If used, select for safety. Choose one-piece construction and loop handle to prevent aspiration (see Figure 16-2).
Hiccups: Are normal and subside without treatment. Small amounts of water may help.
Colic: Consists of paroxysmal abdominal pain, irritable crying. Usually disappears after 3 months. Place infant prone over arms (see Chapter 22, Figure 22-4, D). Use pacifier. Massage back. Relieve caregiver periodically.
3 Months
Physical Development
Care and Guidance
Social Behavior
4 Months
Physical Development
Care and Guidance
Sleep: Stirs about in crib. Sleeps through ordinary household noises.
Diet: Mother’s milk or formula.
Immunization: Second DTaP, IPV, and Hib.
Elimination: One or two bowel movements per day. May skip a day.
5 Months
Physical Development
Social Behavior

Care and Guidance
6 Months
Physical Development
 inch) per month. Sits alone momentarily. Springs up and down when sitting. Turns completely over. Hitches (moves backward when sitting). Bangs table with rattle. Pulls to a sitting position. Chewing more mature. First solid food introduced. Approximates lips to rim of cup.
inch) per month. Sits alone momentarily. Springs up and down when sitting. Turns completely over. Hitches (moves backward when sitting). Bangs table with rattle. Pulls to a sitting position. Chewing more mature. First solid food introduced. Approximates lips to rim of cup.
Social Behavior
7 Months
Physical Development
Social Behavior
Care and Guidance
8 Months
Physical Development


Social Behavior
Care and Guidance
9 Months
Physical Development
Care and Guidance
10 Months
Physical Development
Social Behavior
Care and Guidance
11 Months
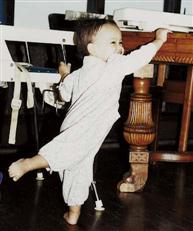
Physical Development
Stands upright holding onto an adult’s hand.
The 11-month-old can feed self finger foods and drink from a “sippy cup.”
Social Behavior
Care and Guidance
Sleep: Greets parents in morning with excited jargon.
Diet: Still spills from cup. Enjoys blowing bubbles.
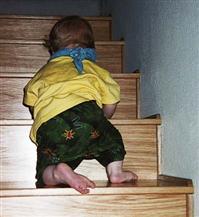
Exercise: Plays with toys in tub. Enjoys gross motor activity. Kicks, pulls self up.
12 Months
Physical Development

Social Behavior
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


