Nursing Care of Women with Complications After Birth
Objectives
1. Define each key term listed.
2. Describe signs and symptoms for each postpartum complication.
3. Identify factors that increase a woman’s risk for developing each complication.
5. Describe the medical and nursing management of postpartum complications.
6. Explain general and specific nursing care for each complication.
7. Compare and contrast mood disorders in the postpartum period.
Key Terms
atony (ĂT-ŏ-nē, p. 238)
curettage (KYŪ-rĕ-tăhzh, p. 240)
endometritis (ĕn-dō-mē-TRĪ-tĭs, p. 241)
hematoma (hē-mă-TŌ-mă, p. 239)
hypovolemic shock (hī-pō-vō-LĒ-mĭk shŏk, p. 236)
involution (ĭn-vō-LŪ-shŭn, p. 244)
mania (MĀ-nē-ă, p. 246)
mastitis (măs-TĪ-tĭs, p. 243)
mood (p. 245)
psychosis (sī-KŌ-sĭs, p. 245)
puerperal sepsis (pū-ĔR-pŭr-ăl SĔP-sĭs, p. 241)
subinvolution (sŭb-ĭn-vō-LŪ-shŭn, p. 244)
 http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Most women who give birth recover from pregnancy and childbirth uneventfully. However, some experience complications after birth that slow their recovery and may interfere with their ability to assume their new role. A woman can have any medical problem after a birth, but most complications related to childbirth fall into one of six categories:
Shock
Shock is defined as a condition in which the cardiovascular system fails to provide essential oxygen and nutrients to the cells. Postpartum shock related to childbearing include the following:
• Cardiogenic shock: Caused by pulmonary embolism, anemia, hypertension, or cardiac disorders
• Hypovolemic shock: Caused by postpartum hemorrhage or blood clotting disorders
• Anaphylactic shock: Caused by allergic responses to drugs administered
The inherent danger of obstetric shock is that body compensation can mask the signs until the condition becomes life threatening. The vigilance of the nurse can enable detection of early signs and then prompt intervention.
Hemorrhage
Postpartum hemorrhage occurs in about 4% of deliveries (Hacker et al., 2009) and is traditionally defined as blood loss greater than 500 mL after vaginal birth or 1000 mL after cesarean birth. Because the average-size woman has 1 to 2 L of added blood volume from pregnancy, she can tolerate up to these amounts of blood loss better than would otherwise be expected.
Most cases of hemorrhage occur immediately after birth, but some are delayed up to several weeks. Early postpartum hemorrhage occurs within 24 hours of birth. Late postpartum hemorrhage occurs after 24 hours and within 6 weeks after birth.
The major risk of hemorrhage is hypovolemic (low-volume) shock, which interrupts blood flow to body cells. This prevents normal oxygenation, nutrient delivery, and waste removal at the cellular level. Although a less dramatic problem, anemia is likely to occur after hemorrhage.
Hypovolemic Shock
Hypovolemic shock occurs when the volume of blood is depleted and cannot fill the circulatory system. The woman can die if blood loss does not stop and if the blood volume is not corrected.
Body’s Response to Hypovolemia
The body initially responds to reduced blood volume with increased heart and respiratory rates. These reactions increase the oxygen content of each erythrocyte (red blood cell) and faster circulation of the remaining blood. Tachycardia (rapid heart rate) is usually the first sign of inadequate blood volume (hypovolemia). The first blood pressure change is a narrow pulse pressure (a falling systolic pressure and a rising diastolic pressure). The blood pressure continues falling and eventually cannot be detected.
Blood flow to nonessential organs gradually stops to make more blood available for vital organs, specifically the heart and brain. This change causes the woman’s skin and mucous membranes to become pale, cold, and clammy (moist). As blood loss continues, flow to the brain decreases, resulting in mental changes, such as anxiety, confusion, restlessness, and lethargy. As blood flow to the kidneys decreases, they respond by conserving fluid. Urine output decreases and eventually stops.
 Safety Alert!
Safety Alert!
Because postpartum women often have a slow pulse rate, suspect hypovolemic shock or infection if the pulse rate is greater than 100 beats/min.
Medical Management
Medical management of hypovolemic shock resulting from hemorrhage may include any of the following actions:
• Giving intravenous (IV) fluids to maintain the circulating volume and to replace fluids
• Giving blood transfusions to replace lost erythrocytes
• Placing an indwelling (Foley) catheter to assess urine output, which reflects kidney function
Nursing Care.
Routine postpartum care involves assessing vital signs every 15 minutes until stable so that the signs of postpartum hemorrhage are identified as early as possible. The woman should be observed closely for early signs of shock, such as tachycardia, pallor, cold and clammy hands, and decreased urine output. Decreased blood pressure may be a late sign of hypovolemic shock. Routine frequent assessment of lochia in the fourth stage of labor helps identify early postpartum hemorrhage. When the amount and character of lochia are normal and the uterus is firm but signs of hypovolemia are still evident, the cause may be a large hematoma. Excessive bright red bleeding despite a firm fundus may indicate a cervical or vaginal laceration. The occurrence of petechiae, bleeding from venipuncture sites, or oliguria may indicate a blood clotting problem. In the first hours postpartum the perineal pad should be weighed to determine the output amount, with 1 g equaling 1 mL (see Chapter 9). Intake and output should be recorded and IV therapy monitored. Oxygen saturation levels are also monitored in early postpartum hemorrhage.
Careful explanations to the mother and family are essential, and providing emotional support and maintaining the integrity of the woman’s support system are key nursing roles. Even if the mother is separated from her infant, information concerning the infant’s condition should be readily accessible. Rooming-in should be established as soon as the woman’s condition permits.
Intensive care may be required to allow invasive hemodynamic monitoring of the woman’s circulatory status. Nursing Care Plan 10-1 specifies interventions for the woman at high risk for altered tissue perfusion related to hemorrhage.
10-1
 Nursing Care Plan
Nursing Care Plan
The Woman with Postpartum Hemorrhage
Patient Data
A woman is admitted to the postpartum unit. She appears anxious and frightened, and her lochia has saturated three perineal pads in the last hour.
Selected Nursing Diagnosis
Ineffective tissue perfusion related to excessive blood loss secondary to uterine atony or birth injury
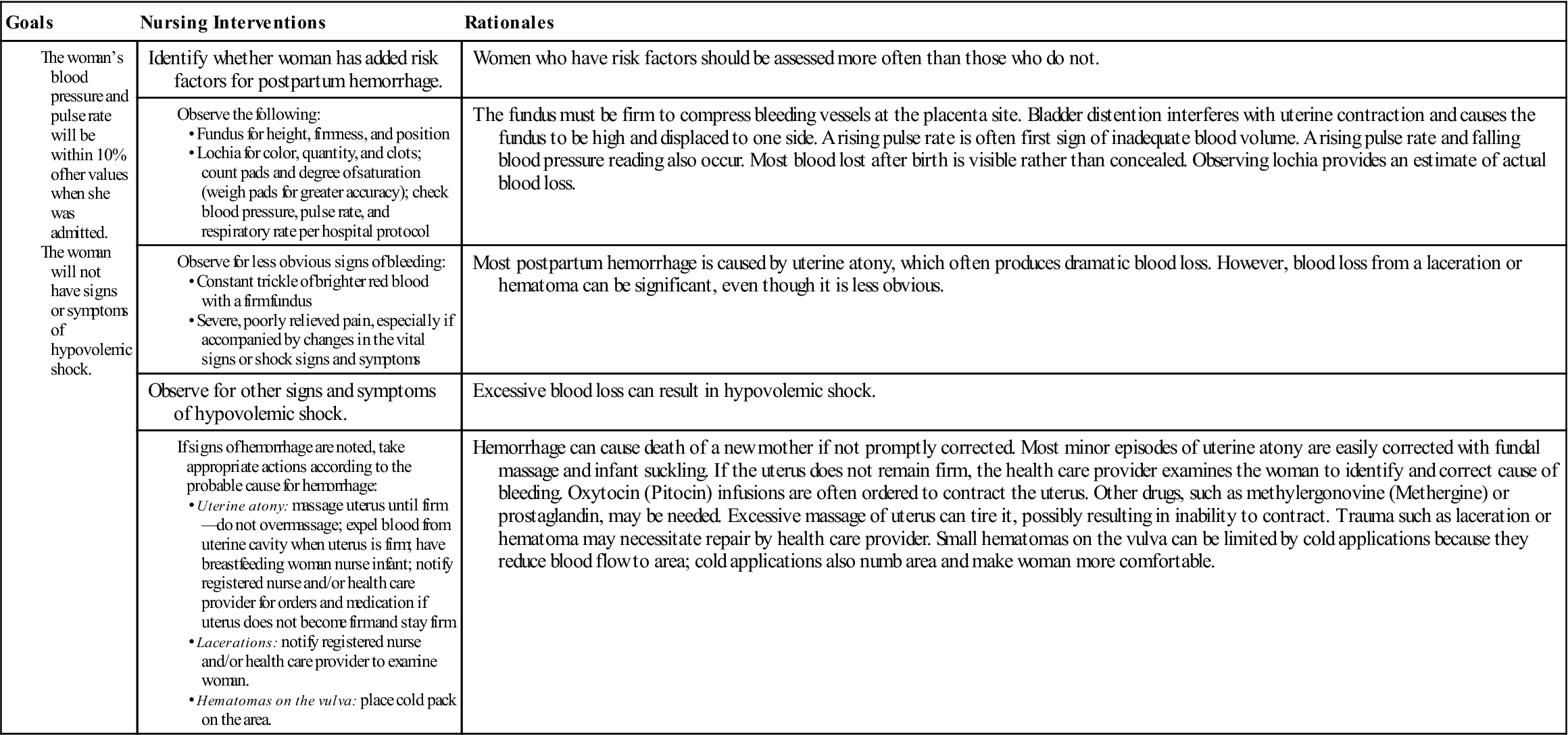
Selected Nursing Diagnosis
Fear, related to powerlessness

Critical Thinking Question
Anemia
Anemia occurs after hemorrhage because of the erythrocytes that are lost. Anemia resulting from blood loss occurs suddenly, and the woman may be dizzy or light-headed and is likely to faint. These symptoms are more likely to occur if she changes position quickly, particularly from a lying to an upright position. Until her hemoglobin and hematocrit levels return to near normal, she will probably be exhausted and have difficulty meeting her needs and those of her infant.
Iron supplements are prescribed to provide adequate amounts of this mineral for manufacture of more erythrocytes. Many health care providers have the woman continue taking the remainder of her prenatal vitamins, which usually provide enough iron to correct mild anemia.
Early Postpartum Hemorrhage
Early postpartum hemorrhage results from one of the following three causes:
Table 10-1 summarizes the types of early postpartum hemorrhage.
Table 10-1
Types of Early Postpartum Hemorrhage
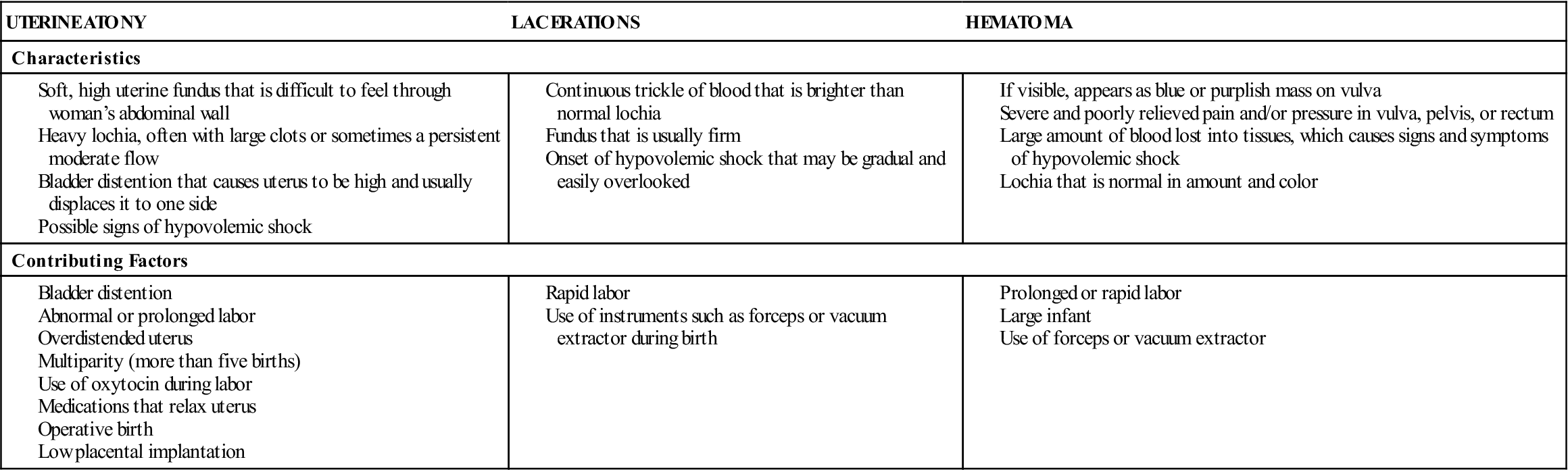
Uterine Atony
Atony describes a lack of normal muscle tone. The postpartum uterus is a large, hollow organ with three layers of muscle. The middle layer has interlacing “figure-eight” fibers. The uterine blood supply passes through this network of muscle fibers to supply the placenta.
After the placenta detaches, the uterus normally contracts and the muscle fibers compress bleeding vessels. If the uterus is atonic, however, these muscle fibers are flaccid and do not compress the vessels. Uterine atony allows the blood vessels at the placenta site to bleed freely and usually massively. Atony may be caused by uterine overdistention, retained placental fragments, prolonged labor, or use of drugs during labor that relax the uterus.
Normal Postpartum Changes.
After birth, the uterus should easily be felt through the abdominal wall as a firm mass about the size of a grapefruit. After the placenta is expelled, the fundus of the uterus is at the umbilicus level and then begins descending at a rate of about 1 finger’s width (1 cm) each day.
Lochia rubra should be dark red. The amount of lochia during the first few hours should be no more than one saturated perineal pad per 1 hour. A few small clots may appear in the drainage, but large clots are not normal.
 Nursing Tip
Nursing Tip
Perineal pads containing cold packs absorb less than regular perineal pads.
 Nursing Tip
Nursing Tip
To determine blood loss most accurately, weigh perineal pads before and after applying them: 1 g in weight equals about 1 mL in volume of blood lost.
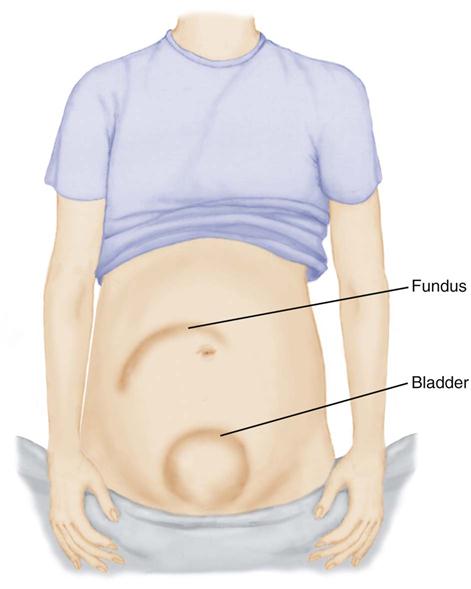
Characteristics of Uterine Atony.
When uterine atony occurs, the woman’s uterus is difficult to feel and, when found, it is boggy (soft). The fundal height is high, often above the umbilicus. If the bladder is full, the uterus is higher and pushed to one side rather than located in the midline of the abdomen (Figure 10-1). The uterus may or may not be soft if the bladder is full. A full bladder interferes with the ability of the uterus to contract and, if not corrected, eventually leads to uterine atony.
Lochia is increased and may contain large clots. The bleeding may be dramatic but may also simply be slightly above normal for a long time. Some lochia will be retained in the relaxed uterus because the cavity is enlarged. Thus the true amount of blood loss may not be immediately apparent. Collection of blood within the uterus further interferes with contraction and worsens uterine atony and postpartum hemorrhage. A woman who has risk factors for postpartum hemorrhage (see Table 10-1) should have more frequent postpartum assessments of the uterus, lochia, and vital signs.
Medical Management and Nursing Care.
Care of the woman with uterine atony combines nursing and medical measures. When the uterus is boggy, it should be massaged until firm (see Chapter 9), but it should not be overly massaged. Because the uterus is a muscle, excessive stimulation to contract it will tire it and can actually worsen uterine atony. If the uterus is firmly contracted, it should be left alone.
Bladder distention is an easily corrected cause of uterine atony. The nurse should catheterize the woman if she cannot urinate on the toilet or in a bedpan. Any clots or blood pooled in the vagina should be expelled by pressing toward the vagina after the uterus is firm. Most health care providers include an order for catheterization to prevent delaying this corrective measure. First the uterus is massaged to firmness, and then the bladder is emptied to keep the uterus firm.
The infant suckling at the breast stimulates the woman’s posterior pituitary gland to secrete oxytocin, which causes uterine contraction. A dilute oxytocin (Pitocin) IV infusion is the most common drug ordered to control uterine atony. Other drugs to increase uterine tone include methylergonovine (Methergine) or a prostaglandin such as carboprost. Methylergonovine increases blood pressure and should not be given to a woman with hypertension.
The health care provider may examine the woman in the delivery or operating room to determine the source of her bleeding and correct it. Rarely, a hysterectomy is needed to remove the bleeding uterus that does not respond to other measures. The woman should have nothing by mouth (NPO) until her bleeding is controlled.
 Safety Alert!
Safety Alert!
The woman who develops a hemorrhagic complication should be kept on NPO status until the health care provider evaluates her because she may need general anesthesia for correction of the problem.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


