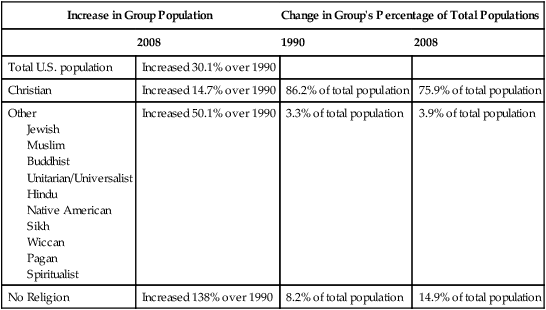
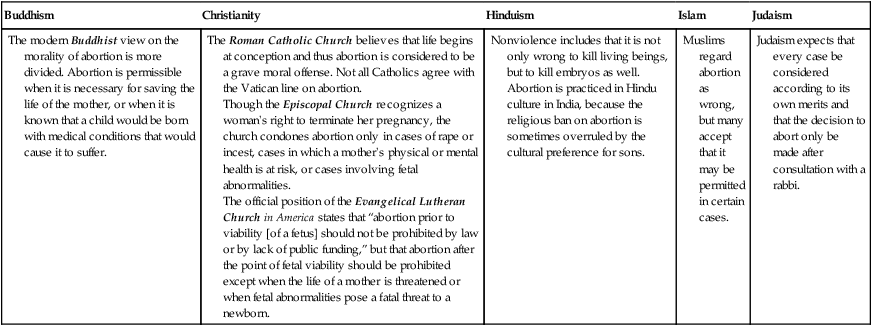
Cultural diversity in the workplace is a growing factor for health care in the United States, both for nurses and the patients and families they care for. More than 80 years ago, following the 1930 census, the U.S. Census Bureau reported that Whites made up 89.8% of the U.S. population (U.S. Census Bureau, n.d.a). By the time of the 1990 census, the White percentage of the U.S. population declined to 80.3% (U.S. Census Bureau, n.d.b). Following the 2010 census the U.S. Census Bureau reported Whites made up 75% of the U.S. population (U.S. Census Bureau, 2011a). Looking into the future, the Census Bureau estimates that “Minorities, now roughly one-third of the U.S. population, are expected to become the majority in 2042, with the nation projected to be 54 percent minority in 2050” (U.S. Census Bureau, 2008, p. 1). The Affordable Care Act of 2010 (ACA) will increase the diversity of patients seen in health care settings. In an amicus curiae brief filed with the U.S. Supreme Court before that court upheld the constitutionality of the ACA, the NAACP Legal Defense & Educational Fund, Inc., and others noted that “racial minorities are much more likely to be uninsured than whites… Latinos are the most likely to be uninsured, followed by African Americans” (U.S. Supreme Court, 2012, p. 10). The Kaiser Family Foundation further pointed out that minorities are much more likely to be uninsured than whites. “About one-third of Hispanics and nearly one-quarter of black Americans are uninsured, compared to 14% of non-Hispanic whites” (The Henry J. Kaiser Family Foundation, 2011, p. 11). The Kaiser report provided the following figures for nonelderly Americans lacking insurance coverage in 2010: The passage of the ACA, with its constitutionality subsequently upheld by the U.S. Supreme Court, results in the provision of insurance coverage to many previously uncovered Americans; and in the process it will also increase the proportion of non-Whites being able to seek and receive health care. Continuing change in demographics and insurance coverage heightens the importance of dealing with the growing cultural diversity in the workplace. There are two important elements to any workplace effectively dealing positively with the growth of cultural diversity: (1) increasing employee knowledge of other cultures, and (2) taking steps to eradicate ethnocentrism in the workforce. Ethnocentrism is defined as being “characterized by or based on the attitude that one’s own group is superior” (Merriam-Webster, 2012). From where does culture come? A culture can develop from characteristics such as those enumerated by the U.S. Department of Health and Human Services (USDHHS, 2003, p. 9). A culture can be defined by characteristics such as the following: • Length of residency in the United States • Perceptions of family and community • Perceptions of health, well-being, and disability • Physical ability or limitations However, when looking at areas from which cultural values are drawn, it is important not to assume that the criteria for a certain cultural group are true for every person who belongs to that racial, ethnic, or cultural group. Patients and/or their families, clinicians, and other individuals should not be put into restricted, culturally specific “boxes” nor labeled by virtue of culture and race. Learning cultural values requires moving beyond the group generalization to the individual’s specific values. History shows that the differences between the two extremes of any group are usually greater than the differences between the midpoint of two different groups. As President Obama said, “culture matters but that culture is shaped by circumstance” (Obama, 2006, p. 255). Henry (2012) gives an example about assuming that the criteria for a certain cultural group are true for every person in that group. He tells of the Dalai Lama reflecting on a trip he took to Israel and a discussion he had with one of the chief rabbis. When queried about what doctrine(s) united Jews all around the world, the rabbi responded that there wasn’t such a doctrine, and that in fact it was the rituals practiced by Jews that united them. Henry (2012) further noted the non-universality of doctrine in the Roman Catholic Church: “Whatever the few required tenets are that all Catholics must believe, certainly they do not include opposition to birth control, legalized abortion and gay marriage” (p. 1). There is a large percentage of Roman Catholic women, more than 90% according to some polls, who have practiced some form of birth control. He explained that “This figure is so high because many priests tell women in the confessional to follow their conscience on this issue” (Henry, 2012, p. 1). Workplace diversity for nurses encompasses not only their nursing colleagues and other health care workers. Just as importantly, it encompasses the patients and families the nurses work with. The U.S. Census (U.S. Census Bureau, 2011b) shows that not only is the nation changing to less and less of a White society, but also it is becoming less identified as a Christian society (Table 11-1). However, race and religion are just two of the things that factor into diversity. What really is diversity? TABLE 11-1 Religious Diversity in the U.S. Source: The 2012 Statistical Abstract, The National Data Book, U.S. Census Bureau, 2011b. In the mid twentieth century there was significant discussion about religious diversity in the United States. Roman Catholics were frequently denied equal treatment in social and cultural arenas. The election of John F. Kennedy as the first Roman Catholic President of the United States saw a significant reduction in the discrimination experienced by Catholics. The tragic events of September 11, 2001, not only resulted in nearly 3000 deaths but also saw an upswing in Muslim Americans being denied equal treatment in social and cultural arenas. Jews in the United States have experienced their own brand of discrimination, and Mormons and other religious affiliations have experienced theirs. The U.S. Census Bureau reported that religious diversity in the United States continues to increase (see Table 11-1) (U.S. Census Bureau, 2011b). It is interesting to look at why humans generalize or categorize so much when dealing with the “unique qualities” that the Vice President’s workforce diversity task force (1999) said “each of us possesses.” Some believe that the human mind generalizes because it cannot deal with a multitude of variables at the same time. Halford and colleagues (2005, p. 70) reported on a study where “the conceptual complexity of problems was manipulated to probe the limits of human information processing capacity… These findings suggest that a structure defined on four variables is at the limit of human processing capacity.” This is perhaps an explanation as to why the mind classifies things for us. However, such classification can lead to significant errors when the mind makes inferences about an individual from the group classification it has created. For example, Hilton (2007) provided an in-depth look at the positions of various religions on abortion (Table 11-2), demonstrating diversity and variance. TABLE 11-2 Data from Hilton, A. (2007). The different religions’ views on abortion. Retrieved from http://www.helium.com/items/716202-the-different-religions-views-on-abortion and The Pew Forum (2013) retrieved from http://www.pewforum.org/abortion/religious-groups-official-positions-on-abortion.aspx. Although followers of Roman Catholicism, Judaism, Protestant faiths, or Islam may hold given positions on abortion or contraception, many adherents of each faith undoubtedly practice something different than what their faith espouses. Those who generalize about Catholics being pro-life or anti-contraception would many times be wrong when applying those characteristics to individual Catholics. As an example, “nearly 70 percent of Catholic women use sterilization, the birth control pill or an IUD” according to a 2011 report from the Guttmacher Institute, the nonprofit sexual health research organization (Reuters, 2011, p. 1). At times it seems that most if not all of the “unique qualities” that the Vice President’s workforce diversity task force (U.S. Department of Commerce and Vice President Al Gore’s National Partnership for Reinventing Government Benchmarking Study, 1999) said “each of us possesses” can become a point of contention both between workers and between workers and those they care for. It is essential for nurses to understand those “unique qualities” of their co-workers and their patients/families as they seek to respond in a holistic way to the needs of those they are responsible for. • Diversity among patients (customers) • Diversity as applied by a diverse population of employees to a diverse population of patients • Application of basic principles of life that are often viewed and valued differently by individuals (both employees and patients) based on individual mores that frequently come from race, ethnicity, religion, and other diverse foundations. But these principles may vary more between individuals within a particular group than they do between groups.
Workplace Diversity

 http://evolve.elsevier.com/Huber/leadership/
http://evolve.elsevier.com/Huber/leadership/
BACKGROUND
Diversity of Employees and Patients
Increase in Group Population
Change in Group’s Percentage of Total Populations
2008
1990
2008
Total U.S. population
Increased 30.1% over 1990
Christian
Increased 14.7% over 1990
86.2% of total population
75.9% of total population
Other
Increased 50.1% over 1990
3.3% of total population
3.9% of total population
No Religion
Increased 138% over 1990
8.2% of total population
14.9% of total population
HISTORY
Buddhism
Christianity
Hinduism
Islam
Judaism
The modern Buddhist view on the morality of abortion is more divided. Abortion is permissible when it is necessary for saving the life of the mother, or when it is known that a child would be born with medical conditions that would cause it to suffer.
The Roman Catholic Church believes that life begins at conception and thus abortion is considered to be a grave moral offense. Not all Catholics agree with the Vatican line on abortion.
Though the Episcopal Church recognizes a woman’s right to terminate her pregnancy, the church condones abortion only in cases of rape or incest, cases in which a mother’s physical or mental health is at risk, or cases involving fetal abnormalities.
The official position of the Evangelical Lutheran Church in America states that “abortion prior to viability [of a fetus] should not be prohibited by law or by lack of public funding,” but that abortion after the point of fetal viability should be prohibited except when the life of a mother is threatened or when fetal abnormalities pose a fatal threat to a newborn.
Nonviolence includes that it is not only wrong to kill living beings, but to kill embryos as well. Abortion is practiced in Hindu culture in India, because the religious ban on abortion is sometimes overruled by the cultural preference for sons.
Muslims regard abortion as wrong, but many accept that it may be permitted in certain cases.
Judaism expects that every case be considered according to its own merits and that the decision to abort only be made after consultation with a rabbi.
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Nurse Key
Fastest Nurse Insight Engine
Get Clinical Tree app for offline access
